
Abstract
Abstract
Background:
Women with gestational diabetes mellitus (GDM) and their infants are at increased risk of developing metabolic disease; however, longer breastfeeding is associated with a reduction in these risks. We tested an intervention to increase breastfeeding duration among women with GDM.
Materials and Methods:
We conducted a cluster randomized trial to determine the efficacy of a breastfeeding education and support program for women with GDM. Women were enrolled between 22 and 36 weeks of pregnancy and cluster randomized to an experimental lifestyle intervention or wait-list control group. Breastfeeding duration and intensity were prespecified secondary outcomes of the trial. Duration of exclusive and any breastfeeding was assessed at 6 weeks and at 4, 7, and 10 months postpartum. We quantified differences in breastfeeding rates using Kaplan–Meier estimates, log-rank tests, and Cox regression models.
Results:
We enrolled 100 women, of whom 52% were African American, 31% non-Hispanic white, 11% Hispanic, 9% American Indian or Alaskan Native, 2% Asian, 2% other, and 4% more than one race. In models accounting for within-cluster correlation and adjusted for study site, breastfeeding intention, and African American race, women allocated to the intervention group were less likely to stop breastfeeding (adjusted hazard ratio [HR] 0.40, 95% confidence interval [CI] 0.21–0.74) or to introduce formula (adjusted HR 0.50, 95% CI 0.34–0.72).
Conclusion:
Our results suggest that targeted breastfeeding education for women with GDM is feasible and efficacious. Clinical Trials Registration: http://clinicaltrials.gov/ct2/show/NCT01809431
Introduction
G
Breastfeeding support interventions have been shown to be effective in multiple settings. In primary care, combined prenatal and postnatal support involving a lay-person was especially effective. 11 Among healthy mothers with term infants, 12 stronger effects were found for face-to-face, proactive support from nonprofessionals with four to eight contacts over the course of the intervention.
Women with GDM may require additional support to initiate and sustain breastfeeding. In a Canadian population-based study, women with gestational diabetes were less likely to initiate breastfeeding or to be breastfeeding at hospital discharge than women without diabetes. 13 A U.S. study found similar rates of breastfeeding initiation, but lower continuation, among women with GDM, compared with women without diabetes. 14 These differences may reflect greater difficulty initiating lactation among women with GDM.15,16
Given the potential for breastfeeding to reduce metabolic disease risk for both mother and child, we tested a social cognitive theory-based intervention to increase breastfeeding duration and intensity among women with GDM. We hypothesized that a breastfeeding support intervention integrated within a lifestyle intervention would increase duration of any and exclusive breastfeeding among women with GDM.
Materials and Methods
We conducted a cluster randomized controlled trial of Nutrition, Exercise and coping Skills Training (NEST), a Nutrition, Exercise, and Social cognitive Theory-based group intervention to optimize outcomes among women with GDM. 17 The NEST intervention included prenatal education about breastfeeding, phone support, and 13 weeks of group nutrition and exercise sessions beginning at about 6 weeks postpartum. Women were randomized to the NEST experimental intervention or to a wait-list control group; women in the wait-list group were offered the nutrition, exercise, and coping skills components of the intervention at the end of the 10-month follow-up period. The prespecified primary outcome of the study changed in fasting glucose and maternal weight from enrollment to 10 months postpartum. Results for the primary outcome of the trial are currently under review. In this study, we present data on the prespecified secondary outcomes of duration of any and exclusive breastfeeding.
Trial design
Although randomizing individual women to the experimental group or wait-list control group would be ideal, we anticipated that we would not be able to accrue a sufficient number of women with similar due dates to form concurrent experimental and wait-list control groups. We therefore used a cluster randomization approach, in which groups of women inducted over a 1-month enrollment period from a given site were randomly assigned to either the experimental group or the wait-list control group. There were no changes in eligibility criteria during the course of the study.
