
Abstract
Abstract
Objectives:
The current study sought to characterize changes in salivary oxytocin (OT) secretion patterns across the breastfeeding cycle, and to evaluate whether breastfeeding has a positive effect on mood disturbances related to postpartum depression, via endogenous OT release.
Materials and Methods:
Twenty-four primiparous mothers who delivered vaginally at term and were exclusively breastfeeding were examined 4–5 days postpartum. Salivary OT was measured using enzyme immunoassays at 30 minutes before breastfeeding (baseline), during breastfeeding (feeding), and 30 minutes after completing breastfeeding (postfeeding). In addition, maternal mood changes were evaluated at baseline and postfeeding using the Profile of Mood States (POMS) questionnaire.
Results:
OT levels rose significantly during feeding (pcorr < .05) and postfeeding (pcorr < 0.05), compared with baseline. POMS scores for Tension–Anxiety were decreased postfeeding compared with baseline (p < 0.001). This decrease was significantly associated with increased OT (feeding minus baseline: r = −0.52, rpart = −0.51, postfeeding minus baseline: r = −0.53, rpart = −0.52, ps < 0.05). POMS scores for Fatigue and Confusion also decreased, while Vigor significantly increased. Significant correlations were found between Fatigue decreases and OT increases (feeding minus baseline: r = −0.48, rpart = −0.53, postfeeding minus baseline: rpart = −0.60, ps < 0.05). This result partially contradicted with the finding of no correlation between increased Vigor and increased OT.
Conclusions:
OT is released across the breastfeeding cycle and can be detected with salivary measurement. This OT release exhibited a temporary anxiolytic-like calming effect on postpartum maternal mood disturbances.
Introduction
A
Breastfeeding and milk ejection are regulated by the neuroendocrine mechanisms of oxytocin (OT) coupled with prolactin and are triggered in response to suckling stimulation by the infant. 3 A number of studies have reported that OT modulates the functioning of the hypothalamic–pituitary–adrenal (HPA) axis and regulates stress and anxiety across a broad range of mammalian species.4–7 Several recent human studies reported an enhancement of social cognitive functioning following treatment with OT nasal administrations, finding that OT reduces social threat perception8,9 and attenuates negative cognitive responses to stress in anxious individuals.10–12 Thus, these studies raise the possibility that the protective effect of breastfeeding on postpartum depressive symptoms is mediated by endogenous OT release and its anxiolytic effects.13,14
Stuebe et al. studied 46 women at 2 weeks and 39 women at 8 weeks postpartum, reporting that plasma OT levels were significantly increased following 10 minutes of breastfeeding or expression using an electronic pump, compared with baseline. 13 In addition, the study revealed a relationship between higher depressive and anxious symptoms, and lower OT release at 8 weeks. In addition, using the same cohort samples, Cox et al. examined stress reactivity using the Trier Social Stress Test and demonstrated a significant modulation effect of OT on stress reactivity. 14 Taken together, these findings indicate that HPA axis activity may be modulated by endogenous OT release associated with breastfeeding cycles. However, to our knowledge, no previous studies have investigated whether OT release during the breastfeeding cycle affects maternal mood changes.
In most previous research, OT has been measured in plasma samples.13,14 Recently, techniques have been developed to enable the measurement of OT in saliva.15–19 However, few studies have measured salivary OT levels during breastfeeding, and contradictory results have been reported. While one study reported a decrease in salivary OT, 17 another study reported the maintenance of stable levels throughout breastfeeding. 19
In the current study, we hypothesized that salivary OT release would increase significantly during breastfeeding, particularly in the early postpartum period, since the milk ejection reflex in this period is more strongly regulated by the endocrine than the autocrine system.20–23 In addition, we hypothesized that breastfeeding would attenuate postpartum mood disturbances related to postpartum depression. To test these hypotheses, we measured salivary OT secretion patterns over the breastfeeding cycle in primiparous mothers at 4–5 days postpartum, and examined the correlations between OT release and maternal mood changes.
