
Abstract
Abstract
Background:
Breastfeeding provides maternal and infant health benefits. Maternity care practices encompassed in the 10 Steps to Successful Breastfeeding are positively associated with improved breastfeeding outcomes. This study assessed changes in maternity care practices and lactation support.
Materials and Methods:
In 2009, 2011, and 2014, New York (NY) hospitals providing maternity care services were surveyed to assess the implementation of 9 of the 10 Steps to Successful Breastfeeding, professional lactation support, distribution of formula and discharge packs, and patient and hospital barriers to breastfeeding success. Generalized estimating equations were used to evaluate changes over time.
Results:
Surveys were completed by 138/138 (2009), 128/129 (2011), and 125/125 (2014) NY hospitals. During this time period, the percent of hospitals reporting implementation of Steps 2, 4, 6, or 9 increased, and the mean number of 9 steps implemented increased from 4.3 to 5.3. Hospitals distributing formula samples at discharge to breastfeeding mothers decreased significantly from 39 (32%) to 3 (2%). Professional lactation staffing ratios (N/1,000 births) of both International Board Certified Lactation Consultants and Certified Lactation Counselors increased between 2009 and 2011, but then decreased between 2011 and 2014. Reported barriers to breastfeeding support changed, with reductions in mixed messages from staff, but increases in lack of financial resources for breastfeeding support, inadequate prenatal education, mothers not being prepared, and family not being receptive to breastfeeding.
Conclusions:
Between 2009 and 2014, NY hospitals reported increased barriers and a reduction in professional lactation support, which may have contributed to the limited improvements in breastfeeding support.
Introduction
I
Comprehensive, structured breastfeeding education and lactation counseling during pregnancy and continuing through the postpartum period is also associated with increased breastfeeding initiation, exclusivity, and duration.12–15
Lack of prenatal education and family support for choosing breastfeeding are barriers that can adversely affect breastfeeding success.16,17 To support mothers with complex breastfeeding problems and lactation management, the Centers for Disease Control and Prevention (CDC) recommends that an International Board Certified Lactation Consultant (IBCLC) be included on the health care team. 18 Increased professional lactation support, especially when provided by an IBCLC, is associated with increased breastfeeding success.19,20
In New York (NY), concerted efforts to improve hospital implementation of recommended maternity care practices (10 Steps) have included development of the Model Hospital Breastfeeding Policy 21 and Implementation Guide, 22 staff training opportunities, quality improvement work, and legislative and regulatory changes.23,24 This work led to significant improvement in written hospital breastfeeding policies and breastfeeding rates in NY hospitals.25,26
The purpose of this study was to evaluate changes in NY hospitals in the implementation of recommended maternity care practices, provision of professional lactation support, and reported hospital and patient barriers to breastfeeding support between 2009 and 2014.
Materials and Methods
Study population
All hospitals in NY that provided maternity care services from January 1, 2009, through December 31, 2014, were included. Birth and maternal demographic data were reported as part of the NY Statewide Perinatal Data System (electronic birth certificate records).
Data collection
Hospital breastfeeding surveys
The 2011 and 2014 breastfeeding surveys were developed based on the 2009 survey. 27 The 2009, 2011, and 2014 surveys contained 66, 77, and 78 questions, respectively. Thirty-eight questions were included in all three surveys. The surveys assessed hospital implementation of the 10 Steps to Successful Breastfeeding, distribution of commercial discharge packs with/without formula, provision of professional lactation support, and patient and hospital barriers to breastfeeding success.
At each hospital, a key maternity contact (lactation coordinator or nurse manager) was identified to complete a survey with input from other knowledgeable breastfeeding staff. In 2009, an article survey was used; in 2011 and 2014, surveys were distributed using SurveyMonkey® and responses were collected electronically. Copies of the hospital breastfeeding surveys are available on request.