Participants
Women were recruited from two clinical sites in Raleigh, North Carolina: Rex Hospital Women's Specialty Services and Wake County Human Services Clinic/WakeMed High Risk Clinic. Rex Hospital Women's Specialty Services serves primarily privately insured women, whereas Wake County Human Services and the WakeMed High Risk Clinic serve primarily publically insured women. Women were eligible if they were diagnosed with GDM with two or more 100-g Oral Glucose Tolerance Test values exceeding established thresholds (fasting 95, 1 h 180 mg/dL, 2 h 155 mg/dL, 3 h 140 mg/dL) 18 and were older than 21 and less than 37 weeks pregnant. Although GDM screening is traditionally performed at 24–28 weeks, we found variation in the timing of screening and presentation to care in our study sites and therefore included as eligible women at a broader range of gestational ages. Additional eligibility criteria included age ≥18 and ≤45, prepregnancy body mass index >25 kg/m2, and ability to read and write in English. We excluded women with overt diabetes, indexed by a baseline A1c ≥6.5 mg/dL.
Experimental intervention
The NEST intervention was developed from two prior trials targeting parents and their school-age children 19 and postpartum women. 20 To tailor the program for women with GDM, we added two sessions addressing (1) the importance of breastfeeding for metabolic control and infant health and (2) progression of GDM to prediabetes and type 2 diabetes mellitus. Details of the NEST intervention have been published elsewhere. 17 Briefly, the intervention began with Phase I, an intensive group intervention, beginning with a prenatal breastfeeding class. Then, starting ∼6 weeks postpartum, women participated in a 13-week intensive lifestyle intervention delivered with weekly classes and a home exercise program. Throughout Phase I, participants received weekly text messages reinforcing intervention themes. During Phase II, participants returned for monthly group sessions for 3 months. The final study contact occurred 3 months after completion of Phase II.
The study interventionist was a college graduate who had undergone training in group-lifestyle interventions and completed an online breastfeeding program. 21 The prenatal class was led by the study's International Board Certified Lactation Consultant (IBCLC).
During pregnancy, intervention group participants attended a specially designed breastfeeding class. Using a white board, the study IBCLC invited women to share benefits of breastfeeding for the mother and infant, using the group's knowledge as a springboard for discussing links between breastfeeding and maternal metabolic control, calories consumed, and weight loss. The class also reviewed the importance of skin-to-skin and early initiation of breastfeeding, feeding based on infant cues, and positioning. Women also received a breastfeeding pillow. Fidelity of the group sessions to protocol was assessed by observation of two randomly selected sessions per month.
Weekly prenatal text messages addressed management of GDM and tips for breastfeeding (see Appendix). Two prenatal messages were breastfeeding specific. The intervention did not include contact during the maternity hospitalization. Following birth, the interventionists contacted women weekly through text messages to inquire how breastfeeding was progressing. Interventionists answered questions using a protocol adapted from an effective prenatal and postnatal breastfeeding intervention. 22
Weekly text messages continued while women were attending the group classes in the 13-week intensive experimental intervention; for women who continued to breastfeed, the weekly study text messages included breastfeeding tips with contacts to text or call for assistance. Messages included anticipatory guidance on engorgement, growth spurts, returning to work, and normal infant sleep patterns, as well as information on the importance of breastfeeding for maternal and child health. If women were encountering difficulties, the study IBCLC called them to provide additional support.
Women allocated to the wait-list control group received usual care for lactation support and GDM during the prenatal and postpartum period. Wake Country WIC offers individualized medical nutrition therapy for women with GDM. WIC breastfeeding peer counselors were also available for home visits or phone support. Women gave birth at either UNC Rex Hospital or WakeMed Raleigh Hospital. Both facilities offer inpatient consultation with International Board Certified Lactation Consultants; however, neither hospital is certified by Baby Friendly Hospital Initiative.
Data collection occurred at the same times as women in the experimental group. At 10 months postpartum, they could receive the 13-week postpartum NEST intervention. The breastfeeding component was not included because the wait-list intervention was delivered at 10 months postpartum, remote from the birth of the infant.
Outcome ascertainment
Women completed study assessments at enrollment at 22–36 weeks of pregnancy (Time [T]1), at 6 weeks postpartum (T2), at the end of the intensive intervention, ∼4 months postpartum (T3), at 7 months postpartum (T4), and at 10 months postpartum (T5). Women who missed a follow-up visit were not excluded from subsequent visits. Duration of any breastfeeding was assessed with the question, “How old was your baby when you completely stopped breastfeeding and pumping milk?” Duration of exclusive breastfeeding was assessed with the question, “How old was your baby when he or she was first fed formula?” Exclusive breastfeeding was defined as never having been fed formula, inclusive of supplementation during the hospital stay.
