
Abstract
Abstract
Background:
Neonatal hypernatremic dehydration (NHD) is a dangerous condition that can lead to severe weight loss, renal impairment, and central nervous system complications. We aimed to evaluate the consequences of NHD in infants in their second year of life.
Materials and Methods:
This was a prospective case–control study in Ghaem hospital, Mashhad, Iran. Sixty-five healthy breastfed neonates (serum sodium concentration <150 mmol/L) and 65 hypernatremic (serum sodium concentration ≥150 mmol/L) neonates were followed up from 2008 to 2011. Maternal and neonatal factors were compared between the two groups together with their growth parameters, and developmental milestones (using Denver II developmental assessment scores) were assessed and compared in ages 6, 12, 18, and 24 months, respectively.
Results:
The weight of infants at 6 months of age was significantly different between the two groups (7,264 ± 1,089 g vs. 7,596 ± 957 g, p = 0.009). Twenty-five percent of infants in the group who had developed NHD had a delay in development at 6 months of age, with corresponding values of 21% at 12 months, 19% at 18 months, and 12% at 24 months of age. Developmental delay was ∼0.3% for the control group at similar ages. The severity of hypernatremia was strongly correlated with poor developmental outcome at 6 months (p = 0.001). Serum sodium concentration of neonates was 153–195 mg/dL in the NHD group. Median peak serum sodium was 158 ± 16 in case group and 141 ± 9 in control group. Serious complications were cerebral edema (five cases), hemorrhage (five cases), and kidney stones (six cases).
Hypernatremic dehydration has an adverse effect on child development especially in the first year of life, their prevalence decreases with advanced age. Growth problems are also present during their first year of life. The major signs and symptoms of infants with poor prognosis on admission were poor feeding (8 infants, 61.5%), seizure (3 infants, 23.1%), hyperthermia (1 infant, 7.7%), and lethargy (1 infant, 7.7%).
Conclusions:
NHD affects growth parameters and developmental milestones of children. Occasionally the child's weight gain was normalized by the end of first year of life; although developmental delay continued, its severity was reduced, with age.
Introduction
N
Subjects and Methods
This case–control study was performed on neonates admitted to Ghaem hospital's Pediatric Emergency and Neonatal Intensive Care Unit (NICU) between 2008 and 2011 in Mashhad, Iran. The case group consisted of 65 neonates admitted with serum sodium concentrations ≥150 mmol/L and control group consisted of 65 neonates, who were assessed for jaundice, and their serum sodium concentration was <150 mmol/L and their serum bilirubin level <17 μmol/L.
The study group was admitted to the hospital and the control group was not. The study group was conducted from 2008 to 2011, but the same number of controls was enrolled for comparison.
A physical examination was performed on admission, and demographic data, birth weight, weight on admission, gestational age, APGAR score, duration of hospitalization, presence of anomaly, signs and symptoms on admission, feeding history, use of any supplement, frequency of urination and defecation, breast problems, maternal age and medical problems, mode of delivery, laboratory data (serum sodium, potassium, urea, creatinine, and glucose), and imaging studies (brain CT scan and kidney and urinary system sonography if done) were all recorded.
Infants were followed up at 6, 12, 18, and 24 months of age, respectively, for their growth and development. Their weight, length, and head circumference were measured and recorded, and their development was assessed using the Denver II Developmental Assessment. The Ethics Committee of Mashhad University of Medical Sciences approved this study and all parents of patients signed informed consent.
Denver developmental screening test
The Denver developmental screening test (DDST), 6 commonly known as the Denver Scale, is a test for screening cognitive and behavioral problems in preschool children. Denver II is a tool for screening of developmental milestones between 0 and 6 years. The test screens the child in four areas: personal social, fine motor, gross motor, and language. The Denver II is a revision and update of the DDST. Its interpretation was slightly modified from the DDST giving greater emphasis to a comparison of the child's performance. The scale reflects what percentage of a certain age group is able to perform a certain task. Denver Scale is not a tool for final diagnosis, but a rapid method to process large numbers of children to identify those that should be further evaluated. The tests cover four general functions: personal social (such as smiling), fine motor adaptive (such as grasping and drawing), language (such as combining words), and gross motor (such as walking).A child fails a Denver screen if he or she has a delay in any of the above domains. If the child has a delay in one domain, this is considered to be a mild developmental delay, if in two areas this is classified as moderate developmental delay, and if in three or more domains, this was considered severe developmental delay.
