
Abstract
Abstract
Background:
Breastfeeding counseling has been shown to increase the initiation and duration of breastfeeding. The American Congress of Obstetricians and Gynecologists calls for all healthcare workers to educate and encourage women to choose breastfeeding. Despite these recommendations, the reported incidence of prenatal breastfeeding discussions varies widely. Lack of physician education has been speculated to be one of the contributing factors.
Objective:
To assess the impact of a breastfeeding educational intervention on the knowledge and counseling behaviors of OB/GYN resident physicians.
Study Design:
Resident physicians in a university-based OB/GYN program were given two lectures on the benefits of breastfeeding and common lactation issues. The residents completed a knowledge test before and after the educational intervention. Resident behaviors were assessed through patient surveys after the initial prenatal visit (n = 79 and n = 81 before and after the educational sessions, respectively). The responses were then analyzed by comparing binomial proportions before and after the intervention.
Results:
Patient surveys showed that the educational intervention resulted in statistically significant increases in the rate of general discussion from 62% to 79% (p = 0.017) and discussion of breast changes that occur during pregnancy from 41% to 57% (p = 0.037). There was a positive trend for breastfeeding promotion from 58% to 72% (p = 0.08) and for breast exams from 42% to 56% (p = 0.08). The median score on resident's knowledge assessment test increased marginally from 20 to 20.5 out of 28 questions after the educational intervention.
Conclusion:
Our study showed that a brief educational intervention on breastfeeding had a meaningful impact on OB/GYN resident physician counseling behavior.
Introduction
A
In this prospective observational study we assessed the extent and quality of OB/GYN residents' counseling on breastfeeding through patient surveys filled out immediately after the initial prenatal visit. We hypothesized that after two lectures on breastfeeding given two months apart, not only would residents' knowledge on the subject improve, but also the surveys would reflect an overall increase in breastfeeding promotion, as well as more detailed discussions on the benefits of breastfeeding.
Materials and Methods
Subjects and setting
Forty-three residents in the Obstetrics/Gynecology training program at the Ohio State University/Mount Carmel Health System were eligible to participate. The outpatient resident clinic took place at a large academic center caring for a predominately Medicaid population in Ohio.
All residents and patients took part in the study voluntarily. Verbal consents were obtained before the study questionnaires and surveys. Data were analyzed collectively without individual identification of subjects. Approval for the study was granted by the Ohio State University Institutional Review Board.
Educational intervention
A faculty member in Obstetrics and Gynecology gave the residents two 1-hour lectures 8 weeks apart. Lectures covered topics on current statistics, breastfeeding benefits, recommendations on breastfeeding promotion, evaluation of position, and latch in addition to basic breastfeeding problem solving. The lectures had significant overlap in information, but were presented in different formats. First was a PowerPoint presentation during department grand rounds and the second was a resident didactic lecture with videos and team Jeopardy.
Measures
Resident knowledge about breastfeeding was assessed using the previously validated pretest questions from the Wellstart International (2013) Lactation Management Self-Study Module. 9 The first questionnaire was given before the first lecture, and the same questionnaire was given again 7 weeks from the last lecture, 15 weeks from the initial test date to assess long-term information retention.
To assess the resident's breastfeeding counseling behavior, patients who presented for their initial prenatal visit at the resident clinic during the study period were approached, and if interested, completed a survey immediately after their visit. Initial prenatal visits were booked as a 30-minute visit on the schedule. The survey was written at the third-grade reading level and aimed to determine the extent and detail of breastfeeding discussion during the visit (Table 1). Patients requiring a translator during the initial prenatal visit were excluded as all surveys and consents were in English. A total of 160 surveys were collected, 79 were collected over a period of 12 weeks before the first lecture and 81 were collected over a period of 15 weeks after the second lecture. During the study period 12 out of the 43 residents covered the initial prenatal clinic visits after the educational interventions. Out of these 12 residents, 9 residents attended both lectures and 3 residents attended one lecture. The residents did not know that the patients were going to be surveyed. The size of the sample population was based solely on time and money constraints of the study itself and not on any calculation of study power.
Statistical methods
The change in resident knowledge about breastfeeding after the intervention was analyzed using Wilcoxon signed-rank test. Data on resident counseling behaviors gathered from patient surveys were analyzed by comparing binomial proportions before and after the intervention. The difference in proportions, before and after the educational program was calculated and the Wald asymptotic confidence limits for the difference were presented. A two-sided significance level of α = 0.05 was used for all tests and are unadjusted for multiple comparisons. All analyses were carried out in SAS version 9.4 (SAS Institute, Cary, NC).
