
Abstract
Abstract
Background:
Breastfeeding is associated with decreased risk of childhood obesity. However, there is a strong correlation between maternal weight status and childhood obesity, and it is unclear whether or not breastfeeding among overweight mothers could mitigate this risk. Our goal was to examine whether or not exclusive breastfeeding (compared to formula feeding) among overweight and obese mothers is associated with lower weight-for-length (W/L) percentile at 1 year.
Materials and Methods:
Data from the Infant Feeding Practices II study were used. Infants who were preterm or underweight at 1 year, and mothers who were underweight before pregnancy, were excluded from analysis. There was a significant interaction between exclusive breastfeeding for 4 months and maternal prepregnancy weight status (normal weight, overweight, obese) on infant W/L percentile at 1 year. Stratified linear mixed-effects growth modeling controlling for covariates was created to test the relationship between exclusive breastfeeding and infant W/L percentile within each maternal weight category.
Results:
A total of 915 subjects met inclusion criteria. Normal weight and obese mothers who exclusively breastfed for 4 months had infants with a smaller rate of increase in W/L percentile during the first year compared with those who used formula. Infants of overweight and obese mothers who exclusively breastfed for 4 months had lower W/L percentile at 1 year than those who used formula.
Conclusions:
Exclusive breastfeeding for 4 months among normal weight and obese mothers resulted in less increase in W/L percentiles in the first year. Obese mothers often have a difficult time initiating and maintaining breastfeeding. Concerted efforts are needed to support this population with breastfeeding.
Introduction
T
The act of breastfeeding may also play a role in the learned self-regulation of energy intake. Breastfed infants are thought to exert more control or self-regulation over the amount of milk consumed, translating into increased self-regulation of caloric intake in later infancy and childhood.11,12 Breastfeeding has also been associated with greater satiety responsiveness 13 and decreased picky eating behaviors 14 among preschool age children, as well as decreased abnormal eating attitudes and behaviors, specifically weight preoccupation and dieting, among 11-year-old boys and girls. 15
One of the strongest predictors of childhood obesity is parental weight status.16,17 Maternal obesity during pregnancy is associated with higher birth weight and risk for being large for gestational age at birth, 18 both of which predict later overweight status in childhood.19,20 Unfortunately, overweight and obese mothers are less likely to breastfeed and typically breastfeed for a shorter duration,21,22 thus decreasing the potential protective effect of breastfeeding on child weight status. However, given the strong correlation between maternal weight status and childhood obesity, it is unclear whether or not breastfeeding could mitigate this risk, particularly among obese mothers.
In a controlled laboratory experiment with rats, milk from different maternal sources appeared to modify the progeny's genetically determined risk of developing obesity and insulin resistance. 23 Young rats genetically determined to have diet-induced obesity (DIO) had improved insulin sensitivity and lower fat mass when they were suckled by a diet-resistant (DR) biologically unrelated dam, or mother. In contrast, DR offspring gained more weight, had increased fat mass, and developed higher levels of insulin resistance when fostered by DIO dams. These results suggest that milk from normal weight dams may be able to decrease the genetic risk of obesity passed on by the biologic overweight dam, while milk from a DIO dam increases one's risk.
In human studies, the evidence is mixed. One study conducted on a German cohort found that overweight mothers who exclusively breastfed for ≥17 weeks had boys with lower percent body fat at 7 years compared with boys who were not exclusively breastfed for that long or only had formula. 24 This differential effect was not seen in girls or boys of normal weight mothers. In another study conducted on a US cohort, there was no effect of exclusive breastfeeding for 6 months among overweight mothers on child weight status at age 9–14 years. 25
Given the results of these studies, our goal was to further examine the interaction effect of exclusive breastfeeding and maternal prepregnancy weight status on infant weight-for-length (W/L) percentile at 1 year. We were particularly interested in examining the effect of breastfeeding among overweight and obese mothers. Using data from the Infant Feeding Practices Study II (IFPS II), we examined whether there was a protective effect of exclusive breastfeeding for 4 months, compared to formula use, on infant growth parameters among normal weight, overweight, and obese mothers. Given the result of the animal study, we hypothesized that exclusive breastfeeding for 4 months would have a protective effect on infant W/L percentile at 1 year among normal weight mothers, but not for infants of overweight and obese mothers.
