
Abstract
Abstract
Introduction:
Because neonatal jaundice remains one of the most commonly treated conditions of the newborn infant, it is important to assess the unintended consequences of treatment with phototherapy. The objective of this study was to evaluate whether treatment with phototherapy affects breastfeeding duration in newborns >35 weeks gestation.
Materials and Methods:
We analyzed data from the Infant Feeding Practices Study II. The exposure of interest was treatment of neonatal jaundice with phototherapy. The outcomes of interest were any breastfeeding through 12 months and exclusive breastfeeding through 4 months. Logistic regression models were developed to evaluate the association between the exposure and outcomes of interest. All models were adjusted for maternal age, race, education, household income, and gestational age, as well as for several potential markers of suboptimal breastfeeding.
Results:
Our study included 4,441 infants, of which 220 (5%) received phototherapy. We found no difference in the likelihood of any breastfeeding through 9 months of age, however, by 12 months, infants exposed to phototherapy were less likely to still be breastfed than those who were not exposed (adjusted odds ratio [aOR] 0.58, 95% confidence interval [95% CI] 0.37–0.92). Infants exposed to phototherapy were less likely to be exclusively breastfed throughout the first 4 months of life.
Conclusion:
Although phototherapy use did not substantially impact rates of any breastfeeding during the first year, it was associated with decreased rates of exclusive breastfeeding in the first 4 months of life. This suggests that we need to tailor messaging to mothers of infants receiving phototherapy to promote exclusive breastfeeding.
Introduction
T
Neonatal jaundice remains one of the most commonly treated medical conditions of the otherwise well newborn infant. 10 In 2009, the AAP released a revised set of guidelines recommending that all newborn infants be screened for jaundice before hospital discharge. This recommendation is in an effort to prevent the rare but devastating consequence of kernicterus. 11 Several studies following the new 2009 AAP guidelines have shown an increase in the number of infants receiving phototherapy for the treatment of jaundice, with one study finding that 7.6% of all infants receive phototherapy in the first few days of life. This has led to a decrease in the incidence of severe neonatal hyperbilirubinemia (serum bilirubin >25 mg/dL); however, it is unclear whether or not the increased screening and treatment of jaundice has led to fewer cases of kernicterus.12–16
Because it is not clear that increased screening and use of phototherapy are associated with a decreased incidence of kernicterus, it may be important to reassess current recommendations.12,17,18 Little is known about the potential harms associated with phototherapy. Nearly 30 years ago Kemper et al. reported on unintended harms of phototherapy, including decreased maternal–infant bonding, increased maternal anxiety, increase in the vulnerable child syndrome, and decreased rates of breastfeeding19–21 However, data collected by Kemper et al. during the 1980s may not be generalizable today. Since that time, national breastfeeding rates as well as hospital practices supporting breastfeeding have increased. 8 The purpose of this study is to determine if the association between treatment of jaundice with phototherapy and a shorter duration of breastfeeding continues to exist in a more recent cohort of infants.
Materials and Methods
Subjects and data collection
We conducted a cohort study analyzing data collected for the Infant Feeding Practices Study II (IFPS II). IFPS II was a survey conducted by the Centers for Disease Control and Prevention (CDC). Data from this survey are publicly available for analysis.
The methodology for IFPS II has been previously published. 22 For the IFPS II, ∼4,000 pregnant women were enrolled between May and December 2005. To maximize participation, the women were selected from a consumer opinion panel poll of roughly 500,000 US households with oversampling of women with lower education levels, and African American and Hispanic women. To continue in the study postnatally, participants must have given birth to a healthy, singleton infant of greater than 35 weeks gestation weighing at least 2.2 kg.
After enrollment, questionnaires were mailed to participants prenatally and then approximately once per month for the first 12 months of the infant's life. Questions were asked about breastfeeding intentions and practices, as well as infant formula use.
Inclusion and exclusion criteria
All infants for whom there were data in the IFPS II were evaluated for inclusion into our study. Infants were included if their mothers ever initiated breastfeeding. This was determined by those who answered “yes” to the question, “Did you ever breastfeed or try to breastfeed your baby, either in the hospital or birth center, or after you went home?” A small group of infants were excluded who indicated “other” treatment for jaundice, which included switching completely to infant formula.