Neonates with NHD with normal development or mild impairment were considered as acceptable prognosis. Neonates who had died or with moderate-to-severe developmental disorders are defined as a group with poor prognosis.
After a diagnosis of hypernatremia was made, the neonate was followed up for the 2-year duration of the study.
Statistical analysis
Statistical analysis was carried out using the SPSS 16.5 statistical package. The Student's t test and Chi-square test were performed on quantitative and qualitative variables. p-Value less than 0.05 was considered statistically significant.
Results
Sixty-five hypernatremic neonates and 65 healthy breastfed neonates were followed up for 2 years as case and control groups, respectively. The mean age of neonates at onset of NHD in case group was 8 days old. Mean percentage weight loss compared to birth weight in the case group was 14% vs. 6.3% for control group (p = 0.01). The weight of infants at 6 months of age was significantly different between the two groups (7,264 ± 1,089 g vs. 7,596 ± 957 g, p = 0.009).
The most common complaint for seeking medical attention was poor feeding. Hyperthermia and jaundice were the next most common reasons for seeking support. Clinical features of the hypernatremic neonates on admission were as follows: weight loss (67%), poor feeding (45%), hyperthermia (38.5%), jaundice (36.9%), lethargy (36.9%), dry mucus membranes (32%), irritability (21.5%), depressed fontanels (20%), seizure (20%), decreased level of consciousness (9.2%), cyanosis (3.1%), and apnea (3%).
Serum sodium level of neonates was 153–195 mmol/L in case group and urea and creatinine was 12–374 and 0.1–6.3 μmol/L, respectively. The level of bilirubin was 14.83 ± 2.91 μmol/L.
There was no significant association between the presence of hypernatremia and time of initiation of breastfeeding, maternal age, problems during pregnancy, and duration of breastfeeding (p > 0.05, Table 1), but the incidence of hypernatremia was significantly related to the use of supplement feeding (camelthorn, flix weld, and glucose water) besides breast milk, absence of let down reflex, inappropriate breast growth during pregnancy, mastitis, frequency of breastfeeding, and frequency of micturition (p < 0.05, Table 1).
Birth weight and neonatal weight expressed as mean ± standard deviation and other variables expressed as median ± IQR.
NHD, neonatal hypernatremic dehydration.
The mean weight of infants at 6 months was significantly different between the groups (p = 0.009).
The median weight of control group (6 months age) was 7,600 g with IQr = 70 g and in case group was 7,450 g with IQr = 100 g (p = 0.632). The median height of control group (6 months age) was 68 cm with IQr = 4 cm and in case group was 67 cm with IQr = 4 cm (p = 0.241). The average head circumference of control group (6 months age) was 44 (2) and in case group was 44 cm (2.5) (p = 0.792).
The median weight of control group (12 months age) was 10,500 g (80) and in case group was 10,000 g (77) (p = 0.457). The median height of control group (12 months age) was 75 cm (2) and in the case group was 75 cm (3.25) (p = 0.44). The average head circumference of control group (12 months age) was 47 (1) and in case group was 47 (1). There is not a significant difference between neonates with 18 and 24 months age in terms of height, weight, and head circumference.
Head circumference and length were not significantly different between groups. By the age of 12, 18, and 24 months none of the growth parameters (weight, length, and head circumference) were statistically different between the groups (p > 0.1).
Neonatal growth and development of 65 neonates in the control group and 65 of those with a history of NHD were evaluated at 6, 12, 18, and 24 months of age. All infants in the control group were developmentally normal at ages 6 and 12 months, but in the case group 25% and 21% had developmental delay at 6 and 12 months, respectively. At 18 months the incidence of developmental delay was 3% for the control group and 19% for case group, and at 24 months 12% of case infants had developmental delay versus none for the case group (Table 3). At the age of 6 months, the severity of developmental delay was directly related to the severity of hypernatremia (p = 0.001).