In all 3 years, the surveys included questions assessing implementation of 9 (Steps 1–7 and Steps 9–10) of the 10 Steps to Successful Breastfeeding. 1 Implementation of Step 8, feeding on demand, was not assessed in these surveys. This step is difficult to assess. Staff have reported confusion in assessing implementation of Step 8 and in defining feeding on demand and feeding cues. 28 In the CDC's Maternity Practices in Infant Nutrition and Care (mPINC) survey, Step 8 was scored as implemented if 90% of mothers were taught to recognize and respond to feeding cues; feeding on demand, per se, was not evaluated. 29 For Step 4, initiate breastfeeding within 1 h of birth, or Step 7, Practice rooming-in, was coded as implemented if 90% or more mothers met the appropriate criteria, which is consistent with the CDC's mPINC survey scoring criteria. 29
The number of professional lactation counseling staff (full-time equivalents) at each hospital was standardized per 1,000 births to calculate a lactation staffing ratio. The United States Lactation Consultant Association (USLCA) has recommended IBCLC staffing ratios (N/1,000 births) to best support and increase the success of breastfeeding. 30 These staffing ratios (1.3, 1.6, and 1.9 IBCLCs per 1,000 births for perinatal level I, II, and III hospitals, respectively) were used to determine if recommendations were met.30,31 The hospital perinatal level was based on the NY Codes, Rules and Regulations, Title 10, Section 721.2. 32 For Regional Perinatal Centers, the guideline for hospital perinatal level III was used.
IRB approval
This study was reviewed and approved by the NY State Department of Health Institutional Review Board.
Statistical analysis
In 2009, 2011, and 2014, hospital breastfeeding surveys from each NY hospital with a maternity unit were collected and survey responses were analyzed. Since responses were received from the same hospitals thrice, statistical procedures appropriate for repeated measurements were used. To evaluate trends in the implementation of maternity care practices (Steps) over time, the generalized estimating equation (GEE) was applied to each variable (excluding Step 8) and to the sum of the nine steps as dependent variables. An independent time variable (with values of 0–2) was used to represent data collected during the three time periods. An unconstructed correlation structure was specified in the GEE. A positive coefficient for the time variable indicated an increasing trend over time; the significance level was set at a p-value of <0.05. GEE was used in the same manner to examine trends in reported barriers to supporting breastfeeding.
Lactation staffing ratios for IBCLCs, Certified Lactation Counselors (CLCs), or “other” lactation staff were generated for each hospital for the three time periods. The changes were not linear over the three time points; therefore, the lactation staffing ratios between 2009 and 2011 and between 2011 and 2014 were assessed using weighted paired t-tests. The IBCLC staffing ratio was compared to the USLCA Staffing Guidelines 31 to determine whether each hospital met the staffing guidelines. The McNemar test was used to test the significance in the changes between 2009–2011 and 2011–2014 to determine whether the hospital met the guidelines.
Hospitals were divided into two groups based on whether they were certified as Baby Friendly or not in 2014. Generalized marginal modeling with GEE estimates were used to test whether the changes over the three survey time points in hospital barriers, steps implemented, or the standardized IBCLC staff ratio differed by Baby-Friendly status.
Hospitals were categorized into four groups based on whether they reported “lack of financial resources” as a barrier to supporting breastfeeding in 2011 and/or 2014 (group 1 reported in neither year; group 2 reported in 2011; group 3 reported in 2014; and group 4 reported in both years). Analysis of variance (ANOVA) was used to compare the mean changes in hospitals' IBCLC staffing ratios by reported lack of financial resources in 2011 and 2014.
Results
The number of NY hospitals providing maternity care decreased from 138 (2009) to 129 (2011) to 126 (2013) and to 125 (2014) because of closures of maternity units and/or hospitals. There was a 4.6% reduction in the number of live births in NY State between 2009 (246,592) and 2013 (235,274), which is consistent with reductions in births seen in the rest of the United States. 33 In 2014, six NY hospitals were certified as Baby Friendly.