Results
In the before-intervention group, 18 resident questionnaires were collected and 17 questionnaires were used for analysis (1 questionnaire was discarded because only one side of the double-sided pages were filled out); in the after-intervention group, 27 questionnaires were collected and 26 questionnaires were used for analysis (1 questionnaire was not included for analysis because the resident was not present for either lecture). Out of the 26 residents who completed the questionnaires in the after-intervention group, 14 (54%) attended both lectures and the rest 12 (46%) attended at least one lecture. After attending the breastfeeding lectures, residents' median score increased marginally to 20.5 [range: 16–24; mean: 20.7 (2.3)] correct answers for 28 breastfeeding knowledge questions, compared with their knowledge score at baseline median 20 [range: 9–22, mean: 18.9 (3.4); p = 0.15 from Wilcoxon signed-rank test].
Changes in resident counseling behaviors after the educational intervention are shown in Figures 1 and 2. The patient surveys showed a significant increase in the general discussion of breastfeeding (17% increase [95% CI: 3.1–31%, p = 0.017]) and breast changes that occur during pregnancy (16% increase [95% CI: 1.0–32%, p = 0.037]). There was a positive trend for breastfeeding promotion from 58% to 72% (p = 0.08) and for breast exams from 42% to 56% (p = 0.08). Discussion on specific benefits of breastfeeding did not show any significant change.

Resident performance on general topics. Percentage of residents asking/performing each task before and after the educational intervention. *denotes statistical significant p < 0.05.
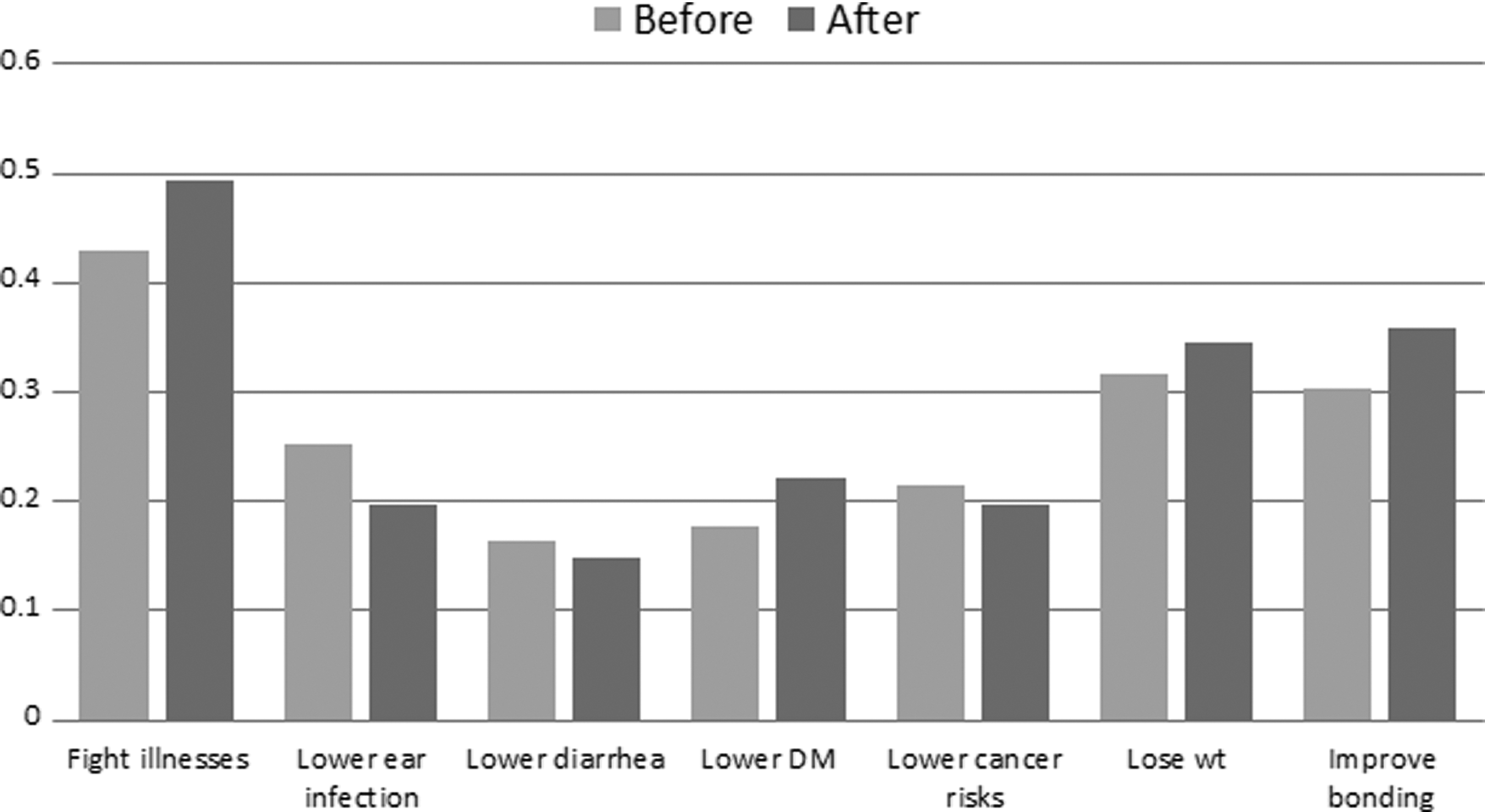
Resident counseling on specific benefits of breastfeeding. Percentage of residents discussing each benefit before and after the educational intervention. DM, diabetes mellitus.
