
Abstract
Abstract
Background:
Breastfeeding provides many health benefits for mothers and their infants that span their life course. Despite this, national breastfeeding rates are below benchmarks set by the CDC (Centers for Disease Control and Prevention). Breastfeeding rates in the Detroit low-income population are particularly low.
Objective:
To measure the effect of hospital-based prenatal and postnatal breastfeeding interventions on breastfeeding initiation and continuation rates in a low-income population. The interventions implemented were a prenatal breastfeeding education curriculum and a hospital-based breastfeeding support group.
Methods:
A total of 650 women were tracked via chart review and telephone survey after delivery to assess breastfeeding initiation, continuation, and goal achievement. The baseline group (n = 330) received care in the hospital-associated prenatal clinic before intervention implementation; the postintervention group (n = 320) received breastfeeding education and had a hospital-based breastfeeding support group made available to them, in which some participated. Data were analyzed using the chi-squared test and the Student's t-test.
Results:
Breastfeeding initiation rates were greater in the postintervention group (p < 0.0001). The breastfeeding continuation rate at or beyond 6 months did not differ among baseline and postintervention groups (p = 0.5), but was greater among women who also participated in the breastfeeding support group compared with women who participated in the prenatal intervention alone. Participation in interventions did not affect the rate, at which women reported meeting their breastfeeding goals.
Conclusion:
Both prenatal education and ongoing postdischarge support are needed to improve breastfeeding continuation.
Introduction
B
Breastfeeding rates in Michigan are below those reported for the nation. In Michigan, 69.3% of mothers initiated breastfeeding in 2011, and 42.9% were still breastfeeding at 6 months, compared with 74.6% and 44.3% nationally. 19 Breastfeeding rates in Detroit, Michigan, a large urban center with a primarily African American population, are even lower.20,21 39.5% of Detroit mothers initiated breastfeeding, and 17.0% of those who initiated continued to breastfeed at least 6 months.
The regional disparity in breastfeeding rates, in which Detroit women breastfeed less than their counterparts, likely contribute to the Detroit infant mortality rate, 22 which was twice that of the state of Michigan at 13.6 per 1,000 births 23 at the time of the present study. The infant mortality rate of Detroit African American infants was even higher at 14.8, 1.5 times the mortality rate of their white counterparts.
In the African American population, low breastfeeding rates have been attributed to the lack of education about the benefits of breastfeeding from healthcare workers, 24 misconceptions about lifestyle constraints while breastfeeding, 25 and lack of generational support. 26 Other studies emphasize that barriers to providing breastfeeding education are exaggerated in healthcare settings that serve low-income populations. 27
In accordance with these findings, the Surgeon General's Call to Action for Breastfeeding 28 listed culturally competent prenatal education, structured discharge programs, and peer support as priority strategies to close economic and racial gaps in breastfeeding outcomes. The Baby-Friendly Hospital Initiative (BFHI) also embraces these strategies 29 with specific requirements for prenatal and postnatal support to promote breastfeeding and optimal hospital care for mothers and their infants. The objective of the present study was to observe the effects of hospital implemented prenatal and postnatal breastfeeding interventions on breastfeeding initiation and continuation rates of a primarily low-income population with a historically low breastfeeding rate.
Subjects and Methods
The present study is a pre/postquasi-experimental study designed with a baseline group selected before intervention implementation and a postintervention group. Study protocol was approved by the St. John Hospital and Medical Center Institutional Review Board (IRB).
Study site
The present study was conducted in an urban teaching hospital in Detroit, Michigan with ∼3,000 deliveries per year. The overall breastfeeding initiation rate of women delivering at the study site before the study period was ∼50%. At the start of the study, the hospital was in the early stages of Baby-Friendly pathway implementation. The hospital supports a Resident Obstetrics Prenatal clinic that is staffed by obstetrics and gynecology residents and hospital-employed faculty staff and primarily serves Medicaid-insured patients.