Data collection
For the study, we abstracted information on maternal age, race and ethnicity, education level, marital status, and household income from the IFPS II. In addition, we obtained data on gestational age at birth, birth weight, and breastfeeding outcome at each study month. Maternal intention to exclusively breastfeed was determined by a question on the prenatal survey that asked, “What method do you plan to use to feed the baby in the first few weeks?” Answer options included “Breastfeed only (baby will not be given formula),” “both breast and formula feed,” “don't know yet,” and “formula feed only.” (There were a small percentage of women who prenatally intended to formula feed only, then initiated breastfeeding after the birth of their baby). This was then classified as a dichotomous variable with those who responded that they did not know yet which feeding method they would choose or those who had intended to exclusively formula feed considered as not having the intention to exclusively breastfeed. We also included data to determine use of supplemental infant formula on the first day of life and any breastfeeding problems the mother had during the first 2 weeks. This information was obtained from questions on the neonatal survey at ∼3 weeks of age. The first question asked “How old was your baby when he or she was first fed formula?” Response options included “1 day of life or less.” Breastfeeding difficulties encountered by the mother were determined from the question, “Did you have any of the following problems breastfeeding your baby during the first 2 weeks of breastfeeding?” This was followed by a list of 16 common breastfeeding problems. If a mother checked any of the responses, she was considered to have had a breastfeeding problem in the first few weeks of life (Appendix A1).
Outcomes
The primary outcomes of our study were any breastfeeding at 1, 2, 4, 6, 9, and 12 months of age. The secondary outcomes included exclusive breastfeeding at 1, 2, and 4 months of age. Exclusive breastfeeding at each month was determined based on the response to a survey item that asked which foods or drinks were given to the baby over the past 2 weeks. Data for exclusive breastfeeding in the past 4 months were not analyzed because the rate of use of complementary foods increased rapidly after this age.
Exposure
The main exposure of interest for our study was whether the infant received phototherapy for the treatment of jaundice in the newborn period. Exposure to phototherapy was determined by parental report on the IFPS II survey when a study infant was ∼3 weeks old. On this survey, parents were asked if their infant was ever jaundiced during the newborn period. If the answer was “yes,” the parent was asked to indicate if any treatment was required for the jaundice. One of the treatment options was phototherapy. All remaining infants whose parents did not indicate receiving phototherapy were considered unexposed.
Data on the presence of jaundice were missing for 42.2% of newborns who were included in the analyses, therefore making them ineligible to answer the question about phototherapy exposure. We assumed that virtually all mothers whose newborns received phototherapy would recall that their babies had been jaundiced when surveyed when the newborn was 3 weeks old. Therefore, we classified all those infants with missing information regarding the presence of jaundice as unexposed to phototherapy. To evaluate the validity of this assumption, we reanalyzed our study data after excluding newborns with missing information on the presence of jaundice.
Analysis
Logistic regression models were developed to evaluate the association between the dichotomous outcomes for both any breastfeeding and exclusive breastfeeding and exposure to phototherapy at each time point. All models were adjusted for the potential confounders of maternal age, race, maternal education, household income, and gestational age at birth. In addition, there are data to suggest that newborns who have breastfeeding problems during the first few days of life are more likely to develop significant hyperbilirubinemia than those who breastfeed well.23,24 Thus, it is possible that any decrease in subsequent breastfeeding after exposure to phototherapy might be related, in part, to breastfeeding problems before treatment rather than to the therapy itself. To account for this, we included markers of potentially suboptimal breastfeeding, including the mother's intention to exclusively breastfeed before birth, use of supplemental formula on day of life 1, and reported breastfeeding problems in the first 2 weeks of life in all of the regression models. Results were considered to be statistically significant if the 95% confidence interval (95% CI) around a calculated odds ratio (OR) did not include 1.0, or the p-value was <0.05.
This study was approved by the Seattle Children's Hospital Institutional Review Board.