Discussion
Antenatal breastfeeding education and promotion has been demonstrated to be effective in improving the rate of breastfeeding initiation and continuation especially among low-income women.10–13 However, in comparison to nurse midwives, studies have shown that discussions by physicians are infrequent (15–29%),2,14,15 brief, and generally lacking in clear support of breastfeeding. 2 Deficiency in residency training curricula on breastfeeding has frequently been cited as a contributor to this problem3–8,16 leading to a lack of knowledge and confidence in providers. Fortunately, studies have also shown that short educational sessions are effective in improving provider breastfeeding knowledge and skills.8,17–19
In this study, we demonstrated a positive change in patient perceived resident breastfeeding counseling behavior after only two educational sessions. Resident knowledge as assessed by a previously validated questionnaire showed a small, nonstatistically significant increase.
In contrast to previous studies that focused on assessment of provider knowledge or skills before and after an educational session, our study focused on patient feedback of provider counseling behavior with the largest patient population studied, 79 in the before-intervention group and 81 in the post-intervention group. Another strength of our study is that patients provided assessment of provider performance through surveys filled out immediately after the initial prenatal visit, thus eliminating recall bias inherent in phone interviews used in previous studies. This may partially explain the high rate of general breastfeeding discussion reported in our study (62% before intervention and 79% after intervention) compared with previous studies. Another reason may be that residents were more conscientious in performing breastfeeding counseling even before the educational intervention due to their knowledge of an ongoing study on breastfeeding. Discussion of specific benefits of breastfeeding remained sparse at 15–30% for each topic both before and after the intervention. This is to be expected given the time constraint at the initial prenatal visit, and it may in fact not change with improved resident knowledge of breastfeeding benefits.
Although many of the same residents were surveyed before and after the educational intervention, the survey responses were collected anonymously. Therefore, the paired nature of these surveys could not be taken account of in analysis. We would expect this to overestimate variation, given a positive correlation between surveys resulting in conservative confidence intervals and larger p-values than would be obtained otherwise. Furthermore, it is unknown which residents saw which patients, therefore, a potential individual resident effect could not be accounted for in the analysis of patient responses. Future studies with larger patient population will be needed to calculate a paired t-test, and control for other variables such as a resident's own experience with breastfeeding, year in training, age, and gender. Another limitation of this study is the short duration and number of lectures given as the educational intervention on breastfeeding. However, it is encouraging to find an improvement in resident counseling behavior with such limited intervention. It highlights the potential effectiveness of such educational interventions.
Conclusion
Our study showed that a brief educational intervention on breastfeeding had a meaningful impact on OB/GYN resident physician counseling behavior. We feel it is imperative that all OB/GYN residency training programs include breastfeeding training in their curricula and potentially include breastfeeding counseling as a target to be met in resident prenatal clinics.
Footnotes
Acknowledgments
The authors would like to thank Kathy Martin, RN, and Cindy Overholts, clinical research coordinator, for collecting the patient surveys in this study. Kathy Martin and Cindy Overholts are both employed by the Ohio State University Wexner Medical Center. They did not receive compensation outside of their salary for their work in this study.
Disclosure Statement
No competing financial interests exist.