
Abstract
Abstract
Objective:
The objective of this study was to assess whether a diet of ≥50% breast milk (BM) was associated with earlier transition off parenteral nutrition (PN) in neonates with gastrointestinal (GI) disorders.
Methods:
This retrospective study assessed enteral feeding outcomes of neonates with surgical GI disorders admitted within the first week of life to a single center between January 1, 2012 and August 10, 2015. Outcomes were assessed according to diet from the point of first enteral intake through 7 days of full enteral feeds. Diets were classified as 100%, ≥50%, or <50% BM.
Results:
One hundred sixty-three patients with an average gestational age of 36 weeks (range 28–40) and birthweight of 2570 g (range 1250–4900) were included. Significant differences in days to full enteral feeds between the 100% and <50% BM groups were found (median 21 versus 32 days; p = 0.023). There were no significant differences between the 100% and ≥50% BM (p = 0.05) or ≥50% versus <50% BM groups (p = 0.74). The 100% BM group had significantly fewer days on PN compared to the ≥50% BM group (median 21 versus 28.5 days, p = 0.034). Hospital length of stay was significantly shorter in the 100% BM group, which was discharged an average of 10 and 13.5 days sooner than the ≥50% and <50% BM groups (p < 0.05).
Conclusions:
Neonates with specific GI disorders who received a 100% BM diet were found to achieve earlier full enteral feeds, have shorter PN courses, and be discharged from the hospital significantly sooner than those who received diets that included formula.
Introduction
N
Data have demonstrated that breast milk (BM) diets for neonates with intestinal failure on PN are associated with a decreased duration of time on PN. 1 BM has been found to stimulate the development of healthy intestinal flora, modulate inflammatory processes, and encourage bowel maturity, repair, and function.1,5,6 In particular, BM diets in premature infants decrease the incidence of late-onset sepsis and necrotizing enterocolitis, increase intestinal motility and gastric emptying, and have general anti-inflammatory effects.5,7 Studies have also supported the role of BM diets in decreasing PN courses by more than 50% in infants with short bowel syndrome. 1 Furthermore, BM diets are associated with decreased time to full enteral feeds and decreased hospital length of stay (LOS) in select populations.5,7–11
We believe that decreasing the time that neonates with GI disorders spend on PN will improve clinical outcomes and decrease overall costs. While there is literature to support this conclusion in preterm and very low-birthweight neonates, there is a paucity of literature assessing the role of BM diets on outcomes of neonates who do not meet such criteria.5,7–8,10–14 The objective of this study was to assess whether a diet of ≥50% BM is associated with an earlier transition off of PN in neonates with specific GI disorders when compared to similar neonates who receive enteral diets <50% BM. Secondary outcomes included hospital LOS and days to achievement of full enteral feeds.
Materials and Methods
This retrospective cohort study received approval from the Institutional Review Boards of the Emory University School of Medicine and Children's Healthcare of Atlanta. After receipt of approval, the Children's Hospital's Neonatal Database (CHND) was queried for all neonates admitted to Children's Hospital of Atlanta at Eggleston's neonatal intensive care unit between January 1, 2012 and August 10, 2015. The study period was selected to include all eligible patients since 2012 to ensure a more standardized approach to lipid management.
Neonates admitted in the first 7 days of life, with a birthweight of 1250 g or greater, and a diagnosis of gastroschisis, omphalocele, small bowel atresia, volvulus requiring bowel resection, surgical necrotizing enterocolitis, spontaneous intestinal perforation, or complicated meconium ileus requiring bowel resection were included. Demographic and clinical information were abstracted from CHND. Further retrospective chart review was performed to confirm the abstracted data and attain additional information.
All information was taken directly from the electronic medical record. Included variables are listed in Appendix A. Full enteral feeds were defined as 100 kcal/kg/day. Diet categorizations were 100%, ≥50% (but <100%), and <50% BM. These categorizations were determined as the cumulative percentage of feeds from the point of first enteral intake through 7 days of full enteral feeds. These categorizations were decided upon to better assess whether any potential benefits of a BM-predominant diet required exclusive intake of BM. For the purposes of this study, BM was defined as mother's own milk or pasteurized donor milk.