Additional breastfeeding measures
Breastfeeding intention was assessed at baseline, using the Infant Feeding Intentions (IFI) Scale. 23 This is a five-point Likert scale measure that assesses strength of intention to initiate breastfeeding (“I am planning to only formula feed my baby” [reverse scored] and “I am planning to at least give breastfeeding a try”) and breastfeed exclusively at 1, 3, and 6 months (“When my baby is X months, old, I will be breastfeeding without using any formula or other milk”). Responses range from “Very much agree” to “Very much disagree.” Feeding intention scores range from 0 to 16, with higher scores indicating stronger intention.
We measured breastfeeding intensity using a dietary recall questionnaire adapted from the Infant Feeding Practices Survey II. 24 Breast milk feeding intensity was defined as the proportion of all milk feedings that were breast milk. For analysis, we categorized intensity as less than 20% (low), 20% to 80% (medium), and greater than 80% (high).22,25 We assessed reasons for introducing formula or stopping breastfeeding using a checklist of reasons for weaning adapted from the Infant Feeding Practices Study II. 26
Sample size
We planned for 80 women to complete the study, with 40 per group. In prior studies, we had experienced attrition rates of about 20%; based on this attrition rate, we enrolled 100 women. To collect data for our primary outcomes of fasting glucose and weight change, an in-person visit was required. We therefore excluded from follow-up women who were unable to attend visits due to work or who moved out of the study region. We further excluded women who became pregnant during follow-up, as their pregnancy would affect their fasting glucose and weight. With 80 participants completing the trial and with adjustment for within-cluster correlation, we had 80% power to detect a 0.67 SD difference between wait-list control and experimental groups with an alpha of 0.05. Because the intervention was low risk, an interim analysis was not performed.
Randomization
A computerized randomization program was used to generate the randomization sequence for the groups of women. The approach to randomization was stratified by study sites; within each site, the sequence that was developed had an equal number of allocations to each of the intervention and control groups, in an effort to have balanced allocation within each site. The project manager used the site-stratified randomized sequences to assign inducted groups, recruited in 1-month blocks, to the appropriate arm of the trial. Six inductions occurred in one site and two inductions occurred in the other site.
Blinding
The goal of our study was to determine the efficacy of a breastfeeding support intervention compared with usual care. We therefore did not provide an attention-control intervention, but rather compared the experimental intervention to a wait-list control condition. Participants were not blinded to their allocation. However, research assistants who were blinded to study group assignment collected all outcome data using a standardized manual.
Statistical methods
To compare baseline characteristics, we used chi-square tests, Fisher's exact tests, or t-tests, as appropriate, to determine whether, despite randomization, the experimental and wait-list control groups were unbalanced at baseline. Unbalanced variables (p < 0.10) were considered for use in covariate-adjusted modeling. We did not adjust for intrapartum variables, such as mode of delivery, infant birth weight, or neonatal complications, as these events occurred after randomization.
The key outcomes for this analysis were duration of any breastfeeding and exclusive breastfeeding. We used an intention-to-treat approach to compare breastfeeding durations between women allocated to the experimental versus wait-list control groups who had follow-up data. We used Kaplan–Meier curves to generate time-specific estimates of any and exclusive breastfeeding, and log-rank tests to compare the curves between the randomized groups. We used unadjusted and adjusted Cox proportional hazards models to estimate the risk of breastfeeding cessation among women allocated to the experimental group versus wait-list control through hazard ratios (HR). All Cox proportional hazards models accounted for within-cluster correlations. Adjusted models included one covariate that differed at baseline between the experimental and wait-list control groups, that is, African-American race. We further adjusted for study site (as a stratification factor) and for breastfeeding intention, which is a strong independent predictor of breastfeeding outcome. 23
To determine whether study site or black race modified the effect of the intervention, we formally tested for interaction using a cross-product term; stratified analyses were also performed in exploratory analyses. To test whether there might be differential loss to follow up as a function of breastfeeding intention, we compared baseline IFI for women who were or were not lost to follow-up separately within the experimental and wait-list control groups by two sample t-tests.
In a secondary analysis, we used the Mantel–Haenszel chi-square test to compare breastfeeding intensity category (high, medium, or low) between randomized groups at the 6-week visit. In an exploratory analysis, we used Fisher's exact tests to measure whether the proportions of women reporting each issue as an important reason for introducing formula or weaning differed significantly between the randomized groups.