Materials and Methods
Participants
Twenty-four hospitalized mothers participated in this study. Participants were recruited at postpartum day 2 from the Miyamura Obstetrics and Gynecology Clinic. Mothers were eligible if they met the following criteria: (i) primiparous; (ii) currently exclusively breastfeeding their infants; and (iii) no history of mental disorders, including depression and anxiety, no current medication use, or history of psychotropic medication use. We used the following exclusion criteria: (i) recent obstetrical complication involving the mother or her infant; (ii) delivery of a preterm infant; or (iii) a delivery by cesarean section. All participants were Japanese. Among the 24 mothers, six were excluded; for three participants, the experimental procedure or assays were not performed correctly, and the other three provided insufficient saliva. Thus, 18 participants were included in the final analyses. The characteristics of the participants are presented in Table 1.
Data are shown as the mean ± standard deviation.
Values in parentheses are ranges.
All participants provided written informed consent after the purpose of the experiment had been explained. The experimental protocol was in accordance with the Declaration of Helsinki (2013) and was approved by the Ethics Committee of the Nagasaki University Graduate School of Biomedical Sciences.
Procedures
Breastfeeding and sampling sessions were conducted by female experimenters (R.N. and M.A.-N.) for ∼60 minutes between 10:00 a.m. and 12:00 p.m. in a quiet private single room in the clinic. There was no music playing, the ceiling light was turned on, and the participants and one experimenter were the only people in the room. All newborns in the clinic were scheduled for bathing at 9:00 a.m. by nurses, as a daily routine. We asked mothers to abstain from breastfeeding after the bathing, and began the experiment at 10:00 a.m. in the private room for each participant. We did not feed the infants nor were they swaddled during this time. The infant lay on a cot during this 30-minute period. Although half of the infants (n = 9/18) were observed crying before breastfeeding, as shown in Table 1, there was no significant influence on OT, when we compared OT between participants with- and without-infant crying using a t-test (baseline: p = 0.24, feeding: p = 0.72, postfeeding: p = 0.76, feeding minus baseline: p = 0.60, postfeeding minus baseline: p = 0.48, postfeeding minus feeding: p = 0.85). Participants were seated on comfortable chairs and three samples of saliva were collected over the breastfeeding cycle, using the same protocol reported by White-Traut et al., 17 to enable direct comparisons of OT secretion patterns (Supplementary Fig. S1; Supplementary materials are available online at www.liebertpub.com/bfm). The first measurement was conducted 30 minutes before breastfeeding began (baseline), the second at the initiation of breastfeeding (+5 minutes after initiation of breastfeeding [feeding]), and the third was 30 minutes after completion of breastfeeding (postfeeding). After breastfeeding was completed, most of the infants fell asleep and mothers placed them in the cot. As shown in Table 1, the third time point varied between individuals depending on the duration of breastfeeding. We did not stop breastfeeding, and as a result, we could evaluate its confounding effect in the correlation analysis. We defined Δ1 (feeding minus baseline) and Δ2 (postfeeding minus baseline) for later correlation analysis. The participants refrained from eating or drinking during the sample collection session.
Salivary OT measurements
Saliva samples were collected from the participants using cotton Salivettes® (Sarstedt, Rommelsdorft, Germany) at the baseline, feeding, and postfeeding time points. Participants were asked to place a Salivette® in their mouth and instructed to chew for 1 minute until it was saturated with saliva. The Salivettes were kept chilled on ice for up to 2 hours, before being centrifuged at 1,500 g for 15 minutes at 4°C. Because of the short half-life of OT, the protease inhibitor aprotinin (500 KIU/mL, Sigma-Aldrich, St. Louis, MO) was added to each collection tube to inhibit metabolic breakdown of the peptide. The liquid samples were stored at −80°C. Although the kit manual provides instructions for an extraction process, it is also possible to lyophilize samples, achieving a similar outcome.15,17,18,24–26 Lyophilization has also been found to significantly increase the validity of measuring saliva OT via enzyme immunoassay (EIA). 26 Therefore, we used the lyophilization process instead of the extraction process outlined in the manual. To concentrate the samples fourfold, they were lyophilized overnight 15 and kept at −20°C until they were assayed. The dry samples were reconstructed in the assay buffer immediately before analysis using OT EIA kits (Assay Designs, Inc., Ann Arbor, MI).15,17,24,25 Because the sample volume was less than 1 mL, we used a single assay to examine OT (a single assay was required for 0.5 mL). Concentrations were calculated using the SUNRISE Rainbow RC-R® microplate reader (Tecan Japan Co., Ltd., Kawasaki, Japan), using relevant standard curves. The mean intra- and interassay coefficients of variation were 7.5% and 10.0%, respectively.