Surveys were completed by 138/138 (2009), 128/129 (2011), and 125/125 (2014) NY hospitals that provided maternity care; 124 hospitals completed a survey in all 3 years. The majority of hospitals reported implementation of Step 3 (94%) and Step 5 (86%) (Fig. 1). The implementation of Steps 4, 7, and 9 were low, although Steps 4 and 9 increased significantly (Fig. 1), as did Steps 2 and 6. Implementation of the other five steps did not change significantly.
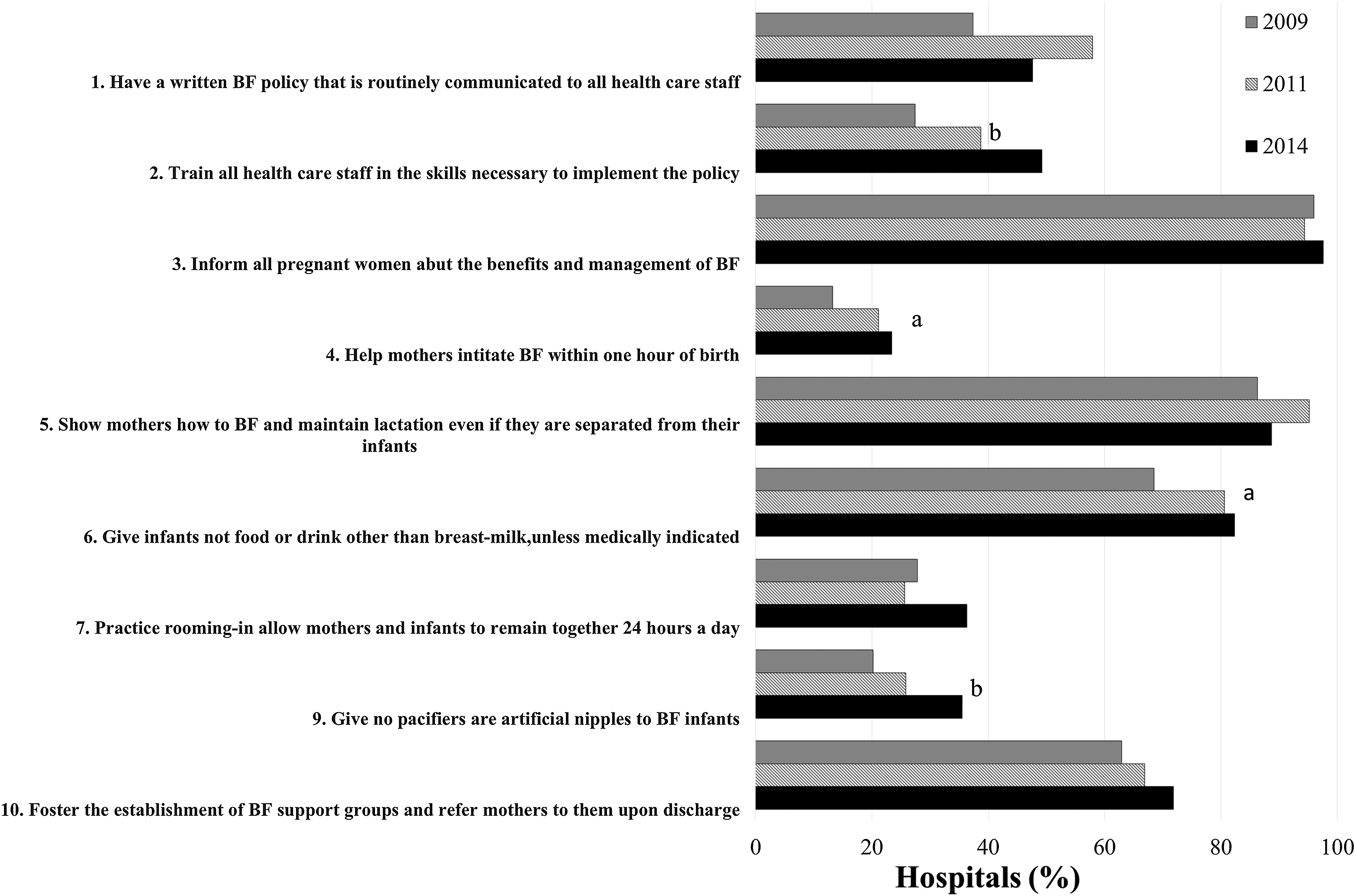
Reported implementation of 9 of 10 Steps to Successful Breastfeeding: 2009, 2011, and 2014. p-Value is for the Wald test of the time coefficient in Generalized Estimating Equation: a, p-value <0.05; b, p-value <0.0005. Step 8, feeding on demand, was not assessed in these surveys.