Infants with NHD were divided into two groups according to the results of their 6-month follow-up. Acceptable prognosis (53 infants) for those who had normal developmental delay and poor prognosis (13 infants) for those who had moderate-to-severe developmental delay or who died because of complications of hypernatremia and after that the risk factors between these two groups were compared (Table 2).
Values are expressed as median and interquartile range and number (%) for categorical data.
Poor prognosis, those who had moderate-to-severe developmental delay or who died because of complications of hypernatremia.
Acceptable prognosis, those who had mild developmental delay.
CT scan was performed in 39 of the cases. The results showed 5 cases with bleeding (12.8%), 29 healthy (74%), and 5 cases with cerebral edema (Table 4). CT scans were performed in the second to fourth day of treatment. This cerebral edema can be complications of treatment. Sonography of urinary tract was performed in 45 of the cases. The results showed 36 normal cases, 6 cases with kidney stones (15.4%), and 3 cases with hyperechogenicity of cortex (7.7%) (Figs. 1 and 2).
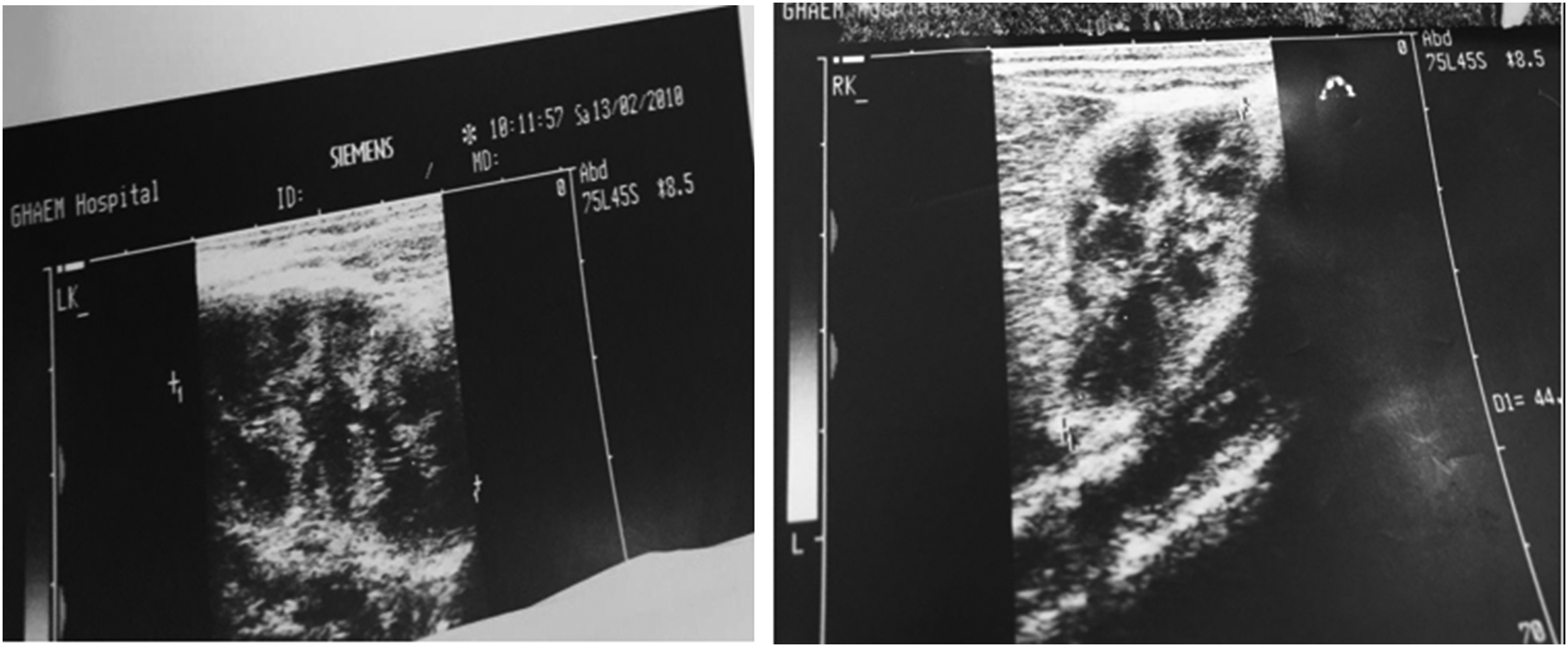
In this neonate, echogenicity of the renal parenchyma increased and the pyramid of kidneys are prominent.
