
Abstract
Abstract
Background:
It is well recognized that breastmilk provides optimal nutrition and immunological protection for infants. Many women, however, experience nipple pain while breastfeeding, leading to premature cessation of nursing. To overcome these difficulties, timely diagnosis is crucial to effectively treat the underlying pathology and permit resumption of breastfeeding. Examination of the superficial breast plays a key role in accurate diagnosis. Traditional direct inspection is clearly inadequate for this task.
Materials and Methods:
The dermatoscope is a useful tool, enlarging and illuminating an area of epidermis to obtain an optimal image. Improvements in dermoscopy involving polarization obviate the need for full contact with the examined surface, thereby providing anatomical detail in three dimensions.
Results:
A novel practice presented in this article features clinical cases introducing this technique as it is applied to the lactating breast, conclusively distinguishing normal from abnormal and illustrating the efficacy and added diagnostic value of this approach. The dermoscope is shown to facilitate identification of the causes of nipple pain ranging from asymptomatic candidal infection to exquisitely painful, minute traumatic erosions, aiding, thereby, in diagnosis of the underlying causes of nursing difficulties. Improved wound surveillance and standardization for purposes of research documentation are additional benefits anticipated with the use of breast dermoscopy.
Conclusions:
We conclude that real-time, high-quality, magnified imaging of the lactating breast represents a recognizable advance in pursuit of a rapid and accurate technique that aids in the identification of the factors responsible for lesions affecting nursing women. Moreover, it features an already existing technology requiring little training at a reasonable cost.
Background
M
Since the advent of contact dermoscopy, first introduced into routine dermatological practice by Goldman, 5 polarized illumination has evolved, facilitating enhanced examination of cutaneous structures without immersion fluid. This tool obviates contact with the examined surface, thereby providing a three-dimensional image without distortion. Furthermore, such technology not only provides 10-fold magnification but the cross-polarized illumination also confers a sense of depth and translucency disclosing intricate detail. The increasing popularity of dermoscopy in various fields led to the present initiative to explore its potential benefits for the lactating mother.6–9
Rationale leading to dermoscopy examination of lactating women
As dermoscopic assessment of superficial skin conditions is widely used as an inherent component of physical diagnosis, 10 the breast of the lactating mother should be no exception to the rule. In this article, we share our experience examining consecutive lactating women either complaining of nipple pain or presenting with an infant afflicted by oral thrush. Examination was performed employing polarized dermoscopy with the DermLite 3GenTm (Fig. 1).

“Dermlite III hybrid” allowing illumination in cross-polarized dermoscopy with optional cellular telephone photography (3Gen LLC).
Dermoscope–smartphone-coupled examination
Classically, enhanced dermatological observation is performed through the eyepiece of the dermatoscope. If fastened to an adapter that fits onto a smartphone, single-handed focus is readily achievable. We recommend placing the patient recumbent on an examination table accessible from either side at a height adjusted for maximal convenience. The patient should then remain stationary, since any motion will result in loss of focus. Projected dermoscopy, for example, attaching the device to a cellphone (Fig. 1), allows examination while the examiner stands upright, thereby enhancing her comfort and protecting her dignity, since this positioning obviates the need for intimate proximity between the examiner's face and the patient's chest. Furthermore, other observers such as students can simultaneously observe the screen.
In addition, any part of the examination may now be recorded and with the appropriate consent, stored, allowing follow-up surveillance, medical education, consultation, or for medicolegal purposes.
