
Abstract
Abstract
Background:
In Thailand, ginger is a popular natural galactagogue among breastfeeding women. However, there has never been evidence to support the effectiveness of ginger in increasing the breast milk volume.
Objectives:
To compare breast milk volume on the third and seventh day postpartum between lactating mothers who receive 500 mg dried ginger capsules twice daily with those receiving placebo.
Materials and Methods:
A randomized, double-blind controlled trial was conducted. Women who deliver a term baby were randomly assigned to receive dried ginger or placebo for 7 days postpartum. Breast milk volume was measured on third day postpartum using test weight method for a period of 24 hours and on seventh day postpartum using 1 hour milk production. We also compared the third day serum prolactin level between the two groups.
Results:
Data from 63 women were available for analysis, 30 from the ginger group and 33 from the placebo group. The two groups were similar regarding baseline characteristics. Women in the ginger group have higher milk volume than the placebo group (191.0 ± 71.2 mL/day versus 135.0 ± 61.5 mL/day, p < 0.01). However, the seventh day milk volume in the ginger group does not differ from the placebo group (80.0 ± 58.5 mL versus 112.1 ± 91.6 mL, p = 0.24). The mean serum prolactin levels were similar in both groups (321.5 ± 131.8 ng/L in the ginger group, and 331.4 ± 100.7 ng/L in the placebo group, p = 0.74). No side effect was reported in this study.
Conclusion:
Ginger is a promising natural galactagogue to improve breast milk volume in the immediate postpartum period without any notable side effect.
Introduction
I
A study by Ushiroyama T. found that postpartum women who receive Xiong-gui-tiao-xue-yin, a traditional Chinese medicine that contains 1 g of ginger rhizome as one of the multiple herbal ingredients, have more daily breast milk volume on day 4–6 postpartum and a higher level of serum prolactin on day 1 postpartum. 6 Therefore, we designed a double-blinded, randomized controlled trial to compare the breast milk volume during the early postpartum period between women receiving dried ginger capsules with those receiving placebo.
Ginger (the root of Zingiber officinale) is a common flavoring agent and condiment in many cuisines worldwide and is also a well-known herbal remedy for many health conditions. 7 The active ingredients of ginger are Gingerols, Shogaol, Zingerone, and Paradol. 8 Many medicinal properties of ginger have been reported, which include antiemetic, antioxidant, and anti-inflammatory.9,10 Ginger also has the property of warming up the peripheral temperature presumably by the effect of vasodilatation, 11 a mechanism that may explain its possibility to boost the milk production through increased blood supply of the lactating breasts.
There was no study regarding the safety of ginger use during the nursing period. However, ginger is considered safe during pregnancy. A study by Choi et al. has shown that ginger consumption during pregnancy does not increase the risk of fetal malformation. 12
The objective of this study is to compare the breast milk volume during the early postpartum period between women receiving dried ginger capsules with those receiving placebo.
Materials and Methods
We conduct a randomized, double-blind controlled trial at HRH Princess Maha Jakri Sirindhorn Medical Center, Nakorn Nayok, Thailand, during August 2015–April 2016. This study was registered with Thai Clinical Trials Registry (registration number: TCTR20151001002). The ethical approval has been granted by the Human Research Ethics Committee, Srinakharinwirot University (registration number SWUEC/F-090/2558). Healthy pregnant women aged 18 years and above who deliver a term baby (≥37 weeks gestation) at our hospital and aim to exclusively breastfeed her baby for at least 6 months were eligible for enrollment.
Participants who had serious medical conditions presumed to result in mother–infant separation and decreased breastfeeding frequency (e.g., postpartum hemorrhage, postpartum sepsis), allergic to ginger, or have a contraindication to breastfeeding such as HIV infection were excluded from the study. Immediately after delivery, a research nurse screened the antenatal record and performed a short interview to identify eligible women. After consent was obtained, the participants were randomized to receive either 1000 mg/day of dried ginger capsule orally (ginger group) or placebo (placebo group).