The mean number of steps implemented by the hospitals increased from 4.33 (2009) to 5.04 (2011) to 5.32 (2014), representing a 23% increase between 2009 and 2014 (p < 0.0001). Only a small percent of hospitals reported implementing all nine steps (0.8%, 2.4%, and 4.0% in 2009, 2011, and 2014, respectively; coefficient for trend = 0.67 with p = 0.089).
There were significant reductions in hospitals reporting that they provided breastfeeding mothers with commercial discharge packs (or gifts) (71%–10%) or free formula samples (32%–2%), or that they allowed formula representatives to visit with hospital staff (70%–28%) (Fig. 2). Furthermore, there was a significant increase in hospitals reporting that they do not provide any formula company materials to breastfeeding mothers (28%–87%).
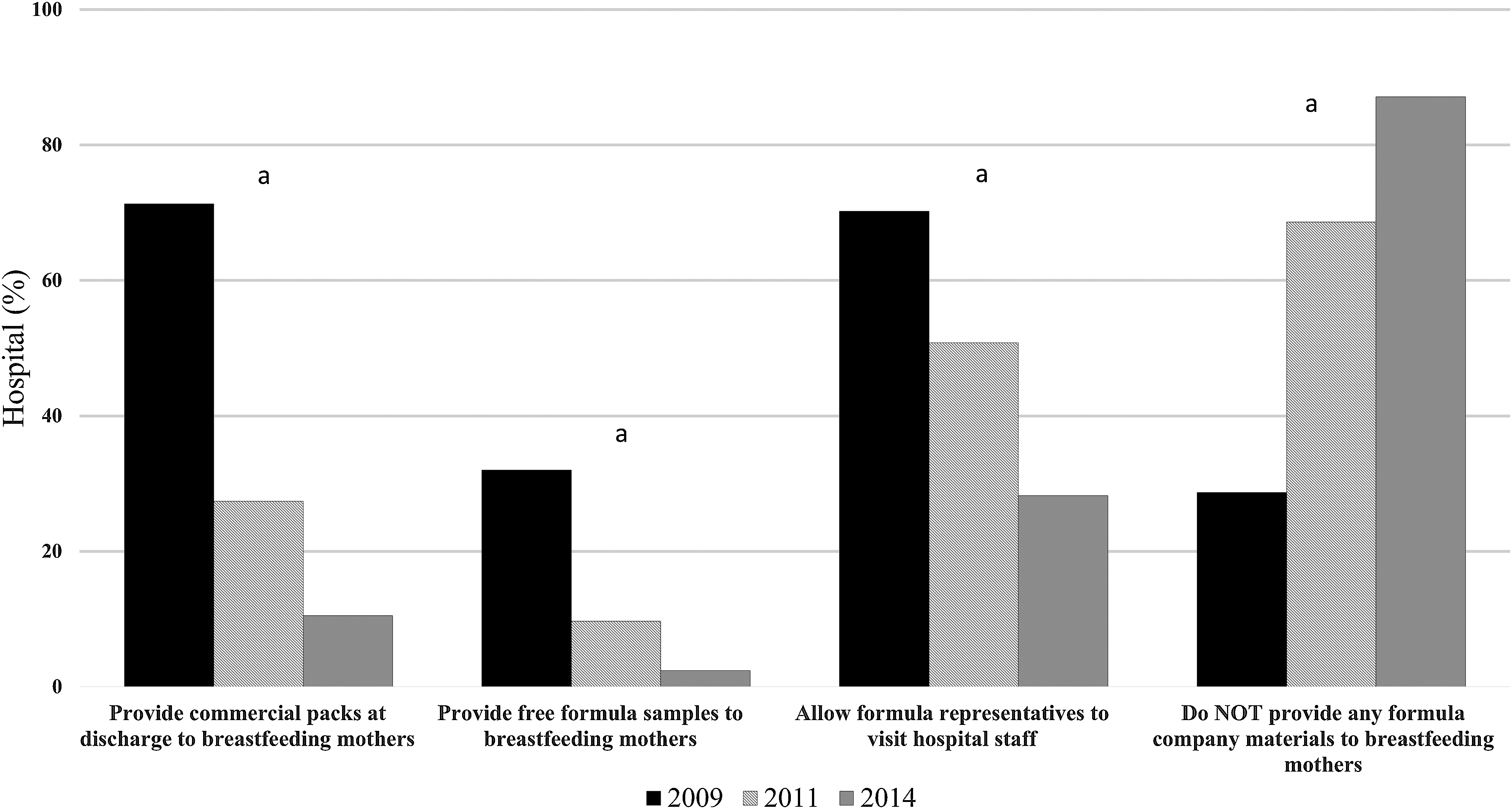
Formula marketing in NY Hospitals, 2009–2014. a, p-value <0.0005. NY, New York.
The professional lactation staffing ratios (N/1,000 births) changed substantially. Staffing ratios for IBCLCs and CLCs increased between 2009 and 2011, followed by a decrease between 2011 and 2014 (Table 1). When the hospitals were stratified by perinatal level, lactation staffing ratios increased significantly between 2009 and 2011 for perinatal level I, II, and III hospitals, but not for the Regional Perinatal Centers, while decreases between 2011 and 2014 were seen among perinatal level I and II hospitals. Consistent with these changes, the percent of perinatal level I and II hospitals that met the USLCA Staffing Guidelines also increased between 2009 and 2011, but decreased between 2011 and 2014.
USLCA Staffing Guidelines for IBCLCs.
CLC, Certified Lactation Counselor; IBCLC, International Board Certified Lactation Consultant; NY, New York; USLCA, United States Lactation Consultant Association; SD, standard deviation; SE, standard error.
