
Abstract
Abstract
Objective:
To identify independent maternal and infant factors associated with donor milk nonconsent and to examine secular trends in nonconsent rates.
Materials and Methods:
Mothers of infants eligible to receive donor milk (≤32 weeks of gestation or ≤1,800 g) born between August 2010 and 2015 were included. Multivariable logistic regression modeled odds of nonconsent.
Results:
Of the 486 mother/infant dyads from the first 5 years of the donor milk program, nonwhite race (adjusted odds ratio [aOR] 1.69; 95% confidence interval [CI] 1.04–2.76) and increasing gestational age (aOR 1.11; 95% CI 1.03–1.21) independently predicted nonconsent. Each year the program existed, there was a 48% reduction in odds of nonconsent (aOR 0.52; 95% CI 0.43–0.62). The most common reason given for nonconsent was “it's someone else's milk.”
Conclusion:
Program duration was associated with reduced nonconsent rates and may reflect increased exposure to information and acceptance of donor milk use among neonatal intensive care unit staff and parents. Despite overall improvements in consent rates, race-specific disparities in rates of nonconsent for donor milk persisted after 5 years of this donor milk program. Further research is warranted to clarify the basis for race-based disparities in donor milk nonconsent rates, with the goal of designing interventions to reduce donor milk refusal among minority mothers.
Introduction
V
While evidence clearly demonstrates the benefits of donor milk for VLBW infants, the acceptability of donor milk among parents is less well defined. Consent rates appear dependent upon maternal education, marital status, and cultural context, while the effect of race or ethnicity on donor milk consent is not clear.12,15–19 A prior study assessing nonconsent rates of a local NICU program, consistent with prior research, found maternal race and marital status to be significant predictors of donor milk nonconsent. 18 However, with the implementation of intervening programmatic changes, greater recognition of donor milk as an available option and increased numbers of parents’ approach to consent for donor milk over the past 5 years have highlighted the need to reevaluate consent patterns for donor milk and determine whether rates of nonconsent have improved since the earlier evaluation of the program. Using data from this 5-year cohort, our group has updated our preliminary results, 18 further assessed current predictors of donor milk nonconsent status in a NICU setting, and examined trends in nonconsent rates over time.
Materials and Methods
The donor milk program at this level IV urban NICU was established in August 2010 to provide access to human milk when mother's own milk is unavailable.18,20 Infants born at ≤32 weeks of gestation or ≤1,800 g are eligible to receive donor milk. If consent is obtained, donor milk is provided until the infant reaches 34 weeks postmenstrual age, until 50% oral feedings are achieved, or until the infant is discharged. For eligible infants, consent from either parent is sought once by a credentialed clinician before the determination of need for donor milk. At this time, the benefits of a human milk diet are explained to the parent. A family's ability to pay does not influence access to donor milk. Parents declining donor milk, and for whom mother's own milk is also unavailable, are fed preterm formula. In the event of nonconsent, parents are asked to provide their primary reason for declining donor milk.
Maternal/infant dyads were eligible for inclusion in this study if the infant was inborn between August 1, 2010 and August 1, 2015 and qualified for donor milk in accordance with the institution's eligibility criteria for donor milk receipt policy. Data were abstracted from in-hospital medical records. Donor milk nonconsent was defined as parents who refused consent or infants with no documentation of donor milk consent in the medical record.
We compared maternal demographics and other factors by donor milk consent status using the Chi-square or Fisher's Exact test for categorical variables and Student t test or Mann–Whitney U test for continuous variables. Multivariable logistic regression modeled odds of nonconsent adjusted for independent risk factors identified in bivariate analysis (p < 0.1) using the backward selection and a retention threshold of p < 0.1. The Hosmer and Lemeshow goodness-of-fit test and receiver operating characteristic (ROC) curves assessed how well the final model fit these data. Self-report reasons for donor milk nonconsent and clinical personnel obtaining consent were also described. A Poisson regression model estimated the occurrence of a not documented nonconsent over the duration of the donor milk program.
This retrospective research was exploratory, and therefore, no sample size calculation was performed. Analyses were conducted in SAS version 9.3 (SAS Institute, Inc., Cary, NC). All p-values were two sided, and significance was set at α < 0.05. The Connecticut Children's Medical Center Institutional Review Board approved this study.
Results
A total of 510 observations, representing a chart for an individual infant, were available for review. After excluding infants either immediately deceased or transferred (n = 7) and those receiving exclusive formula or >50% oral feedings and thus ineligible for donor milk (n = 17), 486 observations were included in the analyses. Of the 486 mother/infant dyads from the first 5 years of the donor milk program, 380 parents consented and 106 did not consent to donor milk use; this includes refusal or undocumented consent.
Study characteristics were stratified by donor milk consent status (Table 1). Of infants that qualified for donor milk, those for whom parents provided consent differed from those not consenting with respect to maternal race; families with white mothers more likely to provide consent (61.9% relative to 50.5%; p < 0.04). No differences in distribution of consent status were observed regarding ethnicity, multiple births, parity, insurance, maternal marital status, maternal partner support, maternal education, maternal history of obesity, maternal history of infertility, maternal history of polycystic ovarian syndrome, maternal history of breastfeeding, maternal breastfeeding duration goal, delivery mode, infant diagnosis of NEC or sepsis, or infant death before discharge.