Randomization was done using a computer-generated list with block of four methods. After the allocation sequence was generated, the researcher enclosed dried ginger capsules or placebo in the sequentially numbered sealed envelopes. These envelopes were kept with the midwife who opened each envelope when a new participant was recruited at the time of her delivery. All women received the enclosed capsules at the dosage of one capsule (500 mg) twice daily for 7 days postpartum, with the first dose started within 2 hours after her delivery. Neither the midwife nor the patient was aware of the treatment group. The group allocation list was kept confidential and only revealed after completion of data collection process.
The dried ginger capsule used in this study was identical with the placebo. Both were prepared by research and development pharmacists at Abhaibhubejhr herbal company specifically for this study. Each capsule contains either 500 mg of dried ginger or 500 mg of corn starch. The dried ginger powder was prepared according to good manufacturing practice.
After delivery, all women received the hospital standard postpartum care along with breastfeeding support procedures. Breastfeeding was initiated within 1 hour after delivery in all women. The mothers were encouraged to breastfeed their baby as frequently as she desires or whenever her baby gives a hunger cue, but the interval between each feeding should not exceed 4 hours. The participants were instructed to keep a record of the time she takes her assigned capsules, the time that the baby was breastfed, and frequency of the baby's stool and urine. LATCH score was evaluated at 24 hours postpartum by a trained midwife.
We recorded the breast milk volume on the third and seventh day postpartum. We chose the third day as the primary measurement time point because it represents the timing of stage II lactogenesis. However, the seventh day time point was chosen due to logistical reasons, as women are routinely scheduled for a follow-up visit one week after delivery. On the third day (48–72 hour), when the mothers were still in the hospital, we used the test weighing method. The weighing procedure was started exactly at 48 hours after the delivery time in all participants. The research nurse weighted the infant fully clothed before and after each feeding with an electronic weigh scale (Zepper® EB-20, accurate to 5 g) for the period of 24 hours. The sum of weight difference in gram was then converted to breast milk volume in milliliter (1 g = 1 mL). This method was deemed comparable with the measurement of breast milk volume based on deuterium oxide dilution technique. 13 Because some galactagogues stimulate milk supply by increasing the level of serum prolactin, we also measured the serum prolactin in this study. The maternal serum prolactin was measured on the third day postpartum. A blood sample was drawn by a research nurse early in the morning (8–9 am) and at least 1 hour after the last feeding to avoid diurnal variation and effects of infant suckling on serum prolactin level.
On the seventh day postpartum, the mothers were appointed for a follow-up visit. The medication compliance along with side effects was checked with the participant. The compliance was checked with both reviewing the log sheet written by the participants and counting of the leftover capsules. At this visit, we measured the 1-hour milk production. The mothers were first asked to empty their breast using an electronic breast pump (Spectra® S1). After an hour, both breasts were then pumped again for 15 minutes to measure the 1-hour breast milk volume. We used the 1-hour breast milk volume instead of the 24 hour test weighing because it offers more practicality. In a study by Lai et al., the hourly pumped breast milk volume was compared with hourly milk production calculated from the test weighing procedure over 24 hours. The result shows that the average hourly volumes obtained from the second to seventh hour were not significantly different from the average hourly breast milk volume using the test weighing method over 24 hours. In our study, we empty both breasts before recording the 1-hour breast milk volume. Therefore, our 1-hour volume would equal the second hour breast milk in a study by Lai et al., which means it has the potential to represent the 24-hour breast milk production. 14
According to the study by Turkyılmaz et al., the average breast milk volume on 3 days postpartum was 38.8 ± 16.3 mL. We expected that women receiving ginger would produce 30% more breast milk and determined that 31 participants were required in each study arm. This calculation was based on a two-tail α level of 0.05 and 80% power. Adjusting for 10% dropout rate, the final sample size was 34 for each study arm. Statistical analysis was done using SPSS version14 (SPSS, Inc., Chicago, IL). Student's t-test and Chi-square tests were used to compare the characteristics between the two groups. A p-value of less than 0.05 was considered statistically significant.
Results
One hundred eight women were assessed for eligibility. Twenty five did not meet the inclusion criteria, and 15 denied to participate in the study. A total number of 68 women were enrolled, and 34 were randomly assigned to each study group. For the ginger group, four participants were excluded (three withdrew from the study, and one developed postpartum endometritis and sepsis). For the placebo group, one participant was excluded due to withdrawal from the study for personal reason.
