
Abstract
Abstract
Background:
The use of breast pumps with a compression component has shown their higher efficacy compared with vacuum pumps. However, the direct role of the compression stimulus is not sufficiently proven in the removal of milk from the main milk ducts of the breast. The aim of this study was to determine the contribution pulsating compression component of the breast pump has on total volume milk ejection by vacuum and compression stimuli.
Subjects and Methods:
Twenty-four lactating women of 21–30 years of age, who volunteered to be included in this study, were examined. Experimental breast pump with vacuum and compressive components were used to express breast milk.
Results:
It was found that volume milk ejection together with vacuum and compression stimuli was 10–46% more than expressing only with vacuum stimuli. Average values were 40.5% ± 5% for expression only with vacuum stimuli and 59.5% ± 5% for expression with vacuum and compression stimuli.
Conclusions:
Compression stimuli increased the efficacy of the breast pump, which is not only due to the effective formation milk ejection reflex but also directly to an additional squeezing of milk from the breast.
Introduction
B
In Russia, there are currently two types of breast pump used in medical practice. The first type (“Ameda®,” “Medela®,” AVENT®”) applies only vacuum stimuli, while the second type of pump (“Lactopulse®” and “Perun®”) applies both vacuum and compression stimuli to the areola and the nipple, similar to removal of milk by an infant.3–5 When applying vacuum on the areola, it expands the areola and stimulates the stretch cutaneous receptors. On the contrary, compression of the areola stimulates the tactile mechanoreceptors. This simultaneous activation of areolar mechanoreceptors is likely to establish lactation in the most efficient way. Besides, compression of the main milk ducts, which lie under the areola, ensures more successful milk ejection. As the clinical research and breastfeeding practice show, this type of breast pump promotes more efficient milk ejection compared to the vacuum-type breast pumps. 6 Nevertheless, the interpretation of the research findings on assessing the compression stimuli in milk ejection was challenged by a number of factors. In particular, as extensive research show, physiological and psychological state of the woman can dramatically influence milk ejection in a 24-hour period. 7 Evidently, to assess the difference in the volume of the ejected breast milk, it is necessary to express milk by simultaneously applying vacuum and compression stimuli during the same session. Mechanical stimulation of mechanoreceptors of the areola releases oxytocin from the central nervous system into the bloodstream, which produces periodic increases in the intraductal mammary pressure.8,9 These serve to increase the rate of milk ejection regardless of the milk removal technique. Evidently, it is difficult to comparatively evaluate the effects of vacuum and vacuum–compression stimuli in milk ejection.
The primary aim of the article is to work out the method that allows us to reveal the difference in volume of milk expressed by applying purely vacuum and by applying vacuum–compression stimuli in relation to changes in intraductal pressure. This method will allow us to assess how the compressive force imposed on the mammary glands directly correlates with the volume of expressed milk.
Subjects and Methods
The study was conducted at the postnatal unit of the D.O. Ott Institute of Obstetrics and Gynecology, St. Petersburg, Russian Federation. Twenty-four lactating women of 21–30 years of age, who volunteered to be included in this study, were examined. Women had been lactating and breastfeeding normally for between 5 and 6 days. Twenty of them were primiparous breastfeeding mothers and four were multiparous mothers. Next, for control purpose, in six women for milk ejection, we applied only vacuum stimuli of 120–140 mm Hg, which was identified as optimal to reduce breast pain, according to a number of studies. Four of them were primiparous breastfeeding mothers and two were multiparous mothers. Infants of all patients were exclusively breastfed. The informed consent of the women was obtained according to the Declaration of Helsinki. The study was approved by the Ethics Committee D.O. Ott Institute of Obstetrics and Gynecology, RAN, Russia.
Our previous experiments suggest that during milk ejection with a breast pump that employs compression stimuli,8,10 pressure in the ducts is created by the milk ejection, but the pressure varies, being at its peak 1.5–2 minutes after the start of feeding. At peak pressure, suction alone removes milk faster than suction plus compression. At all other times, when ductal pressure is not at its peak, suction + compression results in faster milk release.