The frequency with which barriers to breastfeeding were reported by hospital staff changed (Table 2). There were some improvements. Mixed messages from hospital leaders decreased, from 75% (2009) to 17% (2014). Several other hospital barriers, however, increased, with more hospitals reporting lack of financial resources/support, staff turnover, or inadequate documentation/incomplete records of mother's desire to breastfeed. There were also increases in the hospital staff's perception of patient-related barriers that mothers had not received adequate prenatal education or were unprepared for breastfeeding or that families were not receptive to breastfeeding.
Generalized estimating equations were used to estimate the beta coefficient for time. p-Values were obtained from Wald tests.
The wording for this response differed across years. In 2009, the response read, “Mixed messages from different professional members of staff” and in 2011 and 2014, the response read, “Mixed messages from staff in leadership roles.”
The wording for this response differed across years. In 2009, the response read, “Incomplete records” and in 2011 and 2014, the response read, “Inadequate documentation of mother's desire to breastfeed.”
The changes in the number of steps implemented and the professional lactation staffing ratios did not differ based on a hospital's Baby-Friendly status. Differences were noted for four hospital barriers reported in Table 2, although these must be interpreted cautiously because of the small number of Baby-Friendly hospitals (N = 6). The Baby-Friendly hospitals reported a greater increase than the non-Baby-Friendly hospitals (N = 118), in two barriers: lack of financial resources and no lactation coordinator (p = 0.0043 and p = 0.003, respectively). Lack of staff training did not change overall, but this barrier was reported to increase more by the non-Baby-Friendly hospitals (p = 0.037). Mixed messages from staff were reduced overall, with a greater reduction reported by the non-Baby-Friendly hospitals (p = 0.003).