Materials and Methods
Data were obtained from the IFPS II, a longitudinal study conducted by the US Food and Drug Administration in collaboration with the Centers for Disease Control and Prevention (CDC) between 2005 and 2007. Study coordinators mailed questionnaires to mothers selected from a national consumer opinion panel. Criteria for participation included the following: mothers' age ≥18 years, singleton birth, infant gestational age ≥35 weeks, infant birth weight ≥5 pounds, infant not requiring intensive care level of service for >3 days, and the infant not having an illness or condition likely to affect feeding (at birth or potentially during the first year of life).
Questionnaires were administered to the mothers at 7 months of gestation, birth, the neonatal time point (∼3 weeks old), and postnatal months 2, 3, 4, 5, 6, 7, 9, 10, and 12. Questionnaires collected information about maternal health and infant feeding, health, in home care, and medical care. Details regarding the study have been previously described. 26 Of the 1,807 women who completed the 12-month postnatal survey, 1,162 provided the infant's weight, length and date of primary care provider visit in order for us to calculate age- and gender-appropriate W/L percentile at 12 months. Only children with a primary care visit ±30 days of the child's birthday were included for the 12-month time point. Mean age at the time of the 12-month visit was 369.6 (standard deviation [SD] 6.6) days. Additional surveys were excluded if mothers were underweight (body mass index [BMI] <18.5), the infant was preterm (gestational age <37 weeks), or the infant's W/L z-score at 1 year was less than −5.0 or >5.0, resulting in a final sample size of 915. This study was exempted from review by the Institutional Review Board of University of California, San Diego.
Measures
Mothers were asked to record their child's weight (pounds) and length (inches) as documented by the hospital or their primary care provider at birth and the 2-, 4-, 6-, and 12-month well-child visit. Age was determined by calculating the difference between the infant's birth date and the reported date of the primary care provider visit. Weights and lengths obtained more than 30 days before or after the 2-, 4-, 6-, and 12-month time point were not included. Average age at these visits (aside from birth) were 68.8 (SD 14.7), 126.4 (SD 16.4), 192.0 (SD 19.8), and 369.6 (SD 6.6) days, respectively. Infant W/L percentile was then calculated based on the World Health Organization Growth Charts.27,28 Greater infant W/L percentile has been shown to be associated with childhood obesity.29,30 W/L z-scores >5.0 and less than −5.0 were considered biologically implausible and excluded from the data set.
Our primary independent variables were as follows: (1) exclusive breastfeeding for 4 months and (2) maternal prepregnancy weight status. For breastfeeding status, we created a composite variable accounting for both duration and exclusivity of breastfeeding for 4 months. Although the AAP recommends exclusive breastfeeding for about 6 months, 1 the majority of mothers do not adhere to this recommendation, and formula or baby food is often introduced before this time point.31,32 In the CDC National Immunization Survey, only 18.8% of infants born in 2011 were reported to be exclusively breastfeeding for 6 months compared to 32.9% who were exclusively breastfeeding for 4 months. 33 In the original IFPS II sample, 28% of mothers exclusively breastfed for 4 months, 14% for 5 months, and 4% for 6 months. As such, we were unable to examine exclusive breastfeeding for 6 months due to a limited sample size. Therefore, we chose the 4-month time point. In each of the postnatal questionnaires, mothers were asked how often their baby was fed a variety of foods in the past 7 days. Exclusivity was defined when mothers reported only giving the infant breast milk and no other food, including formula, cow's milk, juice, cereal, or baby food. By assessing mothers' responses from the neonatal to month 4 surveys, we created a composite variable that reflected whether or not infants were exclusively breastfed for 4 months. Infants who received formula in the hospital at the time of birth were not excluded from this category since there are many factors that may have influenced whether or not an infant received formula in the hospital despite the intent of the mother to exclusively breastfeed. Mean age of infants at the 4-month survey was 17.52 ± 1.33 weeks.