Clinical experience unit dermoscopic breast examination
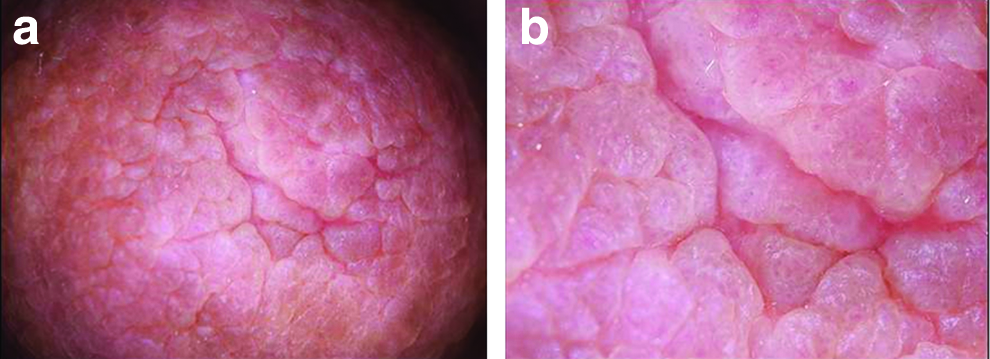
Normal surface anatomy
The nipple (papilla mammae) is typically elevated a few millimeters above the skin in the center of the areolar mammae. Each nipple contains an average of nine lactiferous ducts that end as small orifices near the tip of the nipple.11,12 There they merge, resulting in fewer ductular orifices than the respective breast lobi. The surface projections of these lactation components were magnified up to 10-fold with a dermoscope. The zoom function on the smartphone quadrupled this. At this level of resolution, the gross structure and the papillae, between which the milk is expressed, are well displayed (Fig. 2a, b). At maximal magnification, altering focus was necessary to examine separate planes of the same field. It was important to image the contour, consistency, and confluent surface of the papillae. Their color should be uniform. Superficial digitate protrusions were aligned uniformly and maintained a round contour without overlying crust produced by secretions and without irregular protrusions, indentations, or ulcers. Normal variations were observed (Fig. 3a, b). Also important were the texture of the areolar base and its confluent surface. We paid particular attention to the junction between the mammilla wall and the areola. This interface often remains moist for lengthy periods of time and is, therefore, vulnerable to infection (Fig. 4).

Normal clear surface of junction between the mammilla wall and the areola.
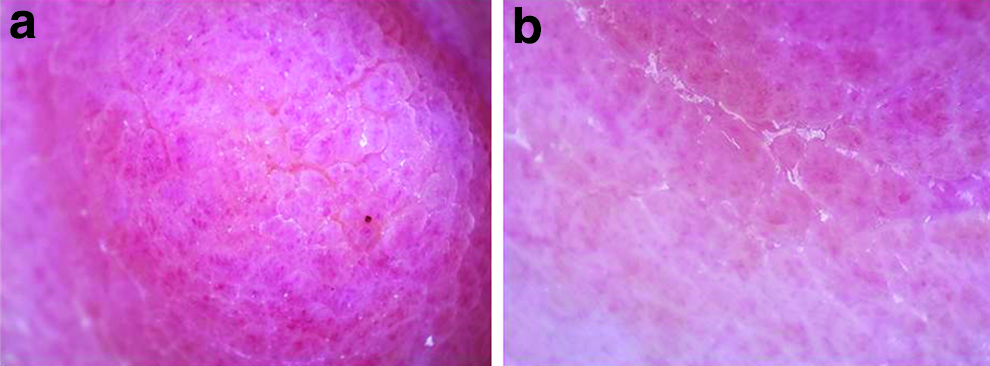
Surface variation
As already indicated, a dry nipple surface is less vulnerable to infection. Dermoscopy, however, may reveal florid scaling that is not necessarily associated with any symptoms (Fig. 5a, b). This state may reflect a natural response to the moist environment, although it suggests the need for greater vigilance for detection of a candidal infection.
Improved standardization for surveillance and research
The dermoscope glass exhibits a graded grid. At a constant, fixed focal distance from the surface, two-dimensional measurements are possible, allowing for accurate assessment of the borders and the area of inflammation or other irregularities. Subsequently, precise scientific measurement can substitute gross subjective estimates of an episode's course. A recent study demonstrating a lack of correlation between pain and wound scores calls for a development of better tools to assess tissue integrity. 13 Dermoscopy may help address this, yielding a scale for evaluation of nipple surface area involvement, grading of erythema, edema, and scab formation that will be more objective than currently used schemes.