Results
The IFPS II had an overall sample size of 4,902 infants. We excluded 461 infants because they were never breastfed. This yielded a study sample size of 4,441 infants. Of these, 1,098 (25%) were reported to have some degree of jaundice by their caregiver. A total of 220 (5%) study infants required phototherapy (Fig. 1). A further 205 infants were excluded from analysis because they indicated “other” treatment for jaundice. In our sample, 30% of women were still breastfeeding at 12 months of age and 27% were exclusively breastfeeding at 4 months. Table 1 outlines characteristics of the study population. Significant differences between the phototherapy exposed and unexposed groups were observed with regard to race, income, and level of maternal education. The infants in the phototherapy exposed group were of a significantly younger gestational age, 38.7 weeks compared with those in the phototherapy unexposed group, 39.4 weeks. Infants in the phototherapy exposed group were also significantly more likely to receive formula supplementation on day of life 1 than those in the phototherapy unexposed group, 25.5% compared with 15.4%.
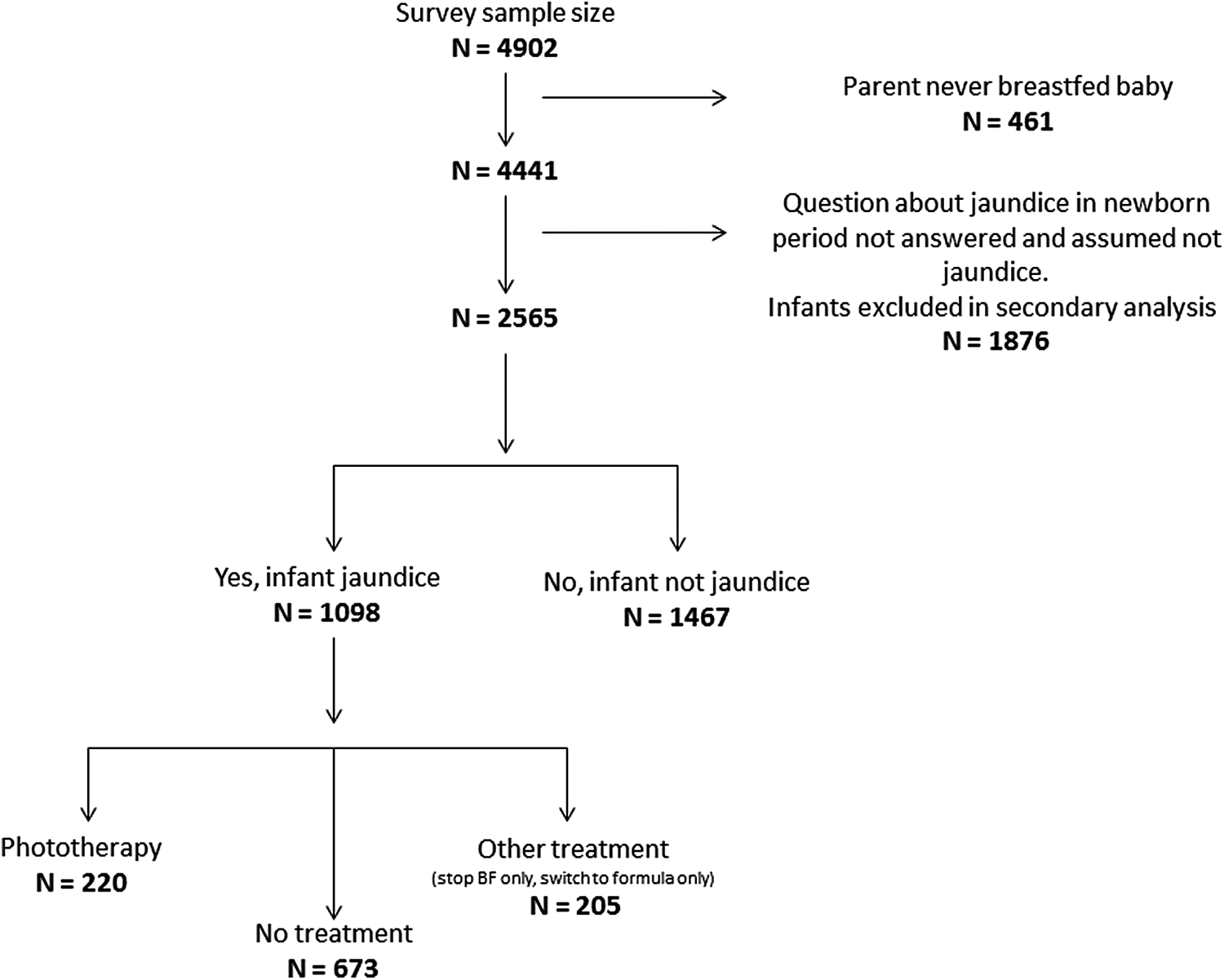
Study numbers and exposure categorization for study participants.