Self-reported maternal prepregnancy weight and height collected during the third trimester of pregnancy were used to calculate maternal prepregnancy BMI. While this study did not directly assess maternal anthropometric measures, numerous studies have demonstrated the validity of self-reported anthropometric measurements in adults with no statistical difference between self-reported values and those obtained from clinical records.34,35 BMI was calculated using the formula BMI = (pounds/[inches] 2 ) × 703. Prepregnancy BMI was then classified as normal weight (BMI 18.5–24.9), overweight (BMI 25–29.9), or obese (BMI ≥30). 36
Covariates
We adjusted for several sociodemographic variables in the model, including maternal age, race, marital status, annual household income, and education. Race was dichotomized as white versus non-white since the majority of the overall sample was white (88%). Marital status was dichotomized as those who were married versus those who were single, never married, divorced, separated, or widowed. The median income within our sample was $40,000. Therefore, household income was dichotomized into those who earned <$40,000/year and those who earned ≥$40,000/year. Maternal education was also dichotomized at the median (some college or below [<16 years] versus college graduate and beyond [≥16 years]). In addition, several variables were selected a priori to be included in the model due to previous evidence suggesting their association with obesity. These included maternal smoking status, 37 gestational diabetes,38–40 and gestational weight gain.41,42 Mothers were classified as smokers if they reported active smoking during the third trimester of pregnancy. Mothers were categorized as having diabetes if they reported having gestational diabetes, juvenile-onset diabetes, or adult-onset diabetes during their pregnancy. Amount of gestational weight gain was reported in the neonatal questionnaire and used as a continuous variable. Infant sex was also included as a covariate.
Statistical analysis
SAS 9.4 (Cary, NC) was used to conduct all analyses. Means and frequencies were used to describe the sample. Bivariate analyses were conducted using chi-square tests or generalized linear models (GLM) to determine whether infant W/L percentile, breastfeeding status, and covariates differed between maternal prepregnancy weight groups. Using PROC MIXED in SAS and testing for fixed and random effects, we conducted linear growth modeling (which accounts for baseline and all subsequent W/L percentiles) controlling for a priori covariates.
First, we estimated the unconditional model with no predictors to examine the beneficial effect of including random slopes. Tests of nested models suggested that adding a random effect for linear slope improved model fit (−2 log likelihood decreased from 37,893 to 37,570). Then, we added a level-1 linear effect of time in months to model individual level growth over time. The linear and quadratic effect of time was tested and the fit statistics improved with the introduction of a quadratic effect of time (−2 log likelihood decreased from 37,366 to 37,288). However, the main effect of time 2 was not significant (p = 0.71) and the simple linear model was used.
In the linear model, we tested the effect of time, exclusive breastfeeding for 4 months, maternal prepregnancy weight status, the three-way interaction between time × exclusive breastfeeding × maternal prepregnancy weight status, and the respective two-way interactions. There was a significant interaction between time × exclusive breastfeeding for 4 months (F[1, 948] = 17.30, p < 0.001) and exclusive breastfeeding for 4 months × maternal prepregnancy weight status (F [2, 1,045] = 3.16, p = 0.04). Therefore, stratified analyses were conducted for each maternal prepregnancy weight status group (i.e., normal weight, overweight, and obese) to examine the effect of exclusive breastfeeding within each group compared to formula feeding. A dummy coded index for exclusive breastfeeding status for 4 months was entered, and a two-way interaction between time × exclusive breastfeeding for 4 months was examined to determine whether there was an effect on change in W/L percentile over time. All these models controlled for known covariates for infant weight status, maternal breastfeeding, and maternal weight status, including maternal age, gestational weight gain, race, marital status, income, education, smoking, diabetes, and infant sex. Statistical significance was set at p ≤ 0.05 for these analyses.
Results
Almost half the sample of mothers (n = 915) was normal weight (47.8%), 28.0% were overweight, and 24.3% were obese (Table 1). Mothers were more likely to exclusively breastfeed for 4 months if they were normal weight. Normal weight mothers were also more likely to have a median income ≥$40,000 and a college degree or higher. Obese mothers were more likely to have diabetes. Infant W/L percentile at birth did not differ significantly between maternal prepregnancy weight groups.
Maternal prepregnancy weight status was classified by the following definitions: normal weight = 18.5–24.99, overweight = 25–29.99, obese ≥30 (mean = 36.03, SD = 5.40).
Maternal diabetes was defined as self-report of gestational diabetes, juvenile-onset diabetes, or adult-onset diabetes during or before pregnancy.
BMI, body mass index; SD, standard deviation.