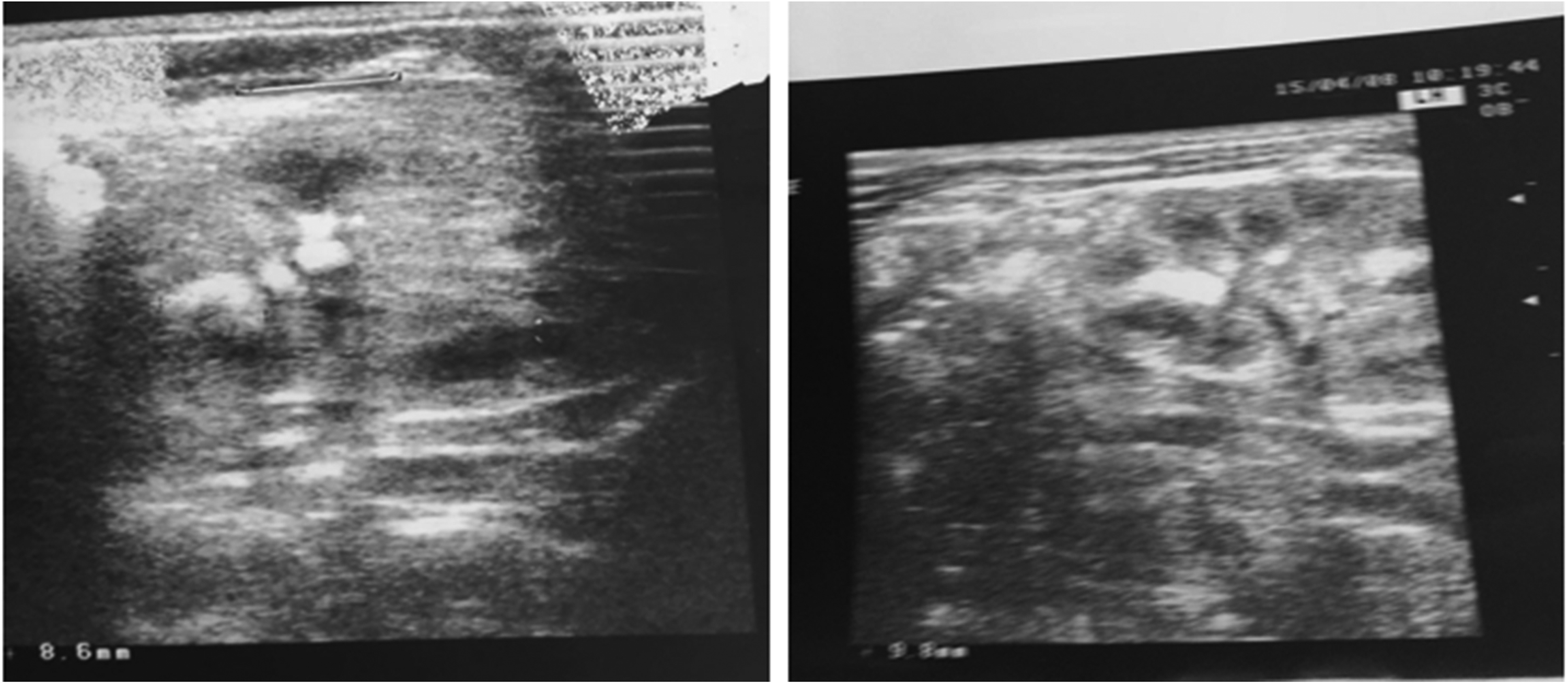
In this neonate, dimension and echo of the kidney is normal. Multiple stones in both kidneys are observed; the largest stone is 6 mm.