Analyses were performed using SAS 9.3 and 9.4 (Cary, NC). The study was approved by the Institutional Review Boards of The University of North Carolina at Chapel Hill, REX Healthcare, WakeMed Hospital, and Wake County Human Services. All participants provided informed consent.
Results
Recruitment
We screened 215 women for the study, of whom 100 were found eligible and subsequently enrolled (Fig. 1). We encountered significant difficulties retaining women in our study; while 85% provided follow-up data at some point, only 51% of participants completed the 10-month follow-up. Women cited multiple reasons for not attending a data collection: life had become overwhelming with the new baby; they moved from the Raleigh, North Carolina area and did not have reliable transportation; they became pregnant again; and they had to go back to work at 6 weeks postpartum. One infant in the experimental group died soon after birth due to a congenital cardiac anomaly.
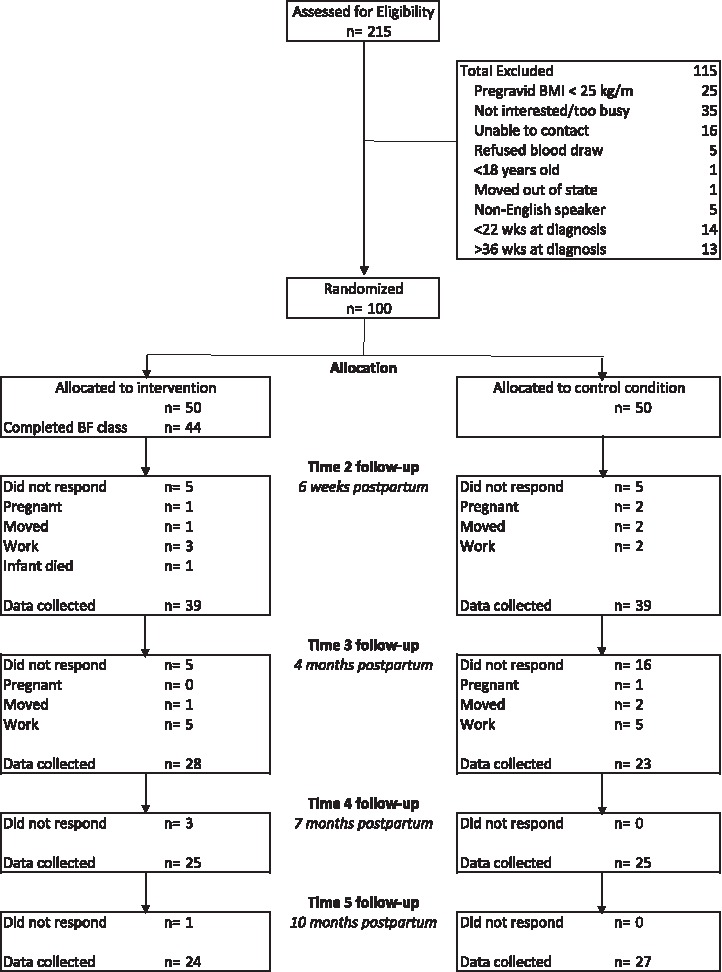
CONSORT flow diagram. BMI, body mass index.
Enrolled study population
Recruitment began on June 29, 2012 and ended on September 11, 2014, once the 100th participant was enrolled. Our study population was diverse (Table 1): 52% were African American, 31% non-Hispanic white, 11% Hispanic, 9% American Indian or Alaskan Native, 2% Asian, 2% other, and 4% more than one race. About 1 in 5 reported a household income <$20,000 per year, and 48% had a high school education or less. IFI scores (0–16 point scale) were similar in the experimental and wait-list control groups (mean ± SD 11.4 ± 4.2 versus 11.3 ± 4.8, p = 0.98). We similarly did not find statistically significant differences in OGTT values between the intervention and control groups (mean ± SD: Fasting 95.2 ± 12.3 versus 100.0 ± 12.0, p = 0.07; 1 h 196.8 ± 24.1 versus 194.1 ± 30.2, p = 0.62; 2 h 171.1 ± 23.6 versus 176.0 ± 29.5, p = 0.40; 3 h 125.7 ± 29.2 versus 138.2 ± 36.2, p = 0.08). Median gestational age at recruitment was 31.6 weeks (interquartile rage 28.3–33.0).