When evaluating any breastfeeding by month of age, there were no significant differences in the rates of any breastfeeding through 9 months of age among infants treated with phototherapy for jaundice compared to infants not exposed to phototherapy. At month 12, infants who were exposed to phototherapy were less likely to still be breastfed than infants who were not exposed to phototherapy (OR 0.58, 95% CI 0.38–0.87) (Table 2).
ORs based on logistic regression adjusting for maternal age, race, maternal education, household income, gestational age, prenatal intention to breastfeed, supplemental formula use on day of life 1, and breastfeeding problems in the first 2 weeks of life.
OR, odds ratio.
When evaluating exclusive breastfeeding by month, infants exposed to phototherapy were significantly less likely to be exclusively breastfed at all months than infants who were not exposed to phototherapy (Table 2).
A secondary analysis was done excluding all 1,876 infants who did not answer the question about whether neonatal jaundice was present. Results from this analysis were not substantially different from results obtained from including these mother–infant pairs in the analysis.
Discussion
The results of this study indicate that, among women who initiate breastfeeding, those whose infants received phototherapy were as likely to be receiving any breast milk through 9 months of age as those whose infants did not receive phototherapy. Only by 12 months of age were they less likely to be receiving any breast milk than their nonphototherapy exposed counterparts. However, we did find that phototherapy treatment was associated with decreased rates of exclusive breastfeeding throughout the first 4 months of life.
Our results are in contrast to the findings of Kemper et al., in which mothers of infants treated with phototherapy were nearly twice as likely to stop breastfeeding by 1 month of age. 19 In our cohort of infants, those exposed to phototherapy were as likely as those unexposed to be receiving breast milk through most of the first year of life. It is unclear what the significance is, if any, of the decreased breastfeeding observed at 12 months of age and this finding may be a statistical fluke. There are several possible explanations for why we did not observe the early abandonment of breastfeeding that Kemper et al. found. First, infants for the study by Kemper et al. were recruited from a single hospital compared to the national sample that we evaluated. There are significant regional differences reported in breastfeeding rates as well as hospital practices supporting breastfeeding. 8 It is therefore conceivable that breastfeeding counseling practices and even maternal motivation to continue breastfeeding could have been different among this population than the more nationally representative population in our study. In the study by Kemper et al., all phototherapy was done in an in-patient setting. In our study, it was not possible to know if an infant was treated with hospital-based or home-based phototherapy. Prior studies have shown that home-based phototherapy appears to be less detrimental to duration of breastfeeding than hospital-based phototherapy. 25 The use of home phototherapy among participants in our study may have attenuated any negative effects on breastfeeding rates. Last, the Kemper et al. study was done nearly 30 years ago. It is likely that much of the observed difference in study findings is due to greater breastfeeding support and encouragement in our newborn nurseries, hospitals, and in outpatient settings, as well as the overall increase in breastfeeding rates, especially marked in non-white populations, now than was practiced 30 years ago. 26
We did find a significant decrease in rates of exclusive breastfeeding among phototherapy exposed infants during the first 4 months of life. This finding suggests that, although the mothers of infants treated with phototherapy are offering at least partial breast milk feeds at similar rates to mothers of infants who do not require phototherapy, they are more likely to be supplementing with formula through the early months of life. This may be due to breastfeeding-related messaging parents receive from healthcare professionals while their infants undergo treatment for jaundice. Our speculation is that mothers of jaundiced infants may internalize the message from providers (either spoken or unspoken) that their breast milk is not enough for the baby and either begin or continue to supplement their infant with formula.