Observations <486.
p-Value generated from a Fisher's exact test instead of a chi-squared test.
PCOS, polycystic ovary syndrome.
Using multivariable logistic regression, nonwhite race (adjusted odds ratio [aOR] 1.69; 95% CI 1.04–2.76) and increased GA (aOR 1.11; 95% CI 1.03–1.21) were independent risk factors for nonconsent. Each year the program continued, there was a 48% reduction in odds of nonconsent (aOR 0.52; 95% CI 0.43–0.62; Table 2). The area under the ROC curve was 0.76, which suggests that the model has modest discriminating power. The Hosmer and Lemeshow goodness-of-fit test was not statistically significant, which indicates that these data fit the model adequately. Predicted probabilities of white/nonwhite race and GA over time are presented in Figure 1. Families with nonwhite mothers approached in the first year of the program whose infants were <37 weeks gestational age had the highest probability of nonconsent. Although the magnitude of racial disparities decreased over time, they were observed throughout the program duration.
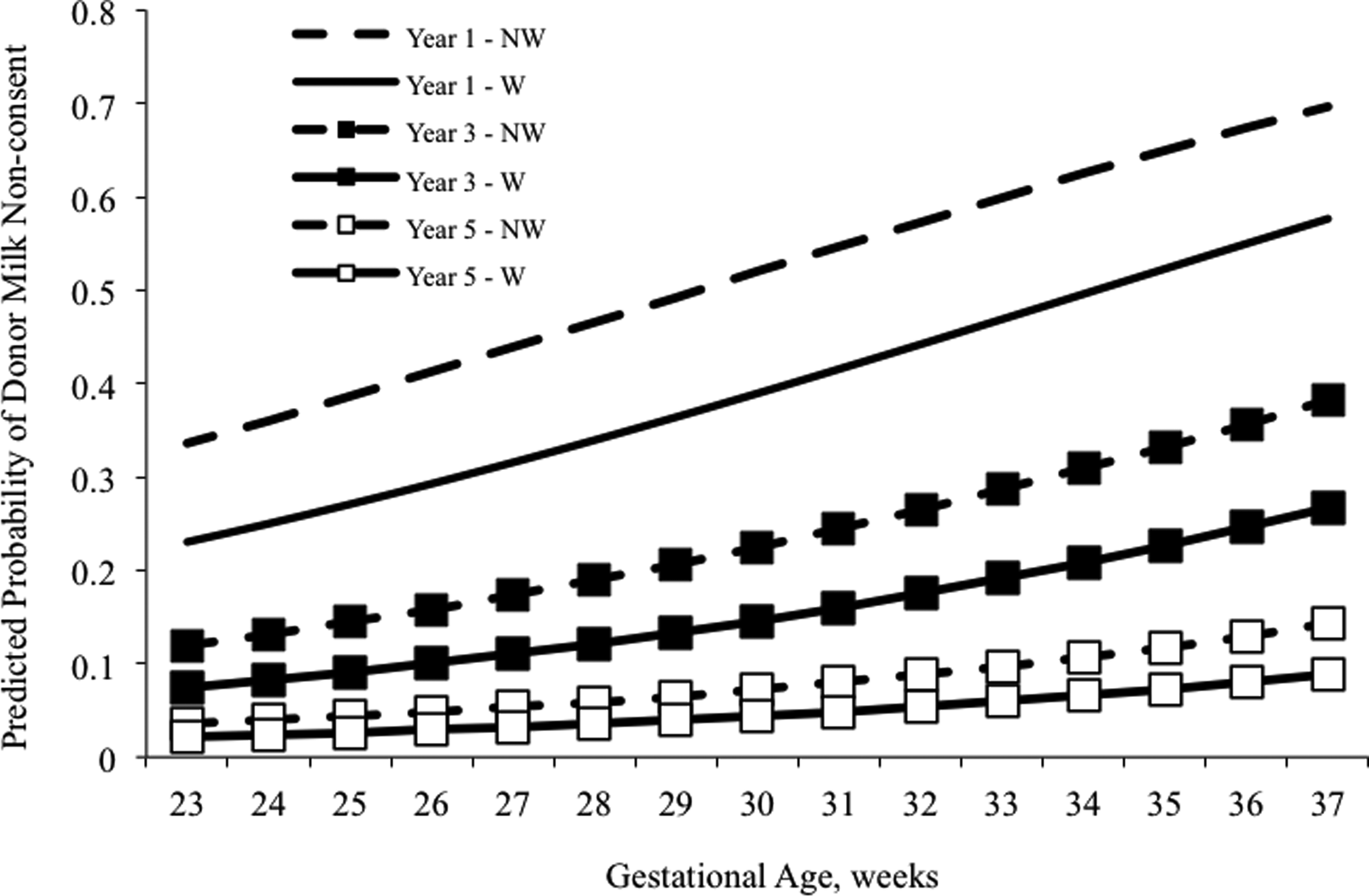
Predicted Probability of Donor Milk Nonconsent by Gestational Age, Year of Program, and Race. NW, Non-White; W, White. Eligibility for donor milk includes infants born ≤ 32 weeks gestational age or ≤ 1800 grams.