Statistical analyses were performed using SAS 9.4 and statistical significance was assessed at the 0.05 level, unless otherwise noted. Descriptive statistics were reported for all variables of interest. Continuous measurements were reported as means and standard deviations or as medians and interquartile ranges according to the distribution of the data. Counts and percentages were reported for categorical data.
Comparisons between three or more groups were made using one-way analysis of variance or Kruskal–Walis tests for continuous measurements or Chi-square tests for categorical comparisons. Post-hoc multiple comparisons for continuous variables were made using Dwass-Steel-Critchlow-Fligner (DSCF) test, which was based on pairwise two-sample Wilcoxon nonparametric comparisons. Count data (number of days) were analyzed through using the Zero-Inflated Negative Binomial Regression modeling to account for excessive zeroes and overdispersion. Normality of continuous variables was assessed using histograms, normal probability plots, and through the Shapiro–Wilk tests for normality. When data were non-normally distributed, appropriate nonparametric tests (previously described) were utilized. In instances of small expected cell counts during analysis of categorical data, Fisher's exact tests were used in place of traditional Chi-square tests. Any neonates with missing data were excluded from analysis. Loss to follow up was not addressed as the primary and secondary outcomes were measured before hospital discharge.
Results
Figure 1 is a flow diagram that depicts patient inclusion from the point of CHND identification. Baseline characteristics of the study population are shown in Table 1. Overall, the majority of neonates included in this study were born between 35 and 38 weeks gestation, with an average gestational age of 36 weeks. No neonates weighed less than 1250 g, with the average birthweight being greater than 2500 g. The most common comorbidities were gastroesophageal reflux, patent ductus arteriosus, failure to thrive, intrauterine growth restriction, hydronephrosis, respiratory failure, persistent pulmonary hypertension, and bronchopulmonary dysplasia. Figure 2 depicts the distribution of patients with each of the selected GI diagnoses.
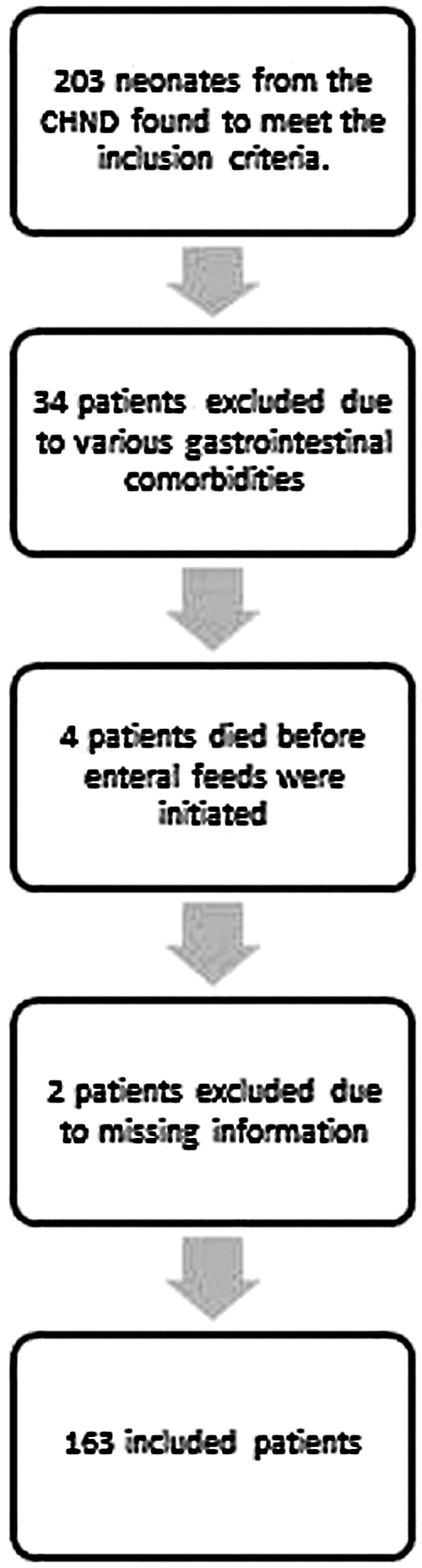
Patient inclusion diagram. CHND, Children's Hospital's Neonatal Database.