Subjects
Subjects were recruited for the study between September 2011 and October 2014. The baseline preintervention group comprised 330 randomly selected women older than 18 years of age who had delivered infants at the study site and sought care in the site prenatal clinic in the 12-month period before intervention implementation. The postintervention group comprised 320 women older than 18 years of age who consented to participate in one-on-one breastfeeding prenatal counseling in the site-associated prenatal clinic and delivered at the study site. All women attending the prenatal clinic were approached to participate. Participation in the study was voluntary, and participants were recruited using opt-out methods, in which patients were able to decline participation. Baseline participants were consented by telephone, and postintervention participants were approached for consent for participation by an International Board Certified Lactation Consultant (IBCLC) at the study site if they met the study criteria.
Interventions
Study interventions were twofold and comprised prenatal and postnatal interventions. The prenatal intervention consisted of a breastfeeding-focused prenatal education curriculum offered at the site-associated resident prenatal clinic delivered one-on-one by an IBCLC. The postnatal intervention consisted of a breastfeeding support group for breastfeeding mothers who had received prenatal care at the site-associated clinic.
Prenatal intervention
The prenatal study intervention implemented a 10-visit optional breastfeeding curriculum delivered one-on-one to patients by IBCLCs in the waiting room of the clinic. The delivery of the education in the waiting room was Health Insurance Portability and Accountability Act (HIPAA) compliant. The curriculum included oral education and printed handouts to address breastfeeding knowledge gaps identified by lactation staff, cultural elements, and breastfeeding benefits and barriers. The titles of the 10 lessons were as follows: Health Benefits of Breastfeeding for Baby, Health Benefits of Breastfeeding for Mom, Support for Breastfeeding, Common Questions, Questions from Moms, Babies Who Are Premature or Have Health Problems, Taking Care of Mom, Pumping and Breastfeeding, and Going Back to Work or School and Pumping Breast milk.
Postnatal intervention
A free on-site breastfeeding support group was established as the postnatal intervention. The group was led by a breastfeeding peer counselor from the area, who was also employed as a Women, Infants, and Children (WIC) peer counselor. The support group was designed to be unstructured and to focus on mothers' breastfeeding questions and concerns. Both breastfeeding postpartum women and pregnant women could participate. The sessions were held once a week. Women were provided with free transportation services, through a contract with a local taxi company, and a light lunch. The group was open to mothers that delivered at different hospitals, although these mothers were not enrolled in the study nor included in final data analyses. Group participation was encouraged through direct referrals, flyers, and a Facebook page.
Methods
A total of 855 women were consented in the study. Women enrolled in the postintervention group who were unable to be reached in three attempts for a telephone survey were excluded in data analysis. Medical records of mothers and the infants in both the baseline and postintervention groups were reviewed after delivery by the research team to determine race, insurance, gestational age, mother's age, extent of prenatal care, breastfeeding initiation, and neonatal intensive care.
Both baseline and postintervention mothers completed a structured telephone survey with IRB-approved questions regarding infant feeding methods, breastfeeding continuation, breastfeeding influences and experiences, breastfeeding goals, barriers to reaching breastfeeding goals, and how helpful they found the interventions, in which they participated in the case of the postintervention participants. The telephone survey was accomplished by a single research assistant who was not involved in prenatal education delivery. The survey was designed to be given to women who had completely discontinued breastfeeding; those who reported they were still breastfeeding were called again at a later time. Surveys were initiated 1 to 3 months after delivery and were ongoing throughout the study; they were completed up to over 2 years postpartum. Breastfeeding continuation data were self-reported recall data. Breastfeeding initiation was either obtained from electronic medical record review or was self-reported in the telephone survey.
Analysis
Descriptive statistics were generated to characterize baseline and postintervention groups. Data were analyzed using the chi-squared test and Student's t-test. Odds ratios were performed to explore the differences found between the two groups. All data were analyzed with SPSS v 23.0 and a p-value of 0.05 or less was considered to indicate statistical significance.
Results
Demographics and clinical characteristics
The demographics and clinical characteristics of the two groups are summarized in Table 1. Mothers in both groups were primarily African American and Medicaid-insured. While some differences between the baseline and postintervention groups were not significant, duration of prenatal care (baseline mean = 8.8 ± 1.0 versus postintervention 7.9 ± 2.5 months, p < 0.0001), gestational age at delivery (baseline = 38.0 ± 2.5 versus postintervention 38.4 ± 2.1, p = 0.01), insurance providers (baseline Medicaid/Medicaid health maintenance organization (