A total number of 30 participants in the ginger arm and 33 participants in the placebo arm completed the assessment of breast milk volume and serum prolactin on third day postpartum. However, 15 women in the ginger group and 21 women in the placebo group come to follow up at seventh day postpartum. A flow chart of the number of participants through the study was shown in Figure 1. All participants who come to the seventh day follow up have taken all of the assigned capsules and none report any side effect.
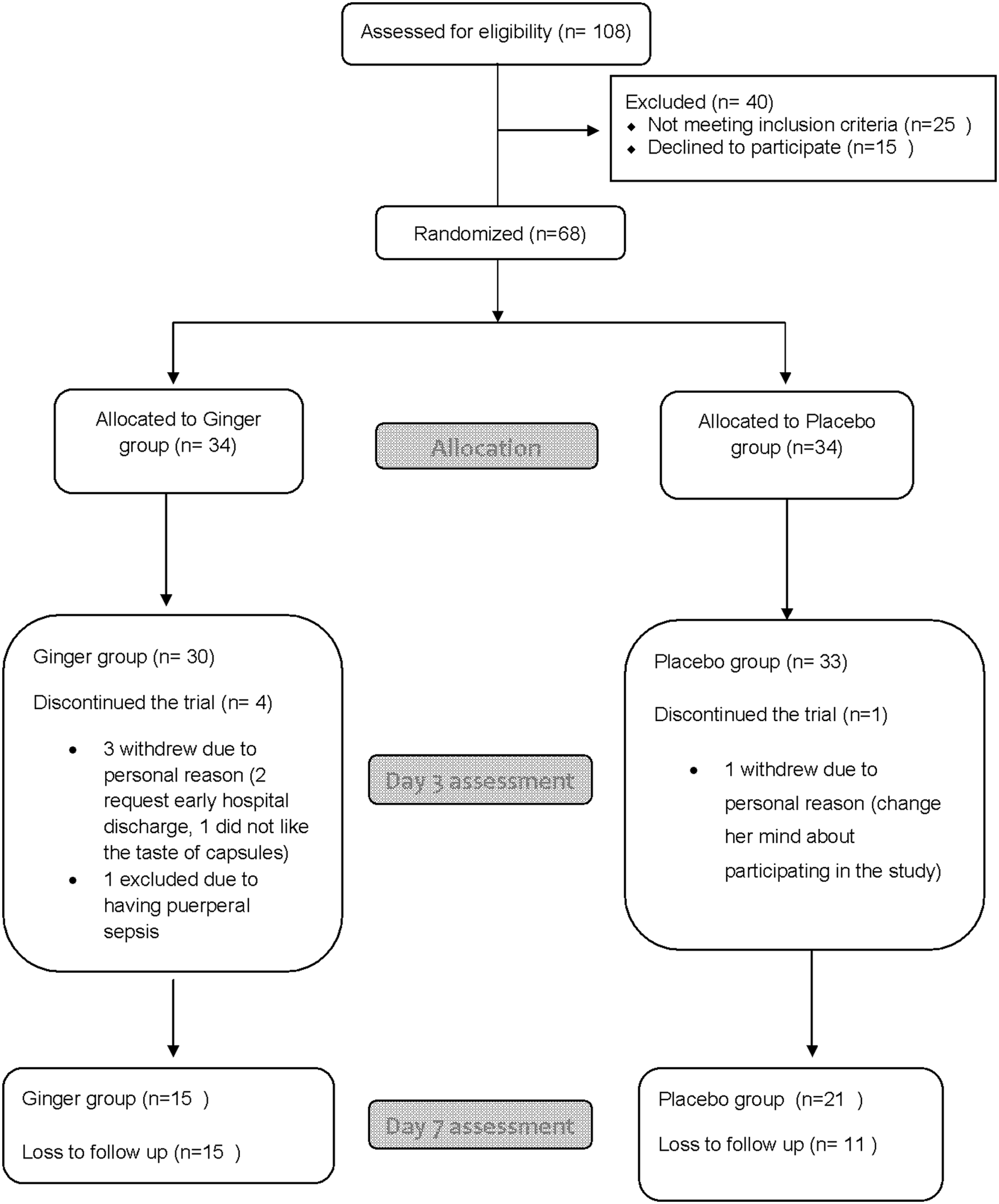
CONSORT flow diagram of participants through the study.