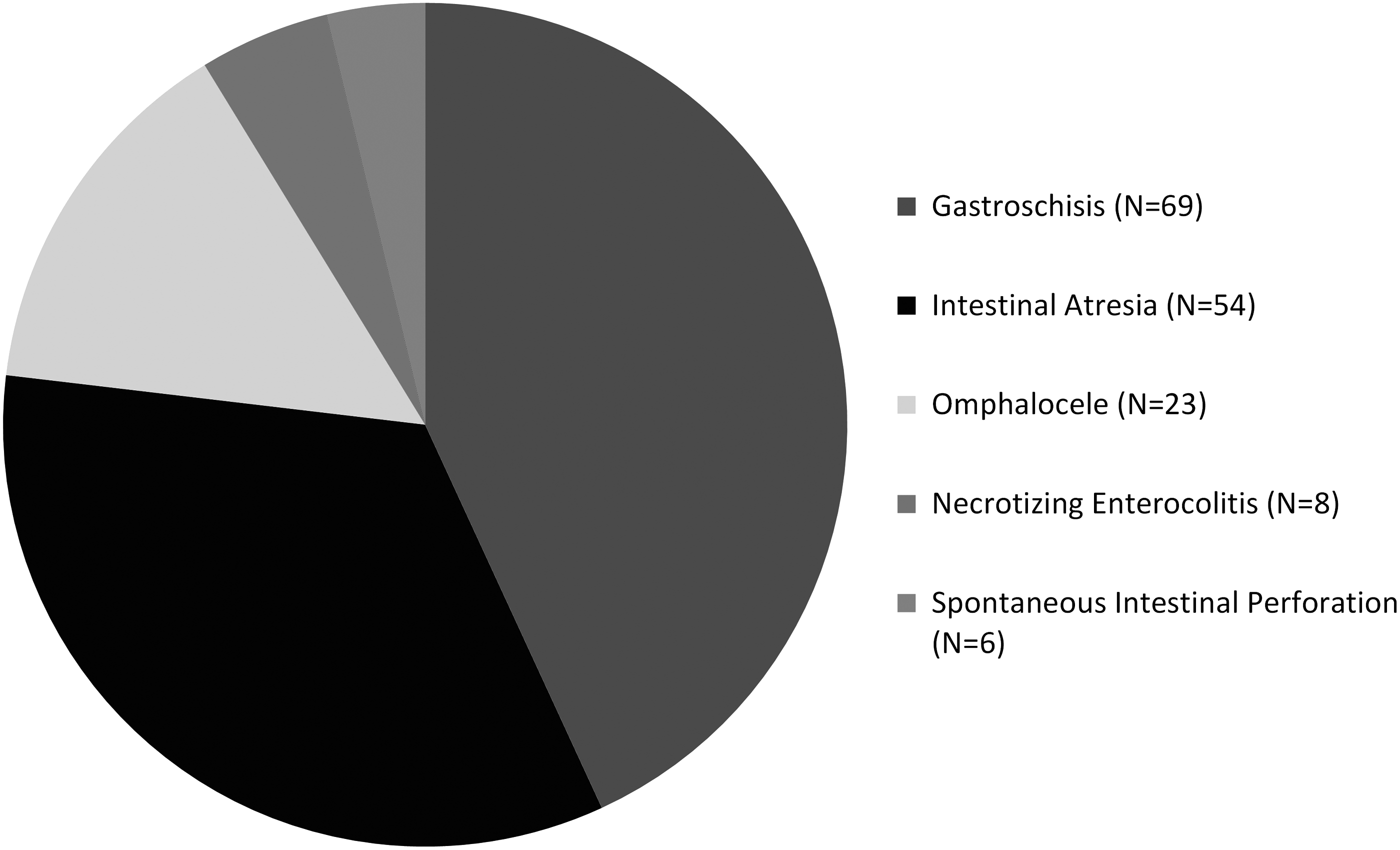
Proportion of patients with each included diagnosis.
Baseline characteristics of included patients. No associations were found between diet exposure and gender, gestational age, birthweight, age at admission, race, primary diagnosis, number of comorbid conditions, presence of a stoma, or days to bowel continuity. Results are reported as the raw number of patients with the percentage of the total in parenthesis, unless otherwise noted.
BM, breast milk; LBW, low birthweight (1500–2499 g); VLBW, very low birthweight (1250–1499 g).