To reduce the effect of intraductal pressure, we minimized the length of intervals between the consecutive vacuum stimuli and vacuum–compression stimuli. Ideally, the vacuum stimulus should repeatedly occur in turn with a vacuum–pressure stimulus. In practice, however, we faced some challenges owing to the inadequacies of the switching module regulating the milk stream into the different milk collection containers. According to the tentative experiments, each session comprises a number of sequences of four consecutive vacuum stimuli followed by four simultaneous vacuum–compression stimuli (Fig. 1B).

The removable cup
A commercially available, software-controlled electric breast pump (Lactopuls) with both vacuum and compression stimuli was modified to conduct experiments. Experimental breast pump that applies compressive force comprises a control unit and a removable cup that is placed on the mammary gland. Figure 1A is a removable cup. The cone-shaped cup (2) made from transparent silicon rubber fits a mammary gland (1) to transfer the milk flow from the breast into the silicon milk collection tube (3), which is further divided into two horizontal tubes (4, 5) connected with the milk collection containers (a, b). The horizontal tubes have one side contacted with the rigid plate (6) and the other side contacted with the wedge-shaped pistons (7) of the pneumatic pistons (8, 9). Either one of the horizontal tubes can be closed off by an electronically operated pneumatic piston, thereby diverting milk to the left or right. The pistons gate the flow of extracted milk, to either the left (b) or right (a) collecting bottles, equating to the milk collected during suction alone, or suction + compression, allowing them to be measured separately at completion of the session. Through the electric pneumatic valves, the breast pump system generates a vacuum into the milk collection containers, through the tubes (10), to carry vacuum to the elastic cone-shaped cup through horizontal tubes (4, 5) and the milk collection tube (3).
There are two components of the experimental breast pump, which are mechanically driven by electronically operated pneumatic pistons to apply positive pressure (i) to the mechanical levers (12) applying pressure to the areola (13); and (ii) to the horizontal tubes (4,5) of the collecting system, diverting milk either to the left or the right, as a function of whether suction alone, or suction and pressure is being applied.
The system operates as follows: when the system is switched on, the system generates periodic vacuum in the milk collection containers at a frequency of one cycle per second with a duration of 0.5 seconds. Besides, it creates regular pressure stimuli in to the pneumatic pistons (8, 9) with a duration of 4 seconds and amplitude of 40 kPa, which at regularly occurring intervals do not allow milk flow as well as vacuum to pass through the horizontal tubes. In particular, if the tube connected to the milk collection container (b) is constricted, the vacuum draws breast milk into the milk collection container (a). Simultaneously, the system cycles causing pressure to be applied by the levers (12) at a frequency of one cycle per second with a duration of 0.27 seconds (Fig. 1B), which compress the areola and may activate additional milk outflow. After 4 seconds, the tube connected to the milk collection container (a) is constricted and only the vacuum draws milk into the milk collection container (b) as the system ceases to generate pressure in the two-membrane pneumatic piston (17) by pressing the levers (12). This cycle is repeated in a rhythmic pattern described as above. In a vacuum–compression sequence, compression occurs in impulses occurring at 0.23-second intervals after the vacuum stimulus and ceases simultaneously with the vacuum stimulus (Fig. 1B). Amplitude of vacuum stimuli was 120–140 mm Hg and pressure stimuli 0–40 kPa. The movement of each of the ends of the levers (12) in contact with the areola of the breast (Fig. 1) at maximum pressure in the two-membrane pneumatic piston (17) was about 12 mm.
