
Abstract
Abstract
Background:
The anogenital distance (AGD) is an anthropometric marker determined by exposures to androgens in utero and throughout the first few months of life. Early exposures to endocrine-disrupting chemicals such as phthalates have been significantly associated with shortened AGD in boys. Limited studies have explored phthalate concentrations in breast milk and infant formula.
Objective:
To explore the associations between breastfeeding duration and AGD measures in infants.
Materials and Methods:
MALAMA (Medio Ambiente y Lactancia Materna) is a follow-up study of 430 mother–child pairs, from birth to 2 years, from two population-based cohorts in Murcia, Spain. Data were collected through medical visits and telephone surveys from birth to 2 years of age. World Health Organization breastfeeding definitions were used. AGD measurements were assessed in a subsample of 71 boys and 49 girls at the 2-year visit. Descriptive analyses, Pearson correlations, and linear regressions were calculated between AGD and breastfeeding duration.
Results:
Duration of all types of breastfeeding, especially full breastfeeding (FB), is correlated with AGD measures in boys (p < 0.05). AGDAS (anoscrotal distance) and AGDAP (anopenile distance) were positively associated with FB (β = 0.004, 95%CI: 0.001–0.007 and β = 0.003, 95%CI: 0.000–0.007, respectively).
Conclusions:
A positive correlation between AGD in male infants and the duration of breastfeeding is reported. Inversely, early introduction of infant formula could lead to the reduction of AGD in boys.
Introduction
H
The anogenital distance (AGD) at birth is an anthropometric marker determined by exposures to androgens in utero. 7 From birth, the AGD grows rapidly and remains a sexually dimorphic marker. Growth of the perineum as determined by measurement of the AGD has been characterized by a rapid increase in the first 12 months of life, followed by gradual plateauing. 8 The AGD may be influenced by both prenatal and early postnatal androgen secretion, and has been identified as a predictor of male fertility, as men with poorer sperm quality display shorter AGDs.8,9
Exposure to some EDCs during early gestation has been shown to reduce the AGD at birth.10,11 The objective of this study is to explore the associations between breastfeeding duration and AGD measures in infants.
Materials and Methods
The MALAMA (Medio Ambiente y Lactancia Materna) project is a follow-up study of 430 mother–child pairs, from birth up to 2 years, from two population-based birth cohorts in the Region of Murcia.12,13 This study was based on the second de novo MALAMA cohort, with 327 of the total 430 pairs. 13 Newborns were recruited between June and July 2009. Inclusion criteria were the following: healthy full-term newborns (≥37 weeks of gestation), birth weight ≥2500 g, single pregnancies from natural conception, Apgar score of more than seven at 1 minute and eight at 5 minutes, and not hospitalized within the first 48 hours after birth. Data were collected through medical visits and surveys at birth and 2 years of age and telephone interviews at 3, 6, and 12 months of age. The study was approved by the institutional review board of the University Hospital Virgen of Arrixaca.
A subsample of randomly selected 120 infants at the 2-year follow-up visit was included in this study. A single physician with training and knowledge in environmental health and risk communication measured the AGDs, using a single set of vernier dial calipers with a scale of 0.1-mm increments. Following previous protocols,7–9 children were positioned on the examination table with their thighs at a 45°angle. The calipers were held in the right hand. In boys, the anoscrotal distance (AGDAS) was measured from the center of the anus to the posterior base of the scrotum. The anopenile distance (AGDAP) was measured from the center of the anus to the cephalad insertion at the base of the penis. The stretched penis length (SPL) was measured with a ruler from the pubic ramus to the glans, with the penis fully stretched. 14 In girls, the anoclitoral distance (AGDAC) was measured from the center of the anus to the anterior tip of the clitoral hood. The anofourchette distance (AGDAF) was measured from the center of the anus to the base of the posterior fourchette.7,8
The parents completed detailed questionnaires, which included items on sociodemographic characteristics, environmental exposures, and lifestyle variables. Taking into account previous evidence, this study examined possible confounders such as birth weight penis length and weight and height at age two, race and ethnicity, family income, parental education level, parental tobacco and illegal drug use during and after pregnancy, and ambient air quality as measured by an air pollution annoyance scale.15,16 This scale relates the perceived risk of families with outdoor air quality on an 11-point Likert scale and ranges from 0 (no disturbance at all) to 10 (intolerable disturbance). 16
Breastfeeding data were collected as recommended by the World Health Organization: full breastfeeding (FB) includes exclusive (no other liquid or solid was given to the infant) and almost exclusive (vitamins, mineral water, juice, or ritualistic feeds were infrequently given in addition to breastfeeds). 17 The FB and formula-feeding durations were recorded along with the date when formula feeding was first introduced into each infant's diet. The duration of FB or any breastfeeding (AB) was used as a continuous quantitative variable (days of lactation) in the analysis.