Maternal mood changes assessment
Major symptoms of postpartum depression include anxiety, guilt, hopelessness, irritability, low energy, and loss of concentration. 1 We evaluated each mother's mood at the baseline and postfeeding time points using a self-report questionnaire, the Profile of Mood States (POMS)—Brief Form. 27 The POMS consists of 30 items in six scales: Tension–Anxiety (T–A), Depression–Dejection (D–D), Anger–Hostility (A–H), Vigor (V), Fatigue (F), and Confusion (C). These six axes cover the full range of symptoms of postpartum depression. Total scores were calculated for each scale with a five-step rating of 0–4 points. Higher scores on each scale indicated a stronger experience of the particular mood measured by that scale.
Statistics
To assess changes in OT levels across the breastfeeding cycle, one-way repeated-measures analysis of variance (ANOVA) was conducted. Significant F ratios were further examined using post hoc paired Student's t tests with an alpha level set at 0.017, using a Bonferroni adjustment (0.05/3). Paired Student's t tests (α = 0.05) were used to analyze POMS score changes between the baseline and postfeeding time points. Spearman correlation analyses (α = 0.05) and partial correlation analyses with adjusted duration of breastfeeding (α = 0.05) were conducted to characterize the relationship between changes in OT levels (Δ1,2OT) and changes in POMS scores (Δ2T–A, Δ2D–D, Δ2A–H, Δ2V, ΔF and Δ2C). All analyses were conducted using IBM SPSS Statistics (ver. 21; IBM Corp., Armonk, NY) and R (ver. 3.2.1) via the RStudio platform (ver. 0.99.489) using the ppcor software package. 28