There was a significant interaction in the overall model between maternal prepregnancy weight status and exclusive breastfeeding for 4 months (p = 0.04). Therefore, separate linear growth models were conducted for each maternal weight group. Among normal weight mothers, the mean W/L percentile at birth was 50.30% (standard error [SE] 9.10), and the between-child variation in growth explained 24.7% of the variability in growth. There was a significant interaction between time × exclusive breastfeeding such that those who did not exclusively breastfeed for 4 months had a 1.06% (SE 0.39) greater rate of increase in W/L percentile over time (p < 0.01; Table 2). By 12 months, infants who received formula in the first 4 months had a mean W/L percentile that was 3.92% higher than those who were exclusively breastfed for 4 months (p = 0.29; Fig. 1a).
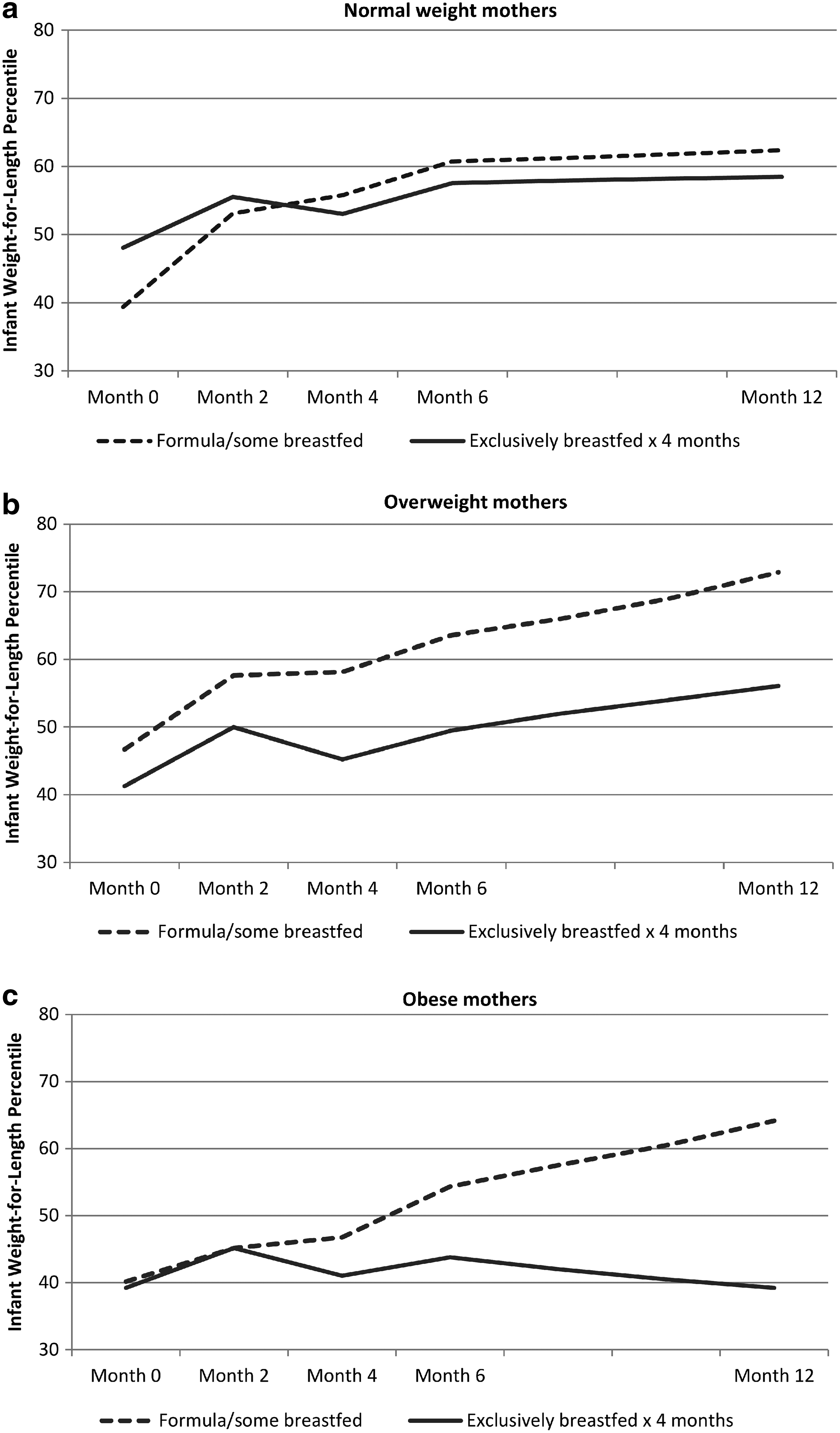
Growth model examining the effect of exclusive breastfeeding for 4 months on infant W/L percentile over the first 12 months of life, stratified by maternal prepregnancy weight status. Figures display growth trajectories of infants over the first 12 months of life.