The <50% BM group ultimately included 18 neonates that received only commercial formula and 34 neonates that received a diet with some, but <50%, BM. There was no difference in time to initial enteral feeds between groups (Table 2). There were significant differences in days to full enteral feeds between the 100% and <50% BM group (median 21 days, 25th–75th percentiles 15–30, versus 32 days, 25th–75th percentiles 21–61.5; p = 0.023). However, the differences in times to full enteral feeds between ≥50% BM group when compared to the 100% and <50% BM groups were not found to be statistically significant (Table 2).
Selected outcomes according to diet exposure. Due to the non-normality of data, distribution medians are reported. Time to initial enteral feeds was not found to be significantly different between groups. Pairwise comparisons found significant differences in time to full enteral feeds between the 100% and <50% BM groups. All other pairwise comparisons had a calculated p > 0.05. Significant differences in the total days on PN were found between the 100% and >50% BM groups. Significant differences were also found with regard to hospital stay in the 100% versus >50% BM and 100% and <50% BM groups. Culture-proven sepsis episodes, biopsy-supported diagnoses of TPN cholestasis, and survival were not found to be significantly different between diet groups.
Significantly different.
[], interquartile range; LOS, length of stay.
Table 2 shows patient outcomes by diet exposure. The 100% BM group had significantly fewer days on PN when compared to the ≥50% BM group (median 21 days versus 28.5 days, p = 0.034). The difference in the duration of PN in the ≥50% BM compared to the <50% BM group was found to be neither clinically nor statistically significant (median 21 days versus 20 days, p = 0.08). Hospital LOS was significantly decreased in the 100% BM group, with the 100% BM group discharged an average of 10 days sooner than the ≥50% BM group and 13.5 days sooner than the <50% BM group (p < 0.05). No significant differences in the occurrence of biopsy-supported diagnoses of PN-associated liver disease, episodes of culture-proven sepsis, or survival were found.
There were no significant differences in patients discharged on PN between groups (Table 2). In the 100% BM group, 1.85% were discharged on PN, in the ≥50% BM group, 7.69% were discharged on PN, and in the <50% BM group, 9.09% were discharged on PN (p = 0.27). There were higher peak direct bilirubin levels and more patients with a direct bilirubin ≥2 mg/dL in groups with more formula exposure (p < 0.05, Table 3). The <50% BM group was significantly less likely to have zero days with a direct bilirubin ≥2 mg/dL than the 100% and >50% BM groups (p < 0.05). The number of days with direct bilirubin ≥2 mg/dL for the <50% BM group was 2.18 times higher than the 100% BM group (p = 0.07).
The peak direct bilirubin levels in milligrams per deciliter (mg/dL) and the number of patients with any direct bilirubin ≥2 mg/dL. Results are reported as the number of patients with the percentage of the total in parenthesis, unless otherwise noted. Significant differences between the 100% BM and <50% diet groups were found with regard to peak direct bilirubin levels. Of the patients with a direct bilirubin ≥2 mg/dL, the median number of days ≥2 and 4 mg/dL are shown. These counts are not mutually exclusive. Analysis of maximum likelihood zero inflation parameter estimates found that neonates exposed to a <50% BM diet were significantly more likely to have direct bilirubins ≥2 and >4 mg/dL, on at least 1 day, when compared to the 100% and >50% BM groups.
Significant difference found between 100% and <50% BM.
Significant differences found between the <50% BM group and the other groups.
CF, commercial formula; Dbili, direct bilirubin.
Discussion
The objective of this study was to assess whether a diet of ≥50% BM is associated with an earlier transition off of PN in neonates with surgical GI disorders when compared to similar neonates who received enteral diets of <50% BM. There was a trend toward earlier transition off of PN with an increased percent of the diet comprising BM, with 100% BM having a median of 21 days on PN, which was 7.5 days shorter than the ≥50% cohort and 9 days shorter than the <50% BM cohort. The difference between the 100% BM group and ≥50% BM was found to be statistically significant (p = 0.034), although the difference between the 100% BM and <50% BM groups was not (p = 0.08). In addition, there was no significant difference in time on PN between the ≥50% and <50% BM groups (p = 0.96). The sample size of the <50% BM group may have been too small to detect statistically significant differences between that group and the others. There were no significant differences in the baseline characteristics between groups, which suggest that the cohorts were appropriate for comparison. There were similar frequencies between diet groupings, with 54 patients analyzed as 100% BM (33.13% of the population), 65 as ≥50% BM (39.88%), and 44 as <50% BM (26.99%). It is interesting to observe that the trend toward earlier transition off of PN was greatest in the 100% BM group, which transitioned off at least a week earlier than the other two groups. Conversely, the ≥50% BM group transitioned off of PN at a median of only 1.5 days earlier than the <50% BM group.