Results
Salivary OT secretion patterns across the breastfeeding cycle
OT levels at baseline, feeding, and postfeeding are presented in Figure 1. One-way repeated-measures ANOVA revealed a significant difference in OT changes across the breastfeeding cycle [F (2, 34) = 8.69; p < 0.001]. OT levels rose significantly during feeding compared with baseline (pcorr = 0.011) and decreased between feeding and postfeeding, although this decrease did not reach statistical significance (pcorr = 1.00). OT levels at postfeeding remained significantly high compared with baseline (pcorr = 0.011).
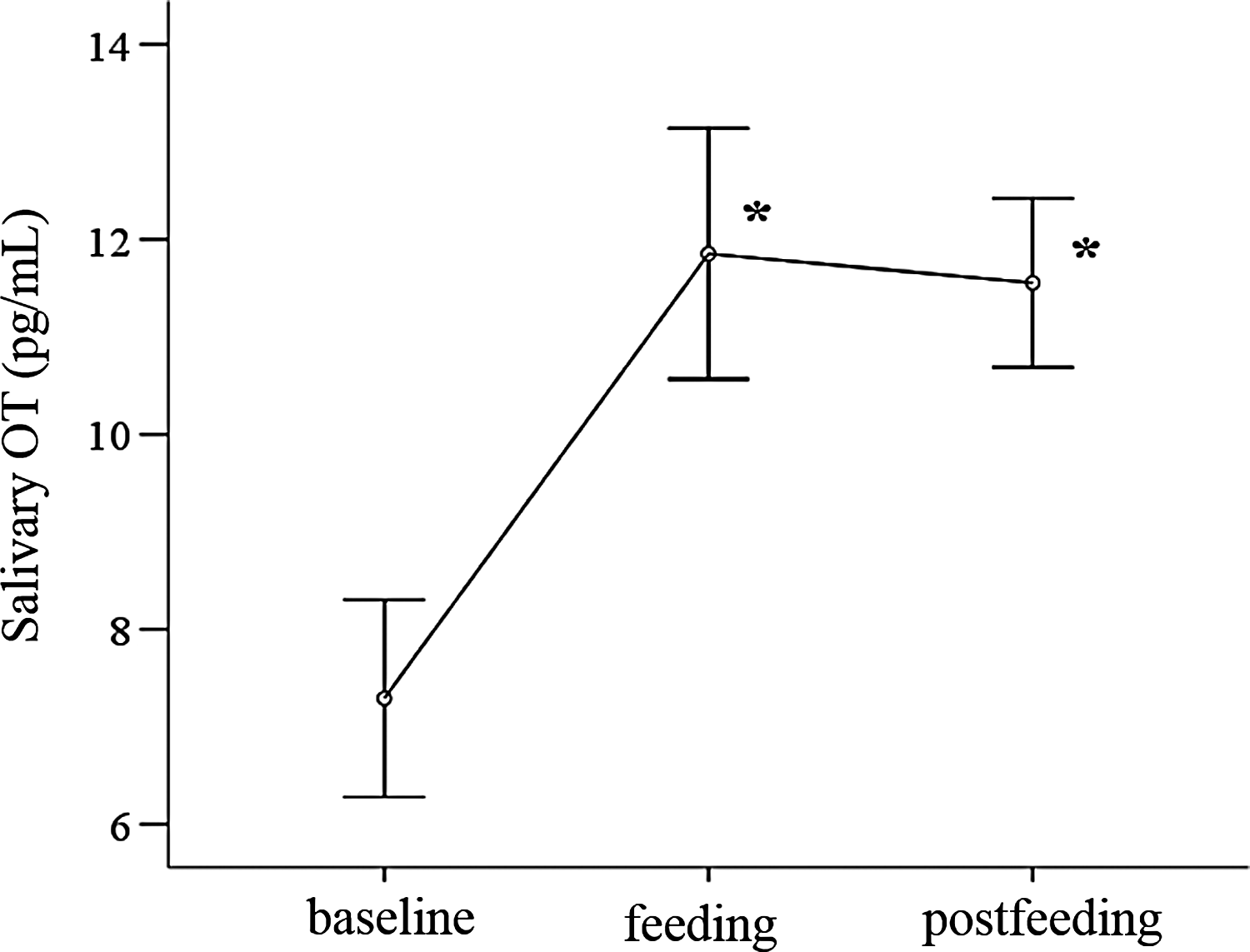
Salivary OT changes across the breastfeeding episode.
Maternal mood changes after breastfeeding
Changes in POMS scores between baseline and postfeeding are presented in Figure 2. Significant differences in POMS scores were observed for the Tension–Anxiety (T–A), Vigor (V), Fatigue (F), and Confusion (C) items. Scores for T–A [t (17) = −4.8, p < 0.001], F [t (17) = −3.3, p < 0.005], and C [t (17) = −2.6, p < 0.05] decreased significantly. Scores for V [t (17) = 2.3, p < 0.05] showed a significant increase. However, neither scores for Depression–Dejection (D–D) [t (17) = −1.6, p = 0.14] nor Anger–Hostility (A–H) [t (17) = −1.4, p = 0.19] exhibited any significant change.