The models included a random statement for the individual allowing variation in intercept, time, breastfeeding status, and time × breastfeeding status with a variance component (VC) covariance structure between the effects. Each result represents the difference in mean W/L percentile for that variable compared to when the predictor equaled 0. All models included covariates for maternal age, race, education, smoking status during pregnancy, marital status, income, diabetes, and infant sex.
SE, standard error; W/L, weight-for-length.
Among overweight mothers, the mean W/L percentile at birth was 42.75% (SE 11.92), and 24.5% of the variability in growth was explained by differences between children. The interaction between time and exclusive breastfeeding for 4 months approached significance (p = 0.08; Table 2). In the simple linear model (without the interaction term), there was a significant effect of time (1.85%, SE 0.25, p < 0.001) and exclusive breastfeeding for 4 months (9.48%, SE 3.24, p < 0.01) on infant W/L percentile. Exclusive breast feeders had a 16.81% lower W/L percentile at 12 months compared with those who received some formula (p < 0.01; Fig. 1b).
Among obese mothers, the mean W/L percentile at birth was 47.78% (SE 12.64), and 25.5% of the variability in growth was explained by differences between children. There was again a significant interaction between time × exclusive breastfeeding, suggesting that those who did not exclusively breastfeed for 4 months had a 1.98% (SE 0.66) greater rate of increase in W/L percentile over time (p < 0.01; Table 2). The W/L percentile was relatively stable among exclusive breast feeders during that first year, while those who had some formula during the first 4 months had a 24.21% higher W/L percentile at 12 months (p < 0.001) compared with those who were exclusively breastfed for 4 months (Fig. 1c).
In post-hoc analyses, separate linear growth models were also conducted for those who were exclusively breastfed for 4 months and those who were not exclusively breastfed for 4 months to examine whether maternal prepregnancy weight status had an impact on infant growth parameters. Among mothers who exclusively breastfed for 4 months, there was no significant interaction between time × maternal prepregnancy weight status (F[2] = 1.09, p = 0.34), that is, changes in infant W/L percentile did not differ significantly depending on the mother's weight status among those who were exclusively breastfed for 4 months. Similarly, there was no significant interaction between time × maternal prepregnancy weight status among those who were not exclusively breastfed for 4 months (F[2] = 0.24, p = 0.78).
Discussion
In this study, controlling for a priori covariates, normal weight mothers and obese mothers who exclusively breastfed for 4 months had infants with lower increases in W/L percentile over the first year compared with those who used formula. Exclusive breastfeeding was also associated with lower W/L percentiles at 12 months among infants of overweight and obese mothers. Our results support the findings of Li et al. 43 who found that among children of overweight and obese mothers, those who breastfed had lower odds of obesity (OR = 2.8 and 3.5, for overweight and obese mothers, respectively) compared with those who never breast fed (OR = 3.8 and 6.1, respectively). While their study suggests that breastfeeding is associated with lower odds of obesity, they did not examine the growth trajectories of these children over time.
Buyken et al. conducted similar linear mixed-effects modeling and found that breastfeeding countered the effect of maternal overweight on the percent body fat trajectories of boys through the age of 7 years, although the effects of breastfeeding were not clearly seen until children were 3–4 years of age. 24 However, the effect on boys' BMI trajectories only approached significance, and no effects were seen among girls. The results of our study complement that of Buyken et al. by demonstrating that the effect of breastfeeding, particularly exclusive breastfeeding, can be seen as early as 1 year of life among infants of obese and overweight mothers.
However, these findings are in contrast with previous animal studies in which DR progeny pups had increased odds of becoming obese when suckled by an obesity-prone (DIO) dam. 23 Changes in obesity risk in this study may have been induced by the content of the milk. Franco et al. 44 found that consumption of a high-fat diet among pregnant dams resulted in increased maternal body fat and a higher triglyceride, protein, and cholesterol content in the milk during lactation. This difference in milk content exposed pups to overnutrition in the immediate postnatal period and manifested as increased body weight and adiposity in the pup at the time of weaning. Other animal models have also suggested that immediate postnatal overfeeding can result in changes in the epigenome and hypothalamo–pituitary–adrenal axis, which then predisposes the offspring to obesity and other metabolic diseases later in life.45–47
In humans, we know that the composition of breast milk is inherently different than formula, containing a lower protein content, different fatty acid ratios, and more bioactive factors such as leptin and ghrelin, which have been associated with lower infant weight gain and decreased adipocyte growth.8,10,48 However, few studies have examined differences in breast milk composition between normal weight and overweight/obese mothers,49–51 and whether there are other active metabolites that provide a protective effect independent of the mother's weight status or dietary intake.