Maternal age, parity, gestational age, intrapartum use of oxytocin, baby gender, birth weight, latch score, and breastfeeding frequency were similar in both groups (Table 1).
The differences in breast milk volume and serum prolactin between the two groups are shown in Table 2. There was a statistically significant difference in third day breast milk volume between the two groups (p < 0.01). The nursing mother in the ginger group has higher milk volume (191.0 ± 71.2 mL) than the placebo group (135.0 ± 61.5 mL). However, the seventh day milk volume in the ginger group does not differ from the placebo group (80.0 ± 58.5 mL versus 112.1 ± 91.6 mL, p = 0.24). The mean serum prolactin levels were similar in both groups (321.5 ± 131.8 in the ginger group, and 331.4 ± 100.7 in the placebo group, p = 0.74).
Statistically significant p < 0.05.
Discussion
The result from this study suggests that ginger increases breast milk volume in the early postpartum period. We measure the breast milk volume on the third day (48–72 hour) as this period represents the average timing of stage II lactogenesis. 15 The 24-hour breast milk volume in our placebo group was 135.0 ± 61.5 mL, which is comparable with the previous study. 6 The mean difference of third day breast milk volume between the ginger and the placebo group was 56 mL/24 hour. This amount of breast milk accounts to 41.4% increment from milk volume of the placebo group. However, such an effect was not demonstrated on the seventh day postpartum, on which we measured the 1-hour breast milk production volume. The 1-hour milk production method was used instead of 24-hour test weighing method on the seventh day follow-up because of its feasibility. The measurement procedure can be completed within a two-hour visit. We design such an outcome measurement with an assumption that the 1-hour breast milk production represents the 24-hour milk production. However, the seventh day measurement fails to show a difference between the ginger group and the placebo group. The discrepancy between the third and the seventh day result is possibly because breast milk volume in a later phase of lactation is largely regulated by infant's individual need and it may dilute the effect of ginger on increasing milk supply.
Some galactagogues such as dopamine antagonists stimulate milk supply by increasing the level of serum prolactin, a lactogenic hormone that promotes breast milk synthesis. However, such a mechanism may not explain how ginger increases breast milk volume, as the average serum prolactin level was similar in both the ginger and placebo group in our study. How ginger increased breast milk supply is not well understood. We hypothesize that ginger induces systemic vasodilatation and increases blood supply to the mammary glands, based on previous evidence that ginger increases peripheral body temperature in human 11 and causes vasodilatation in rats. 16
The limitation of our study is that many participants were lost to follow-up on the seventh day postpartum, resulting in a low and disproportionate number of participants in each study group. Telephone calls were made, where possible, to identify the reasons for not returning to a scheduled follow-up. Most of the absent participants reported that commuting to the hospital is inconvenient for them. The small number of seventh day breast milk volume data available for analysis weakens the integrity of the results. Also, it should be noted that the assessment of seventh day breast milk volume using the 1-hour pumped milk volume may not accurately indicate the actual milk supply in many women, as the pumped volume can be affected by many factors, such as pump fit, maternal discomfort with the pump, and time of the day. We suggest that additional studies with larger sample sizes and more stringent measurement of breast milk volume in the later phase of lactation are needed to confirm the efficacy of ginger on increasing breast milk volume in postpartum women.
Conclusion
Ginger can be a promising natural galactagogue to improve breast milk volume in the immediate postpartum period without any notable side effect. However, more studies with larger sample size and more rigorous methods of measuring milk production are needed to determine the effect of ginger at greater than 3 days postpartum before it can be recommended for use in clinical practice. The mechanism of how ginger increases breast milk is not well understood, but the study result suggests that it may not be through stimulation of serum prolactin.
Footnotes
Acknowledgment
This research was supported by research funding from Faculty of Medicine, Srinakarinwirot University.
Disclosure Statement
No competing financial interests exist.