The data analysis and frequency contingency tables were computed with SPSS 15.0. Partial Pearson correlations and linear regressions were calculated for boys and girls between both AGD measures and duration of each type of breastfeeding, while controlling for birth weight and weight and height at 2 years of age. Student's t-tests were used to compare the means of continuous variables between boys and girls and chi-squared tests to assess the independent categorical variables. A linear regression analysis was performed in which the outcome variables were the AGD measures. To obtain other predictor variables, the comparisons of all variables were made using one-way ANOVA and Pearson correlations. Results of the analysis were reported at α level 0.05 with the corresponding confidence intervals (95% CI) for regression coefficients.
Results
A total of 120 children (71 boys and 49 girls) completed the required surveys and visits. The mean (95% CIs) AGDAS, AGDAP, AGDAF, and AGDAC measures were 4.4 (4.1–4.7) cm, 8.1 (7.8–8.4) cm, 2.4 (2.2–2.6) cm, and 6.0 (5.6–6.4) cm, respectively. Neither the sociodemographic characteristics nor the mean duration of FB was significantly different between boys and girls. The mean SPL was 3.4 (3.2–3.5).
None of the demographic characteristics were significantly associated with AGD or SLP measures. There was a significant association between AGDAC and anthropometric variables in girls (birth weight and both weight and height at 2 years of age) and AGDAP with weight at 2 years of age in boys. Significant positive correlations between the duration of breastfeeding and AGD were found only in boys (Table 1). In the multivariable regression analyses adjusting for birth weight and weight and height at age 2, the FB duration was a significant predictor of both AGD measures (Fig. 1) in boys. AB duration was a significant predictor of the AGDAP measure in boys (r 0.28, p < 0.05).
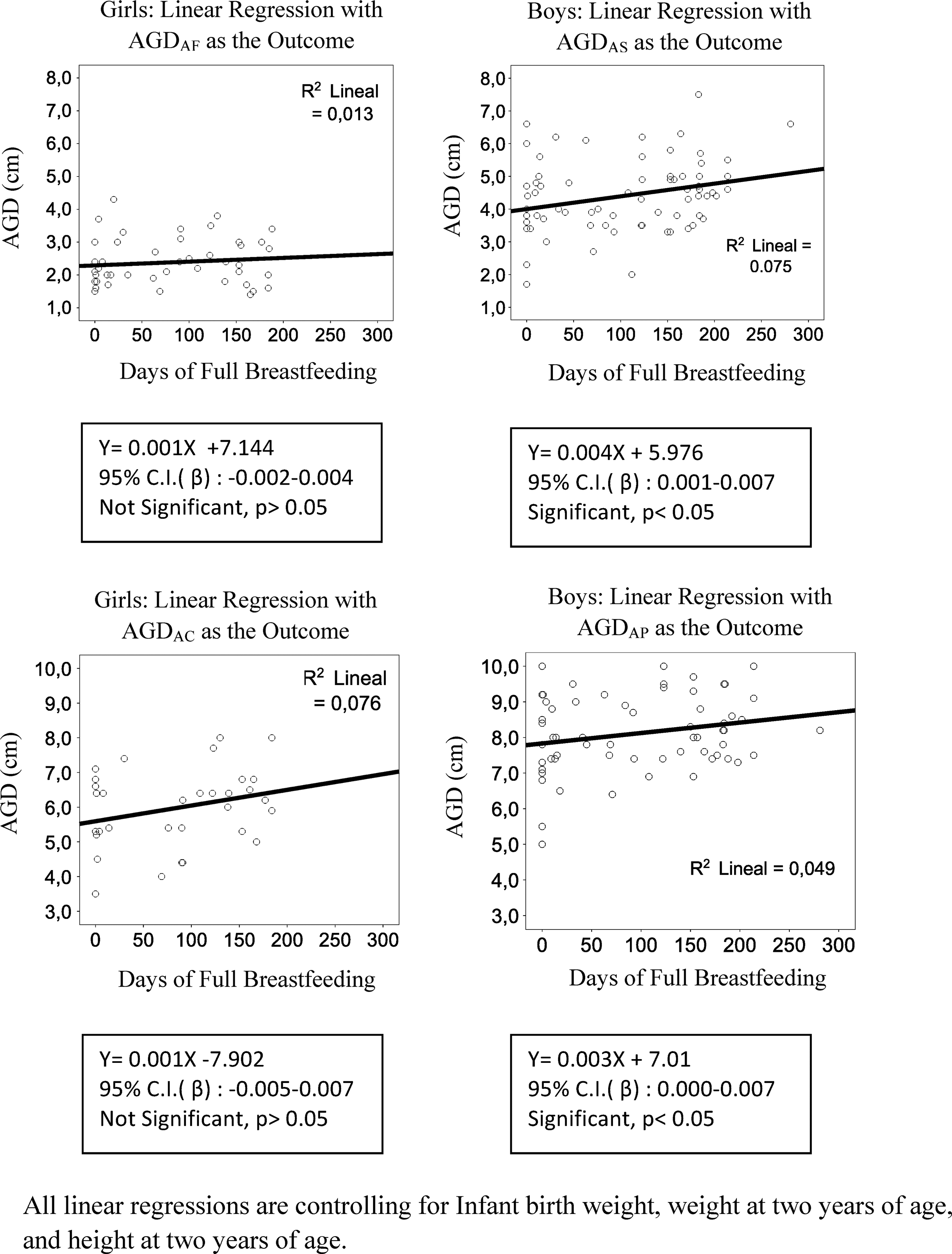
Association of full breastfeeding duration as a predictor of anogenital distances. AGD, anogenital distance.