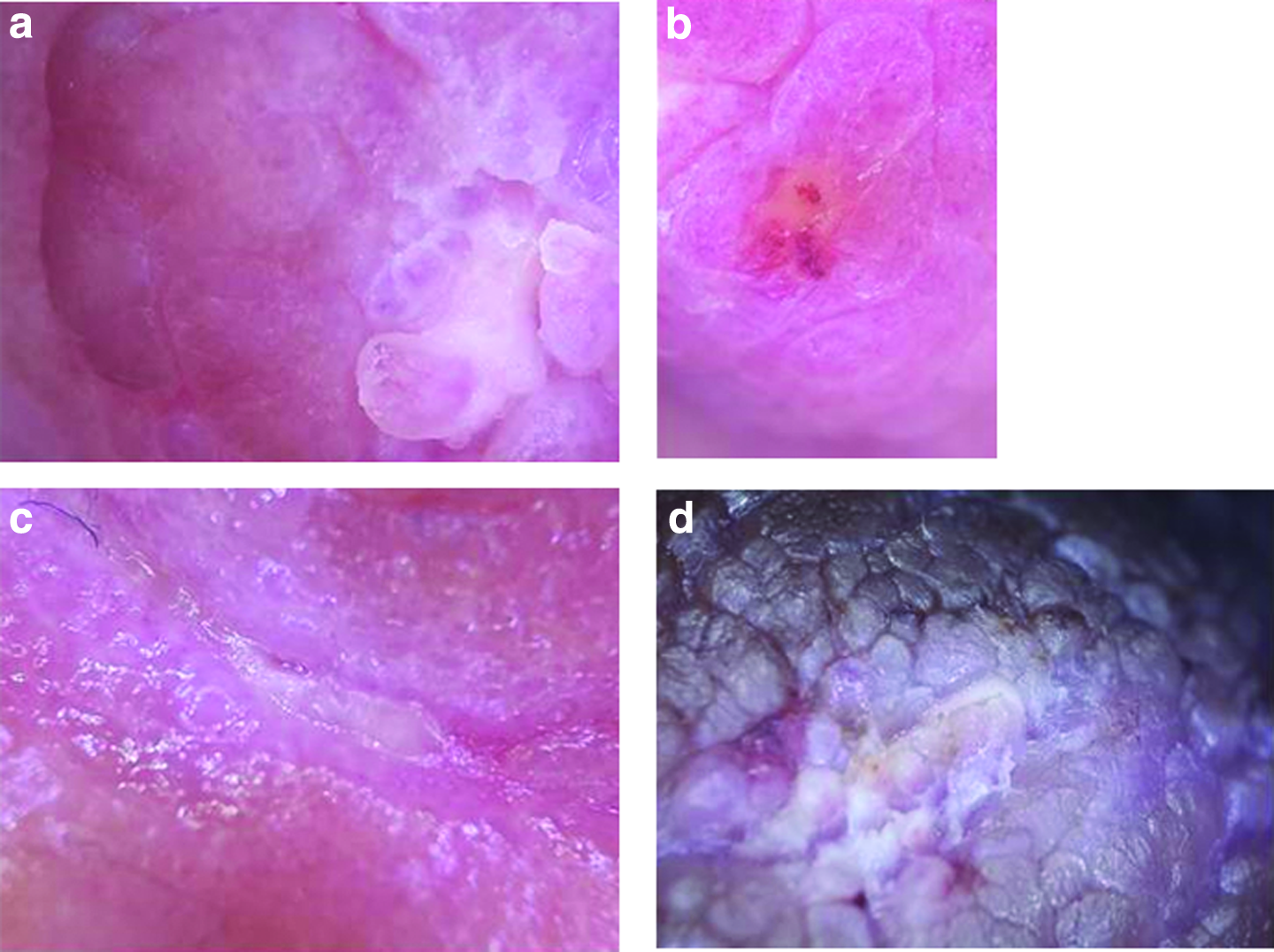
Bacterial infection
This case illustrates the findings from a woman presenting with exquisite nipple pain upon her 3-month-old baby's “latching on” and continuing without interruption as nursing continues. Dermoscopy revealed an occult finding of purulent secretion evident behind a discrete papilla (Fig. 6a). This indicated a localized, subcutaneous infection (Fig. 6b). In another case, the mother's nipple base assumed a pustule-like erosion (Fig. 6c). The infected aspect to the left exhibited hypopigmentation with macerated papillae (Fig. 6d). In both cases, topical fusidic acid cream was applied twice daily to the affected areas for a week, which led to the rapid resolution of symptoms (data not shown).