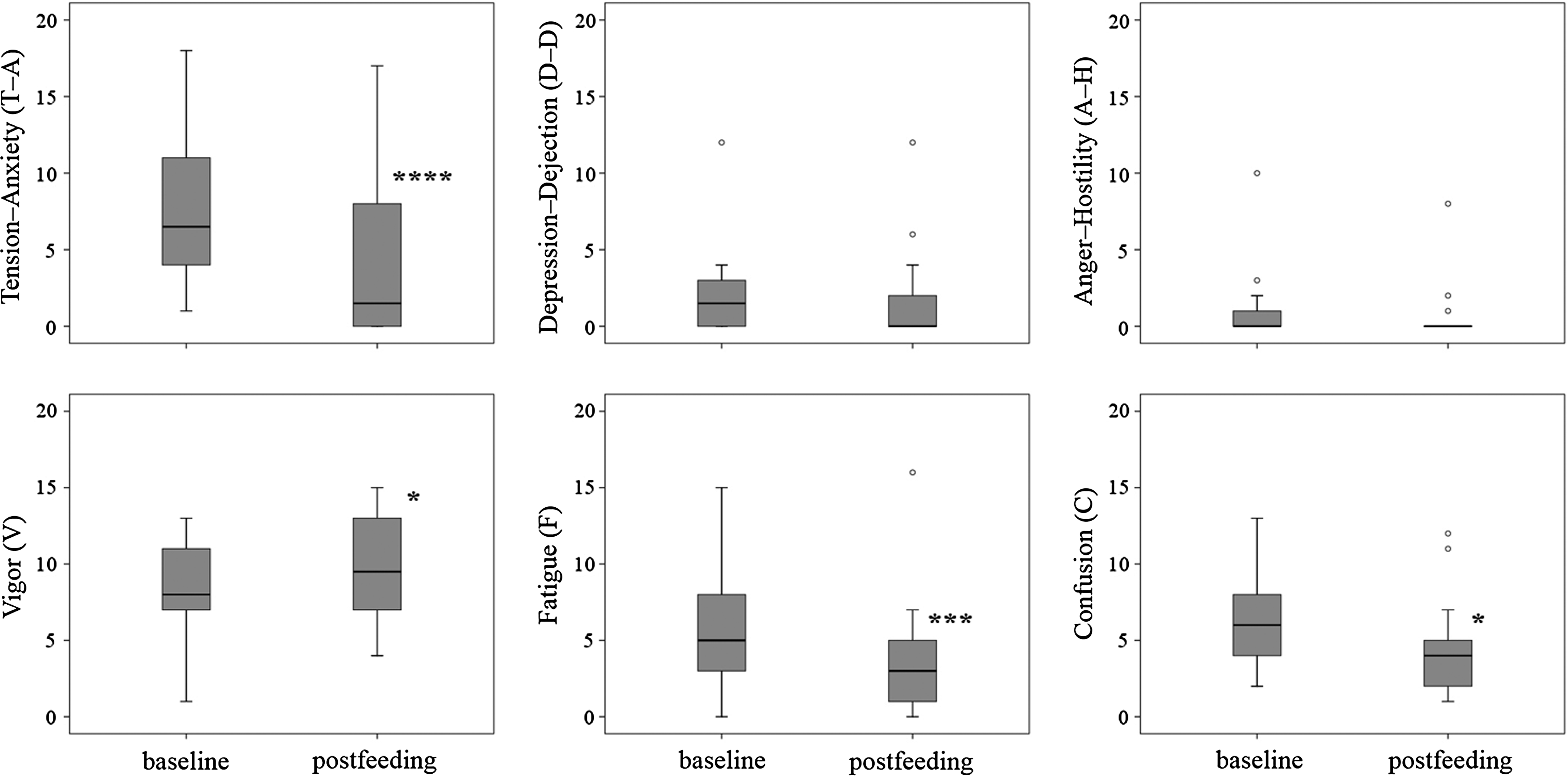
Box-and-whisker plot for maternal mood changes across breastfeeding. Open circle (○) indicates outliers. ****p < 0.001, ***p < 0.005, *p < 0.05.
Correlations between Δ1,2OT and changes in POMS scores
As shown in Table 2, Δ2 Tension–Anxiety (T–A) was significantly correlated with both Δ1OT and Δ2OT, regardless of adjustment (Fig. 3A–D). In addition, Δ2 Fatigue (F) was significantly correlated with Δ1OT and both Δ1OT and Δ2OT when adjusted (Fig. 3E, F, and H). No other correlations were significant.