Outside of metabolic effects, behavioral factors such as the ability to self-regulate energy intake8,11,52 may be contributing to this difference in growth. Infants who breastfeed have demonstrated greater self-regulation while feeding, response to internal cues of satiety and hunger, and ability to adjust their caloric consumption based on the energy density of the food provided.13,53–55 In contrast, infants who were bottle fed during the first 6 months of life were twice as likely to empty a cup of milk on their own in late infancy (7–12 months of life) 11 and eat all the food on their plate in childhood (6 years old). 56 Behaviorally, feeding with a bottle allows mothers to visually assess the amount of milk the infant has consumed and use stimulatory techniques to encourage the infant to resume feeds when paused. As a result, these mothers can control the duration and amount of feedings based on their views of when the infant is hungry and how much he/she should eat. Over the long run, this behavior appears to override the infant's own cues of satiety, which may result in dysregulated eating behaviors. 52 Breastfeeding may therefore allow mothers to develop less controlling feeding patterns and allow the child to self-regulate his/her caloric intake, resulting in more favorable weight status outcomes.
Despite the benefits of breastfeeding, overweight and obese women have lower rates of breastfeeding initiation.57,58 Those who do initiate breastfeeding also tend to do so for a shorter period of time compared with normal weight women.58,59 This trend is likely due to several factors. First, overweight/obese mothers may have a harder time obtaining proper or optimal positioning for latching making it physically difficult for the infant to feed.60,61 Second, they may have a decreased prolactin response to suckling, which is critical in early lactogenesis. 62 Finally, overweight/obese mothers have reported discomfort with exposing body parts in public and difficulty staying modest.62–65 Several programs have tried to increase breastfeeding rates in this population. However, specialized breastfeeding peer counseling targeted toward obese women failed to significantly alter the rate of exclusive breastfeeding for the first 6 months of life, 66 and telephone support from lactation consultants has had mixed results.67,68 Given the benefits of breastfeeding on early infant growth, additional efforts should be made to support breastfeeding initiation and maintenance in this population.
This study is one of a few studies that stratified the effect of breastfeeding on child growth parameters by maternal prepregnancy weight status. Using a fairly detailed report of infant dietary intake, we were also able to determine with some accuracy whether or not infants were being exclusively breastfed for 4 months. Nevertheless, there were several limitations. First, the IFPS II sample was not nationally representative and was overrepresented by whites, women of higher socioeconomic status, English speakers, and those with a stable mailing address. Whether or not this relationship holds true in other racial/ethnic populations is yet to be explored. While this study used a fairly detailed report of infant dietary intake, assessing breastfeeding exclusivity only in the past 7 days may have resulted in an overrepresentation of the proportion of infants who were exclusively breastfed for 4 months. Nevertheless, we were still able to detect an effect of this amount of exclusive breastfeeding on growth parameters in the first year. Third, while the women were asked to provide data almost monthly, the data were obtained via questionnaires and were potentially affected by self-reporting and recall bias. However, the use of self-reported anthropometric measurements in adults has been previously shown to not be statistically different from those obtained from clinical records.34,35 Finally, our exclusive breastfeeding categorization did not distinguish whether or not the breast milk was pumped and fed or provided directly from the breast. Therefore, it is difficult to hypothesize whether or not self-regulation played a role in the outcome. Future analyses should take into consideration the method of delivery of human breast milk and its composition among overweight and normal weight women to shed additional light on mechanisms of action.
Conclusion
The findings of this study suggest that exclusive breastfeeding for 4 months is protective against increased rate of change in W/L percentile during the first year in children of normal weight and obese women, and higher W/L percentile at 1 year in children of overweight and obese women. Because overweight and obese women have lower rates of breastfeeding initiation and higher risk of having overweight or obese children, this group would benefit from targeted interventions to promote breastfeeding and potentially decrease the risk of childhood obesity.
Footnotes
Disclosure Statement
No competing financial interests exist.