GED, General Education Diploma.
Breastfeeding intervention delivery
In the experimental group, 44 of 50 women attended the prenatal breastfeeding group class. Fidelity to the protocol was >85%. Postpartum, nine women in the experimental group requested to be contacted by the study lactation consultant for additional support.
Breastfeeding outcomes
We analyzed duration of any and exclusive breastfeeding among the 85 women who provided data on infant feeding during postpartum follow-up. Women were censored for the Kaplan–Meier analyses and Cox modeling for the appropriate endpoint if they were lost to follow-up before they reported discontinuing any or exclusive breastfeeding, or if they were still breastfeeding at the time of completing the study. In our intent-to-treat analysis, we found that women in the experimental group were more likely to be breastfeeding (log rank p < 0.01, Fig. 2a) and to be breastfeeding exclusively (Fig. 2b, log rank p = 0.06) throughout the follow-up period. At 4 weeks postpartum, we found higher rates of any and exclusive breastfeeding in the experimental group, compared with the control group (Any: 87%. SE 5.4% versus 64%, SE 7.7%; exclusive: 45% [SE 7.9%] in the experimental group and 23% [SE 6.4%] in the control group).
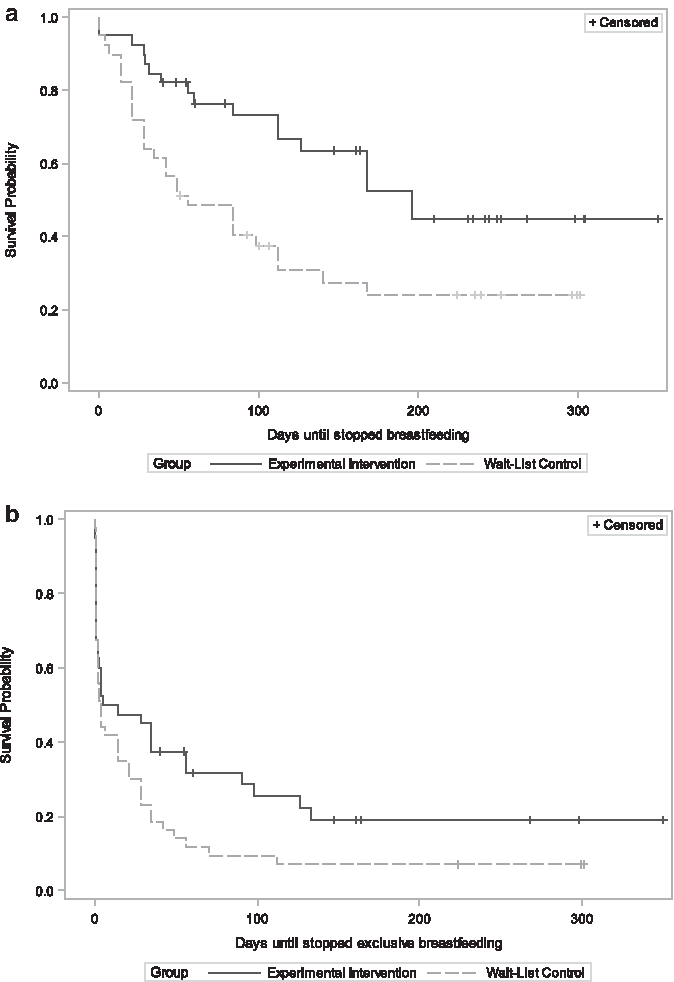
In proportional hazards modeling, women in the experimental group were less likely to discontinue breastfeeding (unadjusted HR 0.44, 95% confidence interval [CI] 0.21–0.95). This association was strengthened with adjustment for prenatal IFI; we further adjusted for study site and black race, yielding an adjusted HR of 0.40 (95% CI 0.21–0.74). We similarly found that women in the experimental group were less likely to introduce formula (unadjusted HR 0.64, 95% CI 0.41–1.02). This association was strengthened with adjustment for prenatal IFI, as well as study site and black race (adjusted HR 0.50, 95% CI 0.34–0.72).
We further tested whether study site or race modified the effect of the intervention on time to weaning. We found similar effects of the intervention on time to weaning at the two study sites (Site 1: HR 0.49, 95% CI 0.26–0.92; Site 2: HR 0.38, 95% CI 0.31–0.47, p for interaction = 0.28). We found a stronger effect size for time to weaning among black women (HR 0.40, 95% CI 0.20–0.78) than among nonblack women (HR 0.63, 95% CI 0.23–1.68), but this difference was not statistically significant (p for interaction = 0.37).