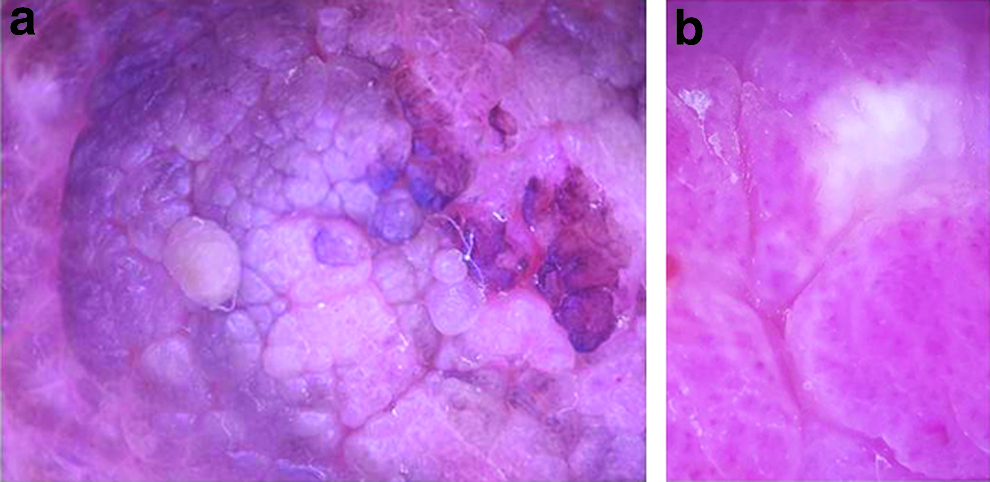
Fungal infection
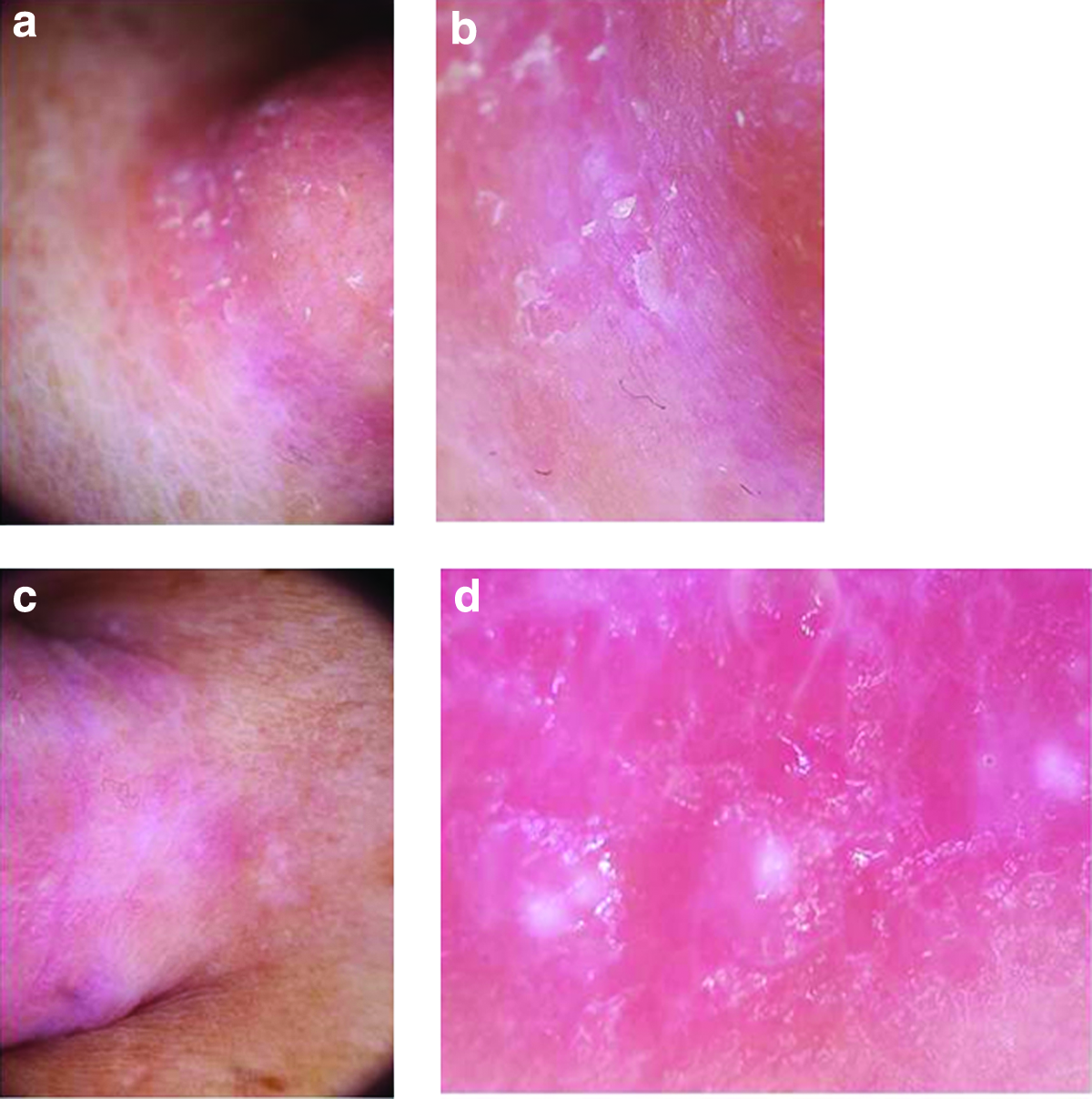
Fungal infections may be the culprit behind nursing-related nipple pain. 14 Two nursing mothers arrived at our clinic with infants presenting an overt oral thrush. Both denied any symptoms or evidence of a fungal rash involving their breasts. Dermoscopy, however, revealed obvious scaling, indicating an infection with Candida albicans. For comparison, a different aspect of the nipple on the affected side and that on the contralateral side exhibited normal surfaces (Fig. 7a–c). Another case revealed the characteristic superficial appearance of yeast (Fig. 7d). An ongoing debate questions whether the nipples in every instance of infantile thrush should automatically be treated with an antifungal agent. 15 It has been established that at least 7% of all asymptomatic nursing women harbor candida. 16 Dermoscopy may be of assistance to determine when such intervention is warranted. In such cases, topical imidazole cream is indicated, accompanied by clear instructions to maintain a dry surface. Here too a culture can be of assistance.
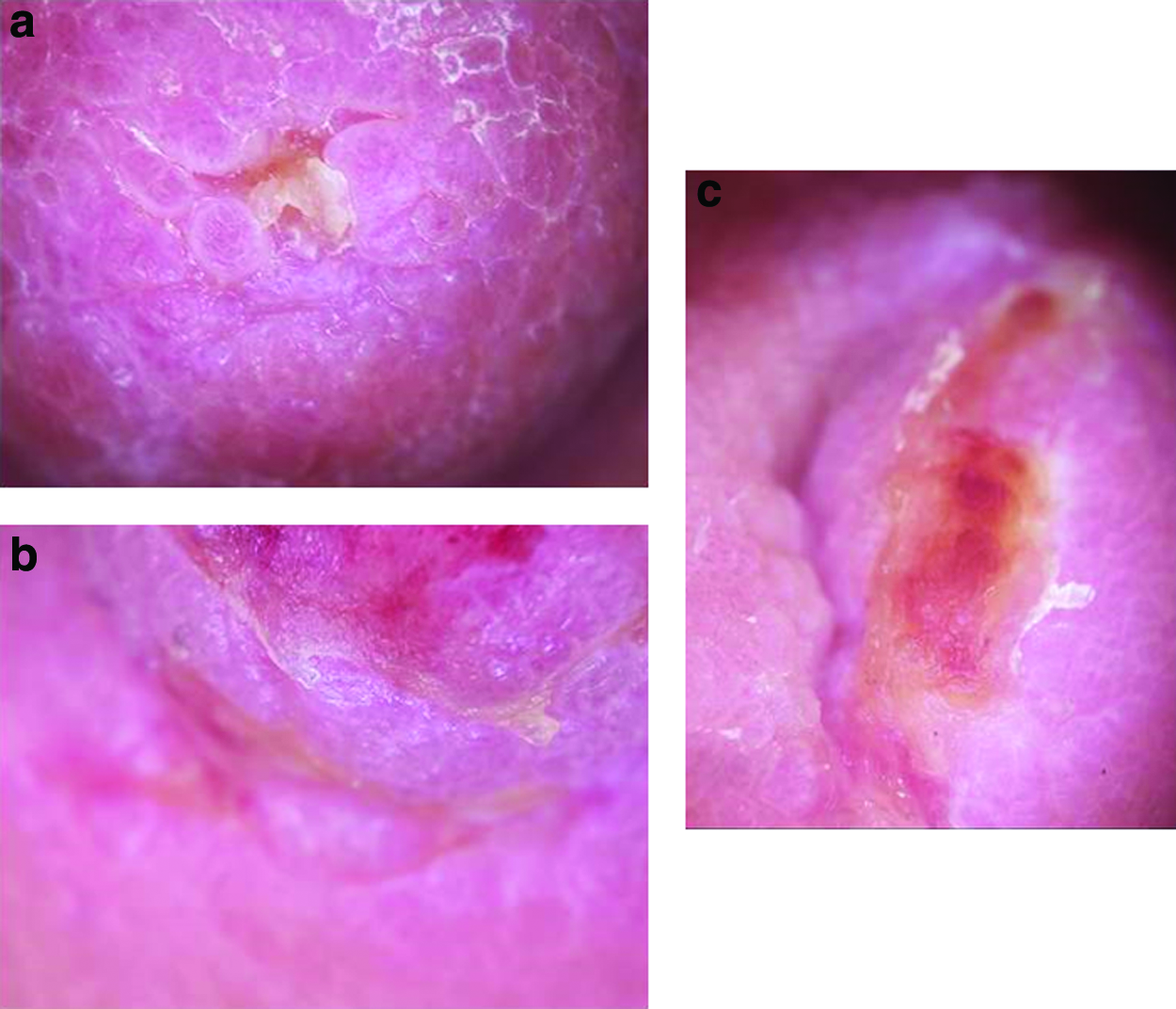
Erosions: nipple trauma