Represents the Type 3 analysis of effects Wald chi-square p-value.
aOR, adjusted odds ratio; CI, confidence interval.
The most common reason given for donor milk nonconsent was “it's someone else's milk” (Table 3). This categorization includes a combination of paternal refusal, those with donor milk safety concerns, and those not wanting someone else's milk. Of the 106 parents who did not provide consent for donor milk, 56 (52.8%) had no formal documented reason for nonconsent. Using Poisson regression, the number of not documented nonconsent observations decreased with each program year p < 0.0001. While international board certified lactation consultants (IBCLCs) obtained the majority of donor milk consents (49%; data not shown), attempts to obtain consent were distributed among clinical personnel.
Did not want other mom's milk (n = 38); safety concerns (n = 3); paternal refusal (n = 2).
Discussion
Despite overall improvements in consent rates, race-specific disparities in rates of nonconsent persisted after 5 years of a donor milk program. The primary reason for donor milk nonconsent was “it's someone else's milk.”
Two prior studies evaluating maternal and infant factors associated with NICU-specific donor milk nonconsent reported conflicting results.18,19 In the first 18 months of the program, our group observed a 42.4% donor milk nonconsent rate, 18 while Parker et al. reported a 9.6% donor milk nonconsent rate. 19 However, their 9.6% nonconsent rate underestimated their total nonconsent rate by excluding the 23.2% of those with undocumented consent status, representing those not exposed to the availability of donor milk use. The combined rate of 32.8% is similar to our initial reported nonconsent rate of 42.4%. Furthermore, the findings of our present study suggest that donor milk nonconsent rates significantly decreased with each year of the program, with the most recent year representing an 8% donor milk nonconsent rate and average rate of 10.3% over the last 3 years of the program. These data suggest that program duration may be associated with increased exposure to information and acceptance of donor milk use, which are reflected in reduced nonconsent rates.
To our knowledge, the type of practitioner obtaining consent has been previously reported in one national study and in our initial study.14,18 In a national survey of NICU medical directors of level III and level IV units (n = 153), 91 (59.4%) reported donor milk use. 14 Of those NICUs, the neonatologist, neonatal nurse practitioner, or physician assistant was most likely to obtain donor milk consent. 14 In our initial study, neonatologists and advanced practice registered nurses were most likely to obtain donor milk consent. 18 The findings from our present study indicate that IBCLCs commonly discuss consent for donor human milk with mothers of preterm infants, along with topics such as milk expression and breastfeeding goals.
The primary reported reasons for donor milk nonconsent are similar between our initial and presently observed results, with the most common reason given for nonconsent being “not wanting someone else's milk.” 18 Similarly, Esquerra-Zwiers and colleagues conducted a qualitative study among mothers who consented for donor milk to explore mother's perspectives on providing donor milk. 21 Consistent with our results, the primary hesitation to donor milk consent was not quality, but concerns over using “somebody else's milk.” 21
This study has several important strengths, primarily related to clinical donor milk program duration, available data, and study design. This comprehensive analysis is the first to model secular trends of donor milk nonconsent rates. Our multivariable model building process used an inclusive p-value retention threshold to maximize the number of potential independent predictors of donor milk nonconsent eligible for inclusion in the final model. Furthermore, we evaluated the statistical adequacy of the multivariable model fit to demonstrate the stability of our findings. This transparent model building process may inform research studies at other sites to confirm the generalizability of these results.
Despite the efforts outlined above, this study has several limitations. First, this is a single center study, which may limit generalizability. However, these results may inform research and quality improvement initiatives at other level IV urban NICUs with long-term donor milk programs. Second, we have high rates of undocumented reasons for nonconsent, but documentation significantly improved as the program continued and formal method data collection of documented reason of nonconsent was developed. In addition, the distribution of maternal race, maternal ethnicity, maternal education, English speaking, or partner support did not differ between those with undocumented reasons for nonconsent and those with documented reasons for nonconsent. Third, we did not systematically document the provider type who approached parents for consent, and therefore, we cannot suggest whether one type of provider is more successful at obtaining donor milk consent relative to other provider types. Finally, while our model fit these data and we identified statistically significant independent predictors of donor milk nonconsent, the observed results could be attributable to unmeasured confounding, potentially with regard to religion or paternal/partner demographics.
Conclusion
Using 5 years of data to describe secular trends after implementing a donor milk program, maternal nonwhite race and increased gestational age are independent risk factors for donor milk nonconsent rates. Reduction in nonconsent rates over time may reflect increased exposure to information and acceptance of donor milk use among NICU staff and parents. Further research is warranted to clarify the basis for race-based disparities in donor milk nonconsent rates.
Footnotes
Acknowledgments
The authors thank Joseph Duckett for his assistance in developing our research database and Donna Bielecki, RN, IBCLC, and Tracy Proulx, RN, IBCLC, for abstracting these data.
Disclosure Statement
No competing financial interests exist.