There were no changes in the percent of hospitals that provided a prenatal care clinic (64–65%) or offered childbirth education classes (90–94%). In addition, almost all prenatal clinics and childbirth classes included a breastfeeding component: 94–96% and 94–97%, respectively (data not shown). There were no statistically significant differences in the mean changes in hospitals' IBCLC lactation staffing ratios and their reported lack of financial resources to support breastfeeding in 2011 and 2014 (ANOVA; p = 0.35).
Discussion
This study found significant increases in the implementation of several key recommended maternity care practices (specifically, Steps 2, 4, 6, and 9) and in the total number of recommended steps to support breastfeeding, suggesting increased compliance with recommended maternity care practices. 5 Of note, the 24% increase seen in the implementation of recommended maternity practices is consistent with the 19% improvement reported by CDC in NY's Composite Quality Practice Score (based on the mPINC surveys), which improved from a score of 67 (2009) to 80 (2013). 26 There are several survey differences: the CDC's most recent mPINC survey was in 2013, while NY's most recent survey was in 2014, and the CDC survey had an 84% response rate compared to 100% response rate for NY's 2014 survey. In addition, NY did not assess Step 8 “feeding on demand,” while the CDC survey used “taught feeding cues” as a surrogate measure, and included several additional measures.
While reported distribution of commercial discharge packs with formula to breastfeeding mothers was lower on NY's surveys (32% in 2009 and 2% in 2014) than on the CDC's surveys (58% in 2009 and 9% in 2013), 26 both sets of surveys found very large reductions in the distribution of packs (94% and 83%, respectively).
The marked increase in hospital professional lactation support between 2009 and 2011 was consistent with increased recognition that lactation counseling is important and needed for successful breastfeeding. The decrease between 2011 and 2014, however, was an unanticipated finding. The reductions in hospital professional lactation support corresponded temporally with hospital financial constraints being cited more frequently as a barrier to breastfeeding support and with reports of reductions in hours and jobs of IBCLCs.34,35 Thus, it was surprising that hospital changes in IBCLC staffing ratios were not related to reported lack of financial resources to support breastfeeding in 2011 and 2014.
While the Affordable Care Act (ACA) calls for comprehensive breastfeeding support and counseling from a trained provider during pregnancy and the postpartum period, the provider's qualifications are not specified, leaving it up to the health insurance companies to define “a trained provider” and determine reimbursement.18,34 The reductions seen between 2011 and 2014 applied to both IBCLCs and CLCs, suggesting that there does not appear to have been a substitution of less skilled for more skilled lactation counselors (i.e., CLCs for IBCLCs). Since the ACA requires that lactation counseling be provided during pregnancy and postpartum, this may have increased opportunities for lactation counselors, allowing some professional lactation staff to move from inpatient to outpatient settings. In addition, the reported increase in staff training and the skills necessary to support breastfeeding policies, 27% (2009 survey) to 49% (2014 survey), may have allowed hospitals to shift some lactation counseling from professional lactation counseling staff to other maternity staff.
In January 2016, the Joint Commission lowered the threshold for mandatory reporting of the Perinatal Care performance measure set to a minimum of 300 births per year (from 1,100), requiring more hospitals to report on exclusive breast milk feeding. 36 Whether this requirement will impact prenatal clinic or inpatient hospital lactation counseling staffing, or the type of lactation counselors employed, is not known. 34
The large reduction in mixed messages from hospital staff leaders or professional members may reflect NY's training and educational efforts to increase professional knowledge and skills to support breastfeeding. Two educational initiatives, Latch On NYC and Great Beginnings NY, were conducted for hospitals in New York City (NYC) (May 2012 through 2014) and hospitals outside NYC (December 2013–October 2014), respectively. Consistent messages would be expected to positively influence breastfeeding initiation and duration.3,17,37 In addition, the increase in patient barriers reported by hospital staff may be due to a real increase or might reflect increased staff awareness because they have received more education.