Long-term neurologic delay means that the child at the age of 2 years had developmental retardation of at least two from four Denver (gross motor, fine motor, speech, and Social). For example, baby at 2 years has a delay in speech, impaired walking, and seizures.
Abnormalities on brain CT scan (hemorrhage or edema) were significantly different between two groups and were more frequent in the group poor prognosis (p < 0.001). The major signs and symptoms of infants with poor prognosis on admission were poor feeding (8 infants, 61.5%), seizure (3 infants, 23.1%), hyperthermia (1 infant, 7.7%), and lethargy (1 infant, 7.7%).
Discussion
The main finding of this study was that hypernatremic dehydration has an adverse effect on child development over a period of 24 months. Although these complications are more frequent during the first year of life, their prevalence decreases with advanced age. Growth problems are also present during their first year of life.
Our data show that neonates with NHD are brought to clinic by the end of their first week of life. Gomez et al, 7 report the mean age of neonates was 4 days, and in the study of Jarcan et al. 8 it was 6.2 days, which is similar to ours. In other studies the time of presentation has been reported to be between 6 and 21 days and it seems that evaluation of feeding techniques and examination of neonates by a neonatologist between their 3 and 5 days of life lead to the early detection of any problems and helps in preventing NHD.2,4
The most prevalent sign in infants of case group in our study was weight loss. Severe weight loss (>10%) was seen in 67% of patients. This could be due to family's inattention or lack of knowledge about its importance or could be due to inattention to neonate's weight status during visits by physicians. Frequent weighing of breastfed infants during their first week of life especially their first 3–5 days may decrease the incidence of NHD. In a study by Moritz et al. weight loss of more than 10% was reported in 73% of neonates with NHD. 1 It is of interest that in our study parents did not notice their neonate's weight loss and it was noted while admitting to the hospital.
We found a significant positive relationship between the severity of weight loss and severity of hypernatremia. In studies by Moritz 1 there was also a positive association between severity of weight loss and severity of hypernatremia. So it seems that early detection of weight loss in neonates can prevent severe weight loss and severe hypernatremia. Uras et al. 10 found that a weight loss of greater than 7% of birth weight was also associated with an increased risk of hypernatremia. In our study neonates with serum sodium concentration >170 mmol/L had the greatest degree of weight loss. In a study 60% babies had both hyperthermia and excessive weight loss. 11
In a previous study, there was a relationship between the severities of weight loss and hypernatremia.9,12 Another study recommended that serum sodium should be measured in weight loss of more than 7% and the baby to be evaluated in terms of hypernatremia and renal failure. 13 Difference of our results was due to neonates who later went to doctor and higher level of sodium in neonates. Our baby had worse prognosis of these studies. Deneuve was our assessment methodology that was different from these studies. Our case in this study was referred later than these studies, and medium level of sodium in neonates with poor prognosis was 173 that show severe symptoms of hypernatremia. These studies did not follow their infants after discharge and had no discussion about the development and growth of babies in their articles, while the main goal of this study was the long-term prognosis of these infants.
The importance of frequent neonatal weighing during their first week of life to prevent excessive weight loss and its complications is clearly evident.