Correlations of breastfeeding variables were adjusted for birth weight and weight and height at 2 years of age.
Average number of days after which formula feeding was introduced.
Significantly associated with AGD measures (p < 0.05), as determined by Pearson correlations.
Full breastfeeding includes exclusive and almost exclusive breastfeeding (vitamins, mineral water, juice, or ritualistic feeds were infrequently given in addition to breastfeeds).
AGD, anogenital distance; CI, confidence interval; NS, not significantly associated.
Discussion
The results suggest the existence of an association between breastfeeding duration and the AGD measures of 2-year-old boys. According to the linear regression, both AGD measures of boys would be increased by about 0.1 mm for each additional month of FB. The AGDs measured in girls and boys are similar to those obtained in previous studies of infants of similar ages.18,19 As in previous studies, a significant correlation between infant AGD and weight and height was found. 20
The strongest associations between male AGD measurements and breastfeeding types were seen for FB (Fig. 1). Nevertheless, the AGDAP measure was also significantly associated with the duration of AB. The differences between the two subcategories of FB (exclusive and near exclusive) are mainly conceptual since in both cases the burden of nutritional contributions falls on breast milk.
Experimental studies have demonstrated that AGD is determined in utero and persists during adulthood. 21 However, it has been recently reported that AGD in adult rats displays certain degree of plasticity, which may be mediated by modulation of local androgen/estrogen action. 22 This finding is yet to be determined in humans.
Previous studies show that the growth of the AGD occurs throughout the first year of life and is particularly fast during the infant's first 6 months. 8 This growth could be related to transient activation of the pituitary–gonadal axis during the first few months after birth that has been observed in other studies. 9 Levels of gonadotropins and sex hormones are elevated in humans in a period known as minipuberty. Male minipuberty regulates long-term testicular functions and sperm production and contributes to masculinization of the brain.23,24 The role of female minipuberty remains unknown. However, exposure to EDCs that interfere with the hormonal environment could alter the AGD growth.
There are some limitations to this study. The lack of AGD measurements at birth prevented the quantification of relative AGD changes during the infant's first 2 years. The infant's EDC exposure was not measured at any prenatal or postnatal time point. In addition, there are confounding factors that may both impact breastfeeding duration and AGD. Previous studies suggest that estrogenic EDCs interfere with lactation.25,26 The presence of these substances has been confirmed in both breast milk and infant formula.27–29 Limited existing evidence suggests EDC exposure to be equal or slightly higher through infant formula than breast milk. 30 Soy-based formula should also be taken into consideration in further studies due to its estrogenic activity. 31 To understand the impact of both EDC exposures and breastfeeding on ADG, future investigations should assess both prenatal and postnatal exposures, including a serial measurement of AGD and to measure EDCs in formula and breast milk. Another limitation was the relatively small size of the sample in this exploratory study. This was specially important for female patients, where only 49 patients were recruited and no significant correlation between AGD and breastfeeding was found. Sources of phthalate exposure are not only limited to the infant's diet but are also present in consumer products and house dust.32–34
The results of this study suggest breastfeeding to be a protective factor against the reduction of the AGD of 2-year-old boys in Murcia. This could be related to an early exposure to EDCs through baby formula. AGD is considered a useful parameter of adult reproductive health.9,35 Consequently, any type of breastfeeding could be potentiating the fertility of future adult males. Taking the significance of its association with both AGD measures into account, FB could be an effective way of preventing AGD shortening and promoting male fertility in future generations.
Conclusion
After adjusting for birth weight, and weight and height at 2 years of age, significant positive correlations between the duration of breastfeeding and AGD were found in boys. No significant differences were found in girls. The data suggest that early introduction of infant formula may reduce the AGD in boys.
Funding
This work was supported by Mount Sinai International Exchange Program for Minority Students (grant MD001452) from the National Center on Minority Health and Health Disparities of the U.S. National Institutes of Health; and the Crecer sin OH Program Regional Coordination of DG Public Health and Drug Addiction, The Regional Ministry of Health, Murcia, Spanish National Plan on Drugs, Ministry of Health, Social Services and Equality, Madrid, Spain.
Footnotes
Disclosure Statement
No competing financial interests exist.