Results
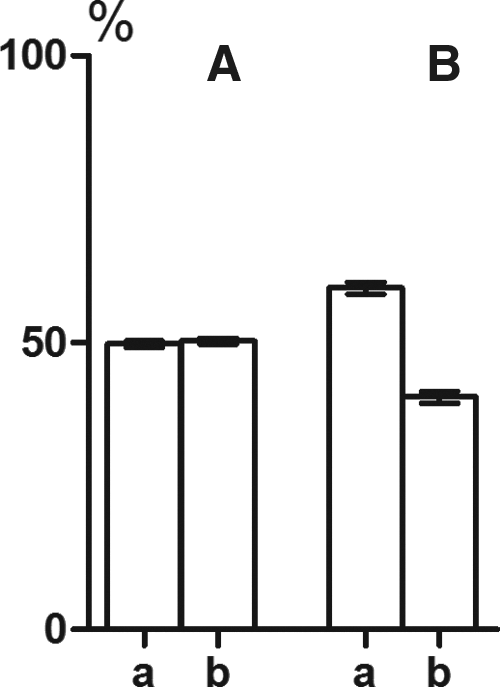
Before the research, we conducted experiments on drawing water from the vessel, which was set to maintain constant water level, to verify whether the systems (a) and (b) show symmetry in collecting the breast milk. To this end, into the cone-shaped cup, there was inserted a plug with a tubule of 1 mm in diameter that allows the flow of water from the vessel into the container. When the vacuum stimuli of 120 mm Hg were switched on, the milk collection containers, each in turn, drew water successively during 4 seconds. After 5 minutes, the milk collection containers received the same volume of milk, which proves that systems show symmetry in collecting milk. Next, for control purpose, in six women for milk ejection, we applied only vacuum stimuli of 120–140 mm Hg. The volume of milk expressed into the different milk collection containers (Table 1) was assessed in percentage proportion in relation to an overall volume of the expressed milk. Referring to Figure 2A, the histogram shows the volume of expressed milk in the milk collection containers (a) and (b). The volume of expressed milk in the milk collection containers (a) equals 49.75% ± 0.51%, while in the milk collection containers (b) 50.25% ± 0.51% (difference was insignificant: p ≤ 0.05), that is, two milk collection containers accumulated the same volume of milk.
The amount of milk in the milk collection containers and extracted by vacuum and together by vacuum and compression in percent to the total amount of milk.
l, left breast; r, right breast.
Furthermore, when consecutively using vacuum and vacuum–compression ejection modes of operation, in 24 women, the volume of expressed milk tends to be higher compared to the volume of expressed milk when using only vacuum mode of operation (Table 2). Among 24 women, there was only one case that made an exception, when the volume of the expressed milk was the same. The difference in the volume of expressed milk varied between 10% and 46%. In addition, according to Figure 2B, the volume of expressed milk equals 40.5% ± 1.03% at vacuum milking and 59.5% ± 1.07% at vacuum–compression milking. As our observations revealed, this difference in the volume of expressed milk can be attributed to the morphology of the mammary glands and their functional state at milk ejection. In the case of exception, that is, the expressed milk volume was the same when using vacuum and vacuum-compression modes of operation, milk drips from the gland quite freely and easily. Through a transparent cover plate (1), Figure 1, it was seen that vacuum of an amplitude twice as little as recommended, that is, 60–70 mm Hg, caused milk expression. This type of mammary glands can be defined as “Type I.” Concerning the other type of mammary glands, during the first minute of pumping, milk ejection was triggered only by applying vacuum–compression stimuli. Furthermore, as reflex pressure increases in the alveolar duct system, milk outflow can be produced by vacuum only. When using vacuum mode of operation, the milk flow rate and volume of expressed milk tend to be lower compared to the vacuum–compression mode of operation. This type of mammary glands can be defined as “Type II.” When using vacuum–compression method, compression of areola increases the volume of expressed milk. At the amplitude of compression stimuli adopted for this research, women could feel the rhythmic compression of areola, but they did not experience pain in breast. Since the examination period (5–6-day) correlated with the lactogenesis, high-altitude alveolar edema was reported in several women. As an increase in compression amplitude produced pain in the breast, the compression amplitude was relatively lower in the session, which probably led to a decreased milk volume.
Discussion
To express milk from the mammary gland, it is necessary to create the difference between the alveolar duct pressure and atmospheric pressure. In this case, milk outflow is facilitated by an increase in positive pressure in the mammary ducts in the areola by applying compressive force. This method is used in manual milk expression. Reducing the pressure in the area surrounding the nipple and areola below atmospheric increases the pressure difference between alveolar duct capacitive system and the external environment surrounding the nipple and part of areola. This method is used in the vacuum breast pumps.