Characteristically, mechanical erosions will demonstrate superficial ulcerations. The margins, however, will be sharply demarcated, without localized inflammation or scaling as seen with bacterial or fungal infections. Two examples are shown here (Fig. 8a, b). These cases were mothers presenting the second week after delivery with inverted nipples that persistently fail to evert. The women were nevertheless determined to nurse regardless of the challenging necessity to use a pump. One, a mother of seven, exhibited a greenish, crusted secretion along the ridge of the areola, which obscured the completely inverted nipple (Fig. 8c).
Discussion
Pain associated with breastfeeding is among the most commonly cited reason for cessation of breastfeeding. 17 Engorgement, nipple trauma, and mastitis are all common in the early postpartum period and can make breastfeeding a painful, frustrating, and, ultimately, untenable experience. Although usually relieved with analgesics and topical ointments, persistent nipple pain requires prompt evaluation to prevent the mother from abandoning breastfeeding and switching to the bottle. Dermoscopy offers improved resolution over traditional, nonaugmented visual assessment of the breast, enhancing the speed and reliability needed to identify pathological events interfering with nursing. It enables the nonspecialist to distinguish normal from abnormal (sometimes subtly-so) tissue, and thereby, to quickly reach a specific, timely, and clinically useful diagnosis.
The use of dermoscopy for diagnosis of breast pathology has ample precedent, but almost exclusively in the realm of detecting neoplastic disease.18,19 Its application in nonlife-threatening conditions, for example, nursing-related nipple pain, seems almost obvious in retrospect. Indeed, examination of almost any medical problem with the integument can benefit from this simple noninvasive, dermatological advance. Our eventual aim is the preparation of an atlas containing the full spectrum of normal and pathological states for use as a reference for any physician or other health practitioner joining the growing community of dermatoscope breast examiners.
Conclusions
Dermoscopy of the nipple and breast reveals previously inaccessible detail for specialists, primary care physicians, and for other health professionals dealing with breast and nipple pain. This approach may improve speed and accuracy of diagnosis as well as provision of standardized evaluation for surveillance and research purposes. Future formal study should familiarize us with both its advantages and limitations and thus optimize its implementation in patient care.
Footnotes
Disclosure Statement
No competing financial interests exist.