There are several limitations to this study. First, the data are now several years old and were not collected for the purpose of answering this question. However, there are no more recent data of such a large sample of women that address this issue that we are aware of. Also, all data obtained rely on parental report. Although it is likely that parents would remember whether or not their newborn required phototherapy and how the infant was fed over the previous 1–2 months, undoubtedly this recall is not perfect. We believe the main limitation of this study is the difficulty in determining whether early cessation of breastfeeding, or the decrease in exclusivity of breastfeeding, was related more to breastfeeding problems before, rather than caused by, phototherapy. Prior studies have demonstrated an association between inadequate breastfeeding and neonatal jaundice.23,24,27 In a study by Bertini et al., breastfed infants who required formula supplementation for excessive weight loss were significantly more likely to have an elevated serum bilirubin level (>12.9 mg/dL) than either those infants who were exclusively formula fed or exclusively breastfed. 23 This led the investigators to conclude that breastfeeding per se is not associated with elevated serum bilirubin levels, but rather inadequate breastfeeding with associated fasting and dehydration. Our results also show that infants exposed to phototherapy were of a younger gestational age than those who were not. Because prematurity, or being born at an earlier gestational age, is associated with both the need for phototherapy and breastfeeding problems, it is difficult to determine if exposure to phototherapy is what led to the subsequent decrease in exclusive breastfeeding. We tried to account for early breastfeeding inadequacy by assessing possible markers of breastfeeding problems such as gestational age, formula supplementation, maternal report of early breastfeeding problems, as well as the mother's overall motivation for exclusive breastfeeding assessed before the birth of her child. Given that the phototherapy group had greater intention to breastfed, but also greater formula use in the first 24 hours of life, this could suggest there were early breastfeeding difficulties that were not completely accounted for in our models.
Conclusion
It is encouraging that increased vigilance about neonatal jaundice, with the concomitant increase in phototherapy use, does not seem to be leading to a significant decrease in the duration of any breastfeeding. However, it is concerning that the use of phototherapy was associated with a decrease in the rate of exclusive breastfeeding through the first 4 months of life, as there is evidence that the benefits of breastfeeding are maximized when there is no use of infant formula.2,28,29 This result suggests that communication related to exclusive breastfeeding in a child receiving phototherapy may need to be evaluated to ensure that, as much as possible, exclusive breastfeeding is supported in newborns receiving phototherapy who are not in need of extra fluid for hydration, thereby preserving a mother's confidence in her ability to exclusively breastfeed after treatment is completed.
Footnotes
Disclosure Statement
W.M.W. has no financial disclosures. Dr. Taylor is co-owner of BiliCam, LLC, a company that is developing a noninvasive method to measure bilirubin levels in newborns. He currently derives no income from the company.
| Did you have any of the following problems breastfeeding your baby during your first 2 weeks of breastfeeding? My baby had trouble sucking or latching on.….….….….….. |
I didn't have enough milk .….….….….….….….… | ||
| My baby choked.….….….….….….….….….….….….….….….…. | My nipples were sore, cracked, or bleeding.… | ||
| My baby wouldn't wake up to nurse regularly enough.….. | My breasts were overfull (engorged).….….….. | ||
| My baby was not interested in nursing.….….….….….….….. | I had a yeast infection of the breast.….….….… | ||
| My baby got distracted.….….….….….….….….….….….….….. | I had a clogged milk duct.….….….….….….….… | ||
| My baby nursed too often.….….….….….….….….….….….…. | My breasts were infected or abscessed.….…. | ||
| It took too long for my milk to come in.….….….….….….…. | My breasts leaked too much.….….….….….….. | ||
| I had trouble getting the milk flow to start.….….….….….…. | I had some other problem.….….….….….….….. | ||
| My baby didn't gain enough weight or lost too much weight ….….….….….….….….….….…. | I had no problems ….….….….….….….….….…. |