The difference in pressure may be created by simultaneously exerting positive pressure and vacuum, which simulates the letdown by an infant. All in all, a reflex increase in pressure in the alveolar duct system is a prerequisite for the all three milk expression techniques, as the mammary alveoli, thin and medium ducts, contain ∼95% of breast milk, which significantly impede milk flow when applying both positive pressure as well as vacuum. According to ultrasound images, 6–14 mammary ducts radiate from the nipple, with the maximum duct diameter of 1–5 mm9 at the distance of 8–9 mm from the nipple. Through these ducts of 1–5 mm in diameter, it is quite easy to remove or express milk. Even so, ∼2–3 mL of milk is accumulated in the main milk ducts and it takes less than a minute for an infant or a breast pump to remove it from the breast. As a result, at breastfeeding or breast pump removal, myoepithelial cells in the alveolar duct system should reflexly “supply” milk in these parts of the mammary ducts. Notably, the milk ducts of the nipple show higher resistance to milk flow. In particular, in the nipple, the mammary ducts become milk ducts in the nipple and measure ∼5–10 times as narrow, 11 with the diameter of the milk ducts varying along the nipple. At the nipple tip (1 mm from the tip), the ducts are the smallest in diameter and measure ∼0.1 mm. Typically, toward the orifice, the ducts tend to become conical in shape and measure 1.5–2 times as wide in diameter. Further inside the nipple (3.5–4 mm from the nipple tip), the ducts become wider in diameter and measure 0.6–0.8 mm. Then, the diameter of the ducts become narrow again and measure at least ∼0.4 mm.12,13 As resistance to the liquid outflow in the tube is inversely proportional to its cross section, the nipples with the narrow milk ducts impede milk outflow. This type of mammary glands can be identified as “Type II.”
In the first 4 days postpartum, the mammary ducts contain colostrum of high viscosity compared to transitional and mature milk, and milk ejection, therefore, may be challenged. The resistance to milk outflow can be overcome by a further increase in intraductal pressure, in particular, by imposing more vacuum. Nevertheless, as clinical studies revealed, high vacuum can cause nipple pain, which fails to facilitate the milk-ejection reflex by blocking the release of oxytocin and, consequently, impedes milk outflow from the breast. To overcome the problem, Morton in her research 14 applied compression with a relatively low vacuum. It appears that simultaneous use of the breast pump with manual areola compression facilitated colostrum outflow.
Vacuum–compression mode of operation seems to be more efficient in milk ejection. 8 Referring to Figure 1A, the breast pump system is redesigned as to allow to independently assess the role of compression stimuli in milk rejection. As studies revealed, when using compression method, there is an up to 46% increase in the volume of milk expressed from the breast, notably from the “Type II”; furthermore, it facilitates extracting colostrum during early lactation. The amplitude of compression stimuli correlates with the volume of milk expressed from the breast. Seemingly, in the case of dense or swollen areola, compression stimuli were applied to the mammary ducts beneath the areola in less force so that compressive force contributed less to milk ejection. Importantly, the breast pumps that applied compressive force had a further advantage over a vacuum-driven system to reduce areola density. As this research and other recent studies 15 have shown, during milk ejection, the massage of areola by compression stimuli may reduce the areola density, so compression against areolar ducts facilitates the outflow of milk accumulated within the glands.
Compressive force may be less important in expressing milk from “Type I.” If so, main milk ducts in the nipple, presumably, had a maximum diameter of 0.6–0.8 mm and it was vacuum, rather than compression, which was applied first to express substantial volume of breast milk. Interestingly, the research on how an infant sucks milk out of the bottles for formula feeding with the nipples of various orifice diameters 16 have practically the same results. In particular, an infant exerted maximum compression with the tongue and gums on the nipples of a small orifice diameter. When the bottle with the nipple of a small orifice diameter was placed in a vertical position, water drips at the speed of 0.04 mL/second. If the speed reaches the value of 0.1 mL/second due to a bigger diameter orifice of the nipple, an infant produces considerably less compression.
Conclusion
The research findings show that compression stimuli increase efficacy of the breast pumps not only due to effective stimulation of the mechanoreceptors of the mammary glands for effective formation of the milk-ejection reflex but also directly by an additional squeezing of milk from the breast. The method described above may be extrapolated to assess the efficacy of the breast pumps of various designs.
Footnotes
Acknowledgment
This study was supported by grant 29690 from St. Petersburg University.
Disclosure Statement
No competing financial interests exist.