The reporting that patients' families are not receptive to breastfeeding is of concern as social support from the family, in particular the infant's father, has been shown to be an important determinant of exclusive breastfeeding in the hospital and with longer breastfeeding duration postdischarge.17,38 Equally of concern are the increased reports that new mothers have not received adequate prenatal education or are unprepared for breastfeeding. Current recommendations are to educate the mother, her partner, and support team, so they can empower and support her breastfeeding intentions.16,17,38–42 Lack of preparation for newborn care, including breastfeeding, is associated with increased formula feeding. 42 Attendance at prenatal classes and structured breastfeeding education and lactation counseling have been associated with increased breastfeeding initiation and longer duration of exclusive breastfeeding.12–14,39 While two-thirds of NY hospitals reported providing a prenatal clinic and 95% offered childbirth classes, almost all of which included a breastfeeding component, it is not known what percentage of pregnant women attend childbirth classes, or how comprehensive the breastfeeding education components are.
All three surveys found that 45–52% of hospitals reported that mothers did not like rooming-in. The current public debate about the role of rooming-in, led by the media who have reported stories about mothers' breastfeeding wars and the closing of nurseries and mothers being denied sleep and forced to stay up at night to care for their newborn infant, may contribute to the reported discontent. Even when the infant-mother room-in, staff still provide nursing care and monitor the infant's health status. Efforts to improve mothers' and families' knowledge about breastfeeding and the 10 Steps to Successful Breastfeeding, including rooming-in, are needed to improve understanding, counter misconceptions, and increase preference for rooming-in.
The family or mother's culture was reported by most hospitals, in all 3 years (67–78%), as a barrier to breastfeeding. In a survey of NYC healthcare professions involved in breastfeeding, 76% reported that most of their clients had a cultural background that differed from their own. 43 When measured on cultural competence, only 23% scored as culturally competent. Research finds that breastfeeding counseling by healthcare providers, breastfeeding support at home, community, and the workplace, and attendance at childbirth classes differ by race and ethnicity, all of which influence mothers' feeding decisions and breastfeeding plans. 44 Improving cultural competency and increasing the diversity of the workforce to better match the population served are potential strategies to reduce cultural barriers.
This study has some limitations. First, the study population is from a single state. NY, however, is a large state, with a racially and ethnically-diverse population, and approximately a quarter million births per year. The breastfeeding survey was completed by hospital maternity staff, in a manner similar to the method used in the CDC's mPINC Survey, which was used as a comparison. Thus, both surveys are potentially subject to the same reporting bias.
This study, however, has many strengths. First, participation by hospitals was very high (100% in 2009 and 2014 and 99% in 2011). The hospital surveys were available from three separate years, which allowed the measurement of changes within each hospital over time. Many of the CDC mPINC survey questions were derived from earlier versions of breastfeeding surveys in NY, which improves the comparability between surveys. These many strengths outweigh the weaknesses.
Conclusion
This study shows increased implementation of several recommended maternity care practices and a large reduction in the distribution of commercial packs and formula samples by NY hospitals. These improvements in maternity care were countered by the reported reductions in hospital inpatient professional lactation counseling support and increases in financial and patient barriers to breastfeeding. Future studies are needed to assess the reasons and effects of reduced professional lactation support and increased patient barriers on breastfeeding success. Efforts to ensure comprehensive breastfeeding education and lactation counseling that reaches more women and their families during pregnancy, the birth hospitalization, and the postpartum period are needed. In addition, more NY hospitals should implement all the recommended practices to support optimal breastfeeding outcomes and ensure the full benefits of maternal and infant health for all New Yorkers.
Footnotes
Acknowledgments
Thanks goes to Kristen Murphy for her work on the 2014 Hospital Breastfeeding Survey. Support for this project was provided by the Robert Wood Johnson Foundation's Public Health Law Research program (Grant No. 12-069) and the NY State Department of Health. These findings do not necessarily represent the views of the funders.
Disclosure Statement
No competing financial interests exist.