Secondary outcomes of this study included decreased hospital LOS and earlier achievement of full enteral feeds. The 100% BM cohort was found to have significantly shorter hospital LOS compared to the ≥50% and <50% BM groups (median 27.5 days versus 40 and 51 days, respectively, p < 0.05). The difference between the ≥50% and <50% BM groups was not found to be significant (11 days, p = 0.97). Again these results likely reflect numerous factors, including the relatively small sample size in the <50% BM group and the fact that neonates with longer hospital stays have an increased likelihood of being given formula.
The 100% BM group did achieve full enteral feeds significantly earlier than the <50% BM group (median 21 days versus 32 days, p = 0.023). There is literature to support a dose–response effect of BM in select populations.8,15 However, unlike days on PN and hospital LOS, the 100% BM group was not significantly different from the ≥50% BM group with respect to days to full enteral feeds, despite a trend toward significance (median 21 days versus 29.5 days, p = 0.05). This finding reflects that full enteral feeds are achieved earlier with 100% BM diets, and it is likely that a more strongly powered study would be able to detect a difference between 100% and ≥50% BM with respect to enteral feeding outcomes.
With the known risks that prolonged PN poses to the liver, it is important to consider whether BM improves hepatic outcomes, including direct bilirubin levels, PN-associated liver disease, and liver failure. Of particular interest to those caring for neonates with short bowel syndrome is the finding that BM has been found to be protective from developing PN-associated liver disease when on PN greater than 4 weeks. 16 Our findings revealed an association between increased formula intake and: 1) higher peak direct bilirubin levels; 2) increased number of patients with any direct bilirubin greater than 2 mg/dL; 3) and, of those patients with direct bilirubin greater than 2 mg/dL, an increased number of days with a direct bilirubin greater than 2 mg/dL (Table 3). In addition, the <50% BM group was significantly less likely to have zero days with a direct bilirubin greater than 2 mg/dL than the 100% and >50% BM groups (p < 0.05). Overall, there were 51 cases of biopsy-supported diagnoses of PN-associated liver disease, which were relatively evenly spread across dietary exposure groups (p > 0.05). However, there is selection bias for those who need additional surgeries being more likely to undergo liver biopsy.
The number of culture-proven sepsis episodes in each group was also investigated as a secondary outcome to investigate the known association between PN and infectious complications. Infants on PN are uniquely predisposed to such infectious complications due to the persistent need for an indwelling central venous catheter through which protein and sugar substrates are infused. In addition, neonates with GI disorders may have inflamed intestinal mucosa with altered permeability and a relatively immunocompromised state.
Septic complications are prevalent among neonates with short bowel syndrome on PN, with studies showing rates as high as 68–80%.1,17,18 Patel et. al found that for each increase of 10 mL/kg/day of BM that an infant consumed, the odds of subsequently developing sepsis were reduced by 19%. 8 Our data revealed a greater percentage of culture-proven sepsis episodes in patients receiving <50% BM, although this difference did not reach significance (P = 0.12).
This study is novel in that its population comprised neonates with surgical GI disorders who are not early preterm or of very low birthweight. This population is largely excluded from earlier BM studies, which tend to focus on very low birthweight and premature neonates. However, neonates with surgical GI disorders may be of those most likely to benefit from BM diets, as they are likely to have intestinal dysfunction. These benefits are thought to be conferred through components of colostrum and BM, including IGF-1, GLPf-2, EGF, GH, immunoglobulin A, erythropoietin, G-CSF, and leukocytes, which are believed to promote adaptation of remnant bowel and neonatal immune function.19–27
The neonates considered in this study had an average gestational age of 36 weeks and an average birthweight of 2570 g. There is a paucity of literature regarding the effect of BM diets on outcomes in neonates with a birthweight greater than 1500 g, and it is unknown if many of the widely reported benefits of BM are applicable to larger neonates. However, the benefits of BM in neonates that are larger, or born at more advanced gestational ages, may be more subtle than those found in smaller and more premature infants. Thus, it is reasonable to expect that larger sample sizes would be needed to detect smaller differences, and our study reveals only the greatest benefits.