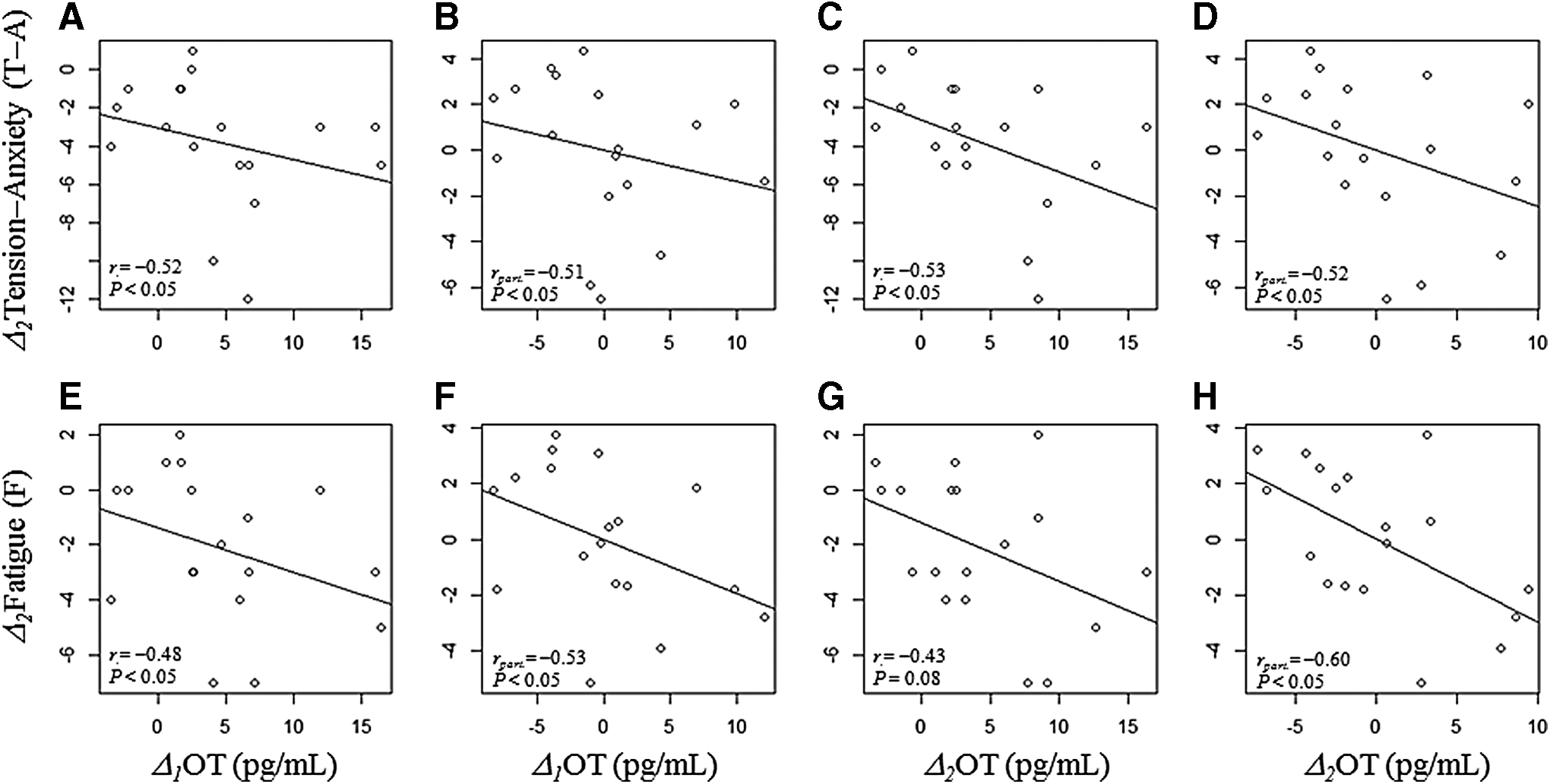
Scatter plots for correlation analysis
Spearman r and rpart coefficients with p < 0.05 are shown in bold. rpart, partial correlation coefficient adjusted by duration of breastfeeding.