To test the extent to which loss to follow-up might have biased our results, we compared IFI scores among women who were versus were not lost to follow-up. In the experimental group, we found similar IFI scores (mean ± SD, IFI score, 0–16 point scale) for lost to follow-up (N = 9, versus 11.2 ± 4.1 for not lost, N = 41, t-test p = 0.42). For women allocated to the control group, the six women lost to follow-up had lower IFI scores than those not lost to follow-up (5.3 ± 4.8 versus 12.2 ± 4.2, t-test p < 0.001).
At the 6-week visit, 62% of women in the experimental group reported high-intensity breastfeeding, defined as >80% of feedings as breast milk, compared with 36% of wait-list control group women (Fig. 3, MH chi-square p = 0.02). Women in the wait-list control group were more likely to report introducing formula or weaning because their breasts were overfull or engorged (10/33 [30%] versus 2/26 [8%] in the experimental group, Fisher's exact p < 0.05) or because they wanted to go on a weight-loss diet (5/33, 15% versus 0/26, 0%, Fisher's exact p = 0.06). No harms were reported in either group.
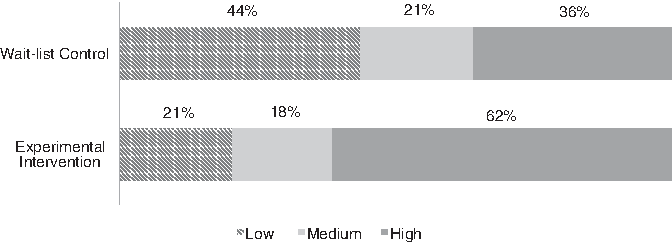
Breastfeeding Intensity at 6 weeks. Breastfeeding intensity is defined as the proportion of infant feedings that are breast milk. Intensity is classified as low (<20%), medium (20–80%), or high (>80%).
Discussion
We found that a targeted prenatal breastfeeding class delivered by an IBCLC, coupled with text messages, phone outreach from a lay interventionist, and lactation consultant support as needed, increased breastfeeding duration and intensity in a diverse population of low-income women with GDM. Our experimental intervention included face-to-face contact, proactive text messages, and phone calls, consistent with practices found effective in intervention studies among healthy mothers and infants. 12 Our results suggest that targeted breastfeeding support for women with GDM is feasible and efficacious.
Our work confirms and extends earlier intervention studies among women with GDM. Ferrara et al. 27 incorporated breastfeeding support in the Diet, Exercise and Breastfeeding Intervention (DEBI) study. Pregnant women randomized to the intervention were referred to a lactation consultant who discussed the benefits of breastfeeding and encouraged exclusive breastfeeding for 6 months. Women were offered a breast pump, and one to four follow-up calls were scheduled in the first 6 weeks postpartum. The authors found no differences at 6 weeks (intervention 87.8%; control 90.8%, p = 0.50) and a modest difference in breastfeeding continuation at 7 months (intervention: 62.7%; control 47.7%, p = 0.09). Among DEBI study participants, 85% were married, and more than half were college graduates. The Balance After Baby Web-based GDM intervention enrolled 75 women at 6 weeks postpartum. Breastfeeding mothers were encouraged to continue, and they had access to 4 online modules related to breastfeeding, as well as a mechanism to contact a lactation consultant. Of 36 women randomized to the intervention, 4 contacted the study lactation consultant. Breastfeeding outcomes were not reported. This patient population was also highly educated: 57% were college graduates and 24% had some college education. Our study provided targeted breastfeeding support to low-income women with GDM, and we found differences in breastfeeding duration between experimental and control groups.
Several factors may explain why our intervention produced greater differences in breastfeeding rates than the DEBI study. We used a face-to-face prenatal group session that engaged women and invited them to share their knowledge about breastfeeding and health outcomes. The small-group setting allowed women to discuss common barriers to breastfeeding and share their own experiences with one another. We also provided proactive support through text messages. It is also possible that the very high breastfeeding rates in the DEBI cohort—nearly 90% at 6 weeks postpartum—created a ceiling effect. This rate is considerably higher than the U.S. National Breastfeeding Rate for children born in 2012. 28
Our study population had similar overall breastfeeding rates, but lower exclusive rates, than reported in national data. In exploratory analyses, we found that control group women who introduced formula were more likely to do so because of engorgement or intention to go on a weight loss diet. Although these differences could reflect multiple testing, it is plausible that intervention guidance about managing engorgement and the role of breastfeeding in weight loss enabled women to overcome these issues.