In this study 40% of neonates with NHD had high serum creatinine values (>1 mg/dL). Mortality was confined to these infants. Unal et al. found that 80% of hypernatremic neonates had acute renal failure, 5 which is more frequent than what we have found; this difference may be attributable to different sampling methods. Renal failure can cause acid–base and fluid and electrolyte disturbances, hypertension, and intracranial complications and can lead to increased mortality and morbidity. More than 12% of our hypernatremic neonates had intracranial hemorrhage, and 12.8% had cerebral edema, which is similar to the previous studies, 4 although Unal et al. 5 reported this to be approximately 4%. According to Musapasaoglu et al., severe hypernatremic dehydration causes serious neurological complications in neonates. The main brain problems were: cerebral edema, intracranial hemorrhage, thrombosis, bleeding infarction, and sustained damage in brain. 14
The higher prevalence of intracranial complications in our study may be due to the more severe hypernatremia and also late presentation of our patients. It has been reported previously that a serum sodium concentration ≥158 mmol/L is associated with a high mortality rate. 15 Acute brain injury is reported in 8% of patients with hypernatremia. 16 Increased serum osmolality due to hypernatremia can cause brain injury with widespread hemorrhage, thrombosis, and subdural effusion, which lead to death or permanent neurologic sequelae. 17 One-fifth of our neonates had seizure, and 9% had decreased level of consciousness. Seizures are common in hypernatremic patients even in the absence of pathologic findings. Seizure usually occurs during treatment, while serum sodium concentrations are returning to normal. Seizures may also occur due to increased osmolality within brain cells as a result of hypernatremic dehydration. 4 Too rapid a decrease of extracellular fluid osmolality due to a change in serum sodium concentration and other active osmotic agents like glucose leads to a shift of fluid into brain cells causing brain edema. This edema is sometimes irreversible and lethal. Brain edema may also ensue during correction of hypernatremia or as a result of using isotonic fluids for correcting dehydration. Slow correction of hypernatremia gradually over several days can limit such complications.
Weight gain was significantly lower in the NHD group at the age of 6 months (p = 0.009). Length and head circumference did not show any significant difference. In addition none of the growth parameters were statistically different at the ages 12, 18, and 24 months. So it seems that hypernatremic dehydration may adversely affect weight gain during the first months of life, which seems to be transient and is corrected by 12 months of age according to our findings. So we can conclude that infants with a history of hypernatremic dehydration catch up their growth with increasing age and reach their normal values. We could not find any similar study on this subject. In a study by Kuklo and Gunes, 3 developmental delay was reported to be 51% in hypernatremic infants at 12 months of age. In our study developmental delay was less than this. In comparison with the study of Ebru et al. 2 in Turkey who followed 15 hypernatremic neonates to 6 months of age, 6 (40%) had moderate developmental delay and one (6%) had severe developmental delay. The incidence of developmental delay was less in our study, which can be due to our greater sample size, long-term follow-up, neonates with more severe hypernatremia, or use of different tools for developmental screening (Denver II in our study vs. BSIDI). However, about severe developmental delay, the two studies were similar.
In our study developmental delay was significantly different between the two groups at all ages. Besides, there was a significant correlation between severity of developmental delay and severity of hypernatremia at 6 months (p = 0.001). So, cases of severe hypernatremic dehydration (Na >160) are more prone to long-term complications and mandate more careful follow-up. In a study by Gabriel and Scobar 106 neonates with dehydration (weight loss ≥12%) and serum sodium concentration ≥150 mmol/L were followed up for 5 years and compared them with 419 control children. They found no significant difference between case and control groups in cognitive tests and neurologic and behavioral problems, which is different from our findings. This can be due to difference in severity of hypernatremia. In Gabriel and Scobar study, only 6.6% of patients had Na >160 mmol/L.
In our study 7 out of 65 patients died as a result of complications of hypernatremia. There was a significant correlation between severity of hypernatremia and mortality (p = 0.001). All who died had serum sodium concentration >160 mmol/L. We could also find that the degree of weight loss in the first 10 days of life, serum sodium concentration, and serum creatinine values were correlated to poor developmental outcomes. In addition, abnormal findings on brain CT scan (edema or hemorrhage) were in significant relation to developmental delay or mortality. So, serum sodium concentrations, serum creatinine values, and degree of weight loss are important prognostic factors that should be evaluated on admission, and detection of any abnormality on brain CT scan is associated with poor developmental outcomes and increased mortality. Our limitations were inability to accurately assess the pregnancy problems and inability to accurately estimate the amount of milk that was received by each baby.
Conclusions
NHD affects growth parameters and developmental milestones of children. Occasionally the child's weight gain was normalized by the end of first year of life; although developmental delay continued, its severity was reduced, with age.
Footnotes
Acknowledgments
This study was kindly supported by the Vice-Chancellor for Research of Mashhad University of Medical Sciences, Mashhad, Iran. This article was derived from an MD thesis (number 87807), Mashhad University of Medical Sciences, Mashhad, Iran.
Disclosure Statement
No competing financial interests exist.