Discussion
Salivary OT secretion patterns across the breastfeeding cycle
The current study revealed that salivary OT levels significantly increased as a result of breastfeeding within 5 minutes after the onset of infant suckling, and did not return to the baseline level for up to 30 minutes after the completion of breastfeeding (50.5 ± 6.1 minutes from the onset) in exclusive breastfeeding primiparous mothers at postpartum days 4–5. These findings are in contrast with those of other recent studies measuring salivary OT.15,17,19
There are several potential causes underlying the discrepancy between the current results and previous reports. First, as suggested by the current data, postpartum time would be expected to substantially influence OT secretion patterns across the breastfeeding cycle. White-Traut et al. 17 measured the salivary OT levels of 11 women, reporting that OT levels were highest 30 minutes before suckling, decreased during breastfeeding, and then rose slightly 30 minutes after breastfeeding. Jong et al. 19 measured the salivary OT levels of four women, reporting that the levels did not change in response to 10 minutes of nursing or 60 minutes after infants started suckling. However, unlike the present study, the mean number of months postpartum varied widely among the participants (3.7 ± 2.1 months and less than 4 months, respectively). This difference may have substantially influenced the trends in salivary OT levels. In contrast to these previous saliva OT studies, Stuebe et al. 13 measured both plasma OT and prolactin during breastfeeding or milk expressed using an electronic pump at both 2 and 8 weeks postpartum, reporting similar OT levels at both time points, while prolactin levels were significantly reduced at 8 weeks compared with 2 weeks postpartum. The link between breastfeeding and reduced prolactin release has been well established and is reported to depend on development in the postpartum months. Specifically, this decline in prolactin release has been found to correspond with the development of autocrine regulation, in which the production of breast milk is suppressed in response to increased internal mammary gland pressure when milk accumulates.20–23 Conversely, during this time, the production of breast milk has been reported to increase in response to a decrease in internal mammary gland pressure when the acini are emptied. Thus, postpartum OT regulation might be influenced by the interaction of prolactin secretion pattern changes and the development of autocrine regulation. Based on this assumption, the OT secretion pattern reported by White-Traut et al. 17 and Jong et al. 19 might represent this autocrine regulation cycle. In contrast, the period at 4–5 days postpartum in the mothers examined in the current study would presumably be an endocrine-regulated period in which milk production is promoted by the secretion of prolactin from the anterior pituitary gland, and by posterior pituitary gland-derived OT secreted in response to the suckling stimulus, resulting in milk ejection.21,22,29
Another possibility is that homogeneity of the participants in the current study, compared with previous experiments, might have contributed to discrepancies in the results. The present study sample was limited to primiparous mothers. In contrast, approximately half of the participants in a study by White-Traut et al. 17 were multiparous mothers, and a study by Jong et al. 19 did not distinguish between multiparous and primiparous mothers in their sample. Moreover, one previous study suggested that multiparous mothers are typically more prone to establishing autocrine regulation of lactation, compared with primiparous women. 30 Thus, this difference may have also influenced the interaction between the OT secretion pattern and postpartum time. This possibility should be tested in future research.
Maternal mood changes after breastfeeding
Scores on the Tension–Anxiety (T–A), Fatigue (F), and Confusion (C) items in the POMS questionnaire decreased significantly postfeeding compared with baseline, while scores for Vigor (V) rose significantly. This indicates that the act of breastfeeding was associated with a more calming and energetic state for mothers, and an increased ability to concentrate. In contrast, scores on the Depression–Dejection (D–D) and Anger–Hostility (A–H) items were unchanged after breastfeeding. This finding may have been due to participants in the present study being a sample of healthy participants, meaning that the baseline scores for those items were relatively low and stable. Accordingly, we were unable to find any effect of OT on improving depressive mood or irritability in this study design.