Our findings must be interpreted in the context of limitations of the study design. This was a cluster randomized controlled trial conducted among low-income, diverse women. In a cluster randomized design, randomization may not balance the groups as efficiently as individual randomization. We experienced much higher loss to follow-up than we had anticipated; however, our time-to-event approach allowed us to incorporate women who had data for at least one follow-up visit. Our low follow-up rates diminished our ability to measure the extent to which our intervention increased achievement of Healthy People 2020 targets, including 3-month exclusive breastfeeding rates and 6-month any breastfeeding rates.
Our low follow-up rates might also bias our results. However, we found that women with lower breastfeeding intention were more likely to drop out of the wait-list control group, but not the experimental group, which would be expected to bias our results toward the null by potentially raising rates of breastfeeding in the control group. Breastfeeding outcomes were self-reported, and it is possible that social desirability bias may have affected responses. However, the research assistants completing follow-up interviews were not involved in delivering the intervention and were blinded to treatment group allocation.
We assessed exclusive breastfeeding duration by asking when the infant was first fed formula; however, we did not assess timing of introduction of solid foods. We also did not quantify use of other breastfeeding services among study participants. We enrolled women across a wide range of gestational ages, potentially reducing exposure to the prenatal intervention. However, this approach may increase the generalizability of our findings, in that women with GDM may present late for care. Furthermore, diminished exposure to the intervention would be expected to bias our results toward the null. Finally, because our breastfeeding support intervention was embedded in a lifestyle intervention that included one prenatal class and 13 weekly classes beginning at about 6 weeks postpartum, we cannot determine whether the breastfeeding components alone would have a similar impact on infant feeding outcomes. However, we found substantial differences at 6 weeks postpartum, before the weekly group sessions, suggesting that the combination of the prenatal class, text messages, and access to an IBCLC can impact breastfeeding outcomes.
Our results suggest that a single-group prenatal encounter with a lactation consultant coupled with automated text messages may improve breastfeeding duration and intensity among women with GDM. Future studies are needed to test both the efficacy and effectiveness of our intervention in diverse settings and evaluate feasibility of its implementation within routine prenatal care.
Conclusion
Our results have important implications for the care of women with gestational diabetes. GDM management currently focuses on glycemic control during pregnancy to prevent macrosomia and neonatal hypoglycemia for the newborn, as well as postpartum screening to determine maternal risk for type 2 diabetes. 1 We tested a social cognitive theory-based breastfeeding intervention among women with GDM, and we found that our intervention increased breastfeeding duration and intensity. These results suggest that such breastfeeding support could be integrated into GDM management. If our findings are replicated, our intervention may improve health outcomes across two generations.
Footnotes
Acknowledgments
The authors wish to thank the mothers and infants who participated in the study. In addition, we wish to acknowledge our study coordinator, Madeline Neal, interventionist, Gail Hall, and lactation consultant, Hannah Edens. Ms. Neal and Ms. Hall were employed by the UNC School of Nursing during the study period. Ms. Edens continues to be employed by UNC Hospitals. All three individuals were supported by 1R21DK092750-01A1 during the study period. Findings were presented at the Society for Maternal Fetal Medicine, abstract number 97, on February 6, 2016. The trial is funded by the National Institutes of Health: The National Institute of Diabetes and Digestive and Kidney Disease, 1R21DK092750-01A1. Breastfeeding pillows were donated by The Boppy Company. Neither the National Institutes of Health nor The Boppy Company had any role in the design of the study, analysis of results, or preparation of the article.
Disclosure Statement
No competing financial interests exist.
Appendix
Breastfeeding text messages delivered as part of the Nutrition, Exercise and coping Skills Training (NEST) intervention
Study participants randomized to the intervention received up to 16 prenatal text messages regarding gestational diabetes and breastfeeding, as well as weekly text messages from birth through the end of the Phase I intensive intervention.
Listed here are the breastfeeding-related text messages provided as part of the study.