Despite the small sample size, it is interesting to see the relatively large differences in enteral feeding outcomes, PN courses, and hospital LOS that were found. Our data suggest that in our population of infants with GI disorders, the benefits of BM can be striking. While 100% BM diets were associated with the most significant results, the data support the hypothesis that there are likely differences conferred through a diet that is even a majority BM.
There are numerous limitations to this study. One potential limitation is that a prolonged PN course will bias the results to reflect an association with formula. Neonates with prolonged courses of PN are more likely to have received formula, as they will have had prolonged hospital stays, with more recorded feedings, and more opportunities to be given formula due to unavailability of BM. Next, it is important to acknowledge that this study was not designed to detect small differences in rare outcomes and is limited by its sample size. In addition, this study does not stratify BM outcomes according to pasteurized donor BM versus mother's own BM. Very few of the neonates included in this study received donor BM and those who did, often received it within the context of a predominantly mother's own BM diet. Last, our study population was heterogeneous in terms of qualifying diagnoses, gestational age, and birthweight. Most of the published literature regarding BM specifically addresses outcomes in the lowest birthweight and most premature neonates. There are little data on the effects of a BM diet in the more heterogeneous neonatal surgical population, and our population was designed to be heterogeneous to begin to fill this gap in knowledge.
In consideration of the objectives, limitations, and biases of this study, the authors recommend a cautious overall interpretation of the results. It is likely that BM confers significant advantages to neonates with surgical GI disorders regarding PN outcomes, enteral feeding outcomes, and hospital LOS. These results are more generalizable to neonates with surgical GI disorders than the previously published studies of predominantly low birthweight and early preterm neonates. More high-quality studies are needed to assess the role that BM can play in enteral feeding and infectious and hepatic outcomes in neonates with surgical GI disorders.
Conclusion
In conclusion, BM conferred significant advantages to neonates with surgical GI disorders who were predominantly late preterm to term and nonlow birthweight. Neonates with surgical GI disorders who received a 100% BM diet were found to achieve earlier full enteral feeds, have shorter PN courses, and be discharged from the hospital significantly sooner than those who received diets that included formula. The data suggest a potential for benefit conferred through a diet of ≥50% BM. More studies are needed to determine if there is a dose–response effect of BM on infectious, hepatic, and enteral feeding outcomes in neonates with surgical GI disorders.
Footnotes
Disclosure Statement
No competing financial interests exist. The authors have no affiliations, including consultantships, honoraria, stock ownership, equity interests, arrangements regarding patents, or other vested interests to disclose.
Appendix A
Abstracted variables included name, medical record number, date of birth, date of admission, neonatal intensive care unit (NICU) discharge date, hospital discharge date, birthweight, survival, care completed at the study institution, gender, gestational age, race, ethnicity, administration of antenatal steroids, inclusion diagnosis, comorbid diagnoses, presence of an ileocecal valve, presence of a microcolon, estimated residual small and large bowel length, presence of an ascending, transverse, or descending colon, presence of a stoma, location of a stoma (if applicable), days to bowel continuity (if applicable), episodes of medical necrotizing enterocolitis, date of any gastrointestinal surgery or surgeries, day of parenteral nutrition (PN) initiation, day of PN cessation, date of initial enteral feeds, date of full enteral feeds, type of enteral feeds, diet upon discharge, line complications, sepsis episodes, sepsis organisms, maximum direct bilirubin levels, days with a direct bilirubin ≥2 mg/dL, days with a direct bilirubin ≥4 mg/dL, liver biopsy results (if applicable), presence of liver failure, CMV status (if known), date of any hospital readmission, and occurrence of liver or small bowel transplant.
Calculated variables included day of life, hospital length of stay, NICU length of stay, floor length of stay, percent of predicted small bowel length, presence of short gut syndrome, days on PN, and days to hospital readmission.