Associations between OT release and maternal mood changes
The current findings revealed that Tension–Anxiety (T–A) scores significantly decreased after breastfeeding, suggesting that a calming effect may have been caused by OT release triggered by breastfeeding. In animal studies, the anxiolytic effects of OT have been investigated extensively.4,31–33 Although a number of human studies have examined the therapeutic effects of intranasal OT administration, they have typically been conducted among male subjects,8–12 in part, because variations in gonadal steroids during the female menstrual cycle can modulate the effects of OT on mood. However, one clinical trial of nasal OT for women with postpartum depression has been conducted, reporting that OT decreased maternal happiness and caused women to describe their infants more negatively. 34 Furthermore, there is evidence suggesting that the impact of OT is modulated by early parental separation, 35 and that genetic variations in OT may affect associations between early childhood trauma, breastfeeding, and depression. 36 Thus, the potential anxiolytic effects of nasal OT for postpartum women remains controversial. Future research is required to further understand the link between nasal OT and mood, including investigations of dose-dependent effects. 37 To our knowledge, no previous reports have examined whether the endogenous OT release across breastfeeding has an effect on postpartum anxiety. The current findings indicate that endogenous OT release across the breastfeeding cycle may have a preventative effect on severe mood disturbance among mothers, via an anxiolytic-like calming effect. In addition, we found that the Fatigue (F) scores were decreased and were associated with OT release. Moreover, the effect on participants' energy levels may also be a positive effect of OT, because intranasal OT administration has been reported to reduce fatigue in older adults, compared with placebo treatment. 38 In contrast, the current results revealed that the Vigor (V) score was increased throughout breastfeeding, but this effect on energy levels was not mediated by OT release. Thus, this result does not correspond with an effect of fatigue reduction. These results suggest that the effects of OT on energy levels may be partial and limited to reducing the feeling of fatigue.
Limitations
The current study involved several limitations that should be considered. First, we did not evaluate any simultaneous episodic or pulsatile OT secretion patterns in response to infant suckling, because of the limited sampling frequency. However, salivary OT measurement during breastfeeding may be a useful index to evaluate the oxytocinergic and milk ejection functions among postpartum mothers. Second, we measured salivary OT using a nonextractive method, in accord with a previous report.15,17 There is considerable controversy in the literature regarding the optimal method for measuring OT, particularly the role of extraction in the processing of samples to quantify the active peptide. Although some previous studies measuring unextracted OT have reported associations with some social behaviors,18,19,24–26 unextracted OT values are not correlated with extracted OT values,26,39 raising the concern that unextracted OT may not provide a biologically relevant measurement. Further studies using extracted OT should be conducted to confirm the current findings. Third, we excluded multiparous mothers from the experiment. Multiparous mothers have been found to establish autocrine regulation of breastfeeding as early as 4–5 days postpartum,20–23 which may affect the results. Future studies are required to test this possibility. Fourth, as described above, we did not exclude the possibility that the observed calming effect and OT release are caused by infant cues other than suckling, including various visual and tactile cues. Future studies involving a range of experimental control conditions, such as the mother holding the infant without breastfeeding, or in which the infant is bottle-fed, should be conducted to rule out the effects of potentially confounding variables. Fifth, the participants in the present study were healthy mothers. Clinical studies examining participants at high risk of postpartum depression may help to clarify the present results. Sixth, we did not correct for multiple testing in the correlation analyses. Applying a more strict correction in future studies may help to confirm the robustness of the current findings. Seventh, the current study reported the results of a partial correlation analysis, adjusted for breastfeeding duration. However, it is possible that OT at feeding may have affected subsequent breastfeeding duration, and therefore, duration may mediate the association between OT at feeding and subsequent duration. Adjusting for a mediator may produce biased results, reducing the internal validity of the study, but was required to adjust for changes in POMS scores because mood changes evaluated by POMS would be expected to be affected by the duration as the second time questionnaire was conducted at postfeeding. Finally, we did not examine the influence of mode of delivery. Mothers undergoing delivery by cesarean section would not be exposed to OT surges during delivery, and this may have also influenced the OT secretion pattern across breastfeeding in the present experiment phase.
Conclusion
The current study revealed differences in salivary OT levels between baseline, feeding, and postfeeding time points, confirming that the widely accepted notion that OT is released as a result of infant suckling also applies to salivary OT in early postpartum primiparous mothers. In addition, increased OT levels were found to persist for at least 30 minutes after the completion of breastfeeding, regardless of overall duration. Moreover, we found that breastfeeding exhibited a temporary anxiolytic-like calming and energetic effect on maternal mood disturbances, associated with OT release. This study provides support for the value of early postpartum breastfeeding.
Footnotes
Acknowledgments
This work was supported by a KAKENHI Grant-in-Aid for Scientific Research (C), (25463477 to M.A.-N.). We are grateful to the medical staff of the Miyamura Obstetrics and Gynecology Clinic for technical assistance. We are also grateful to Dawayland Cobb for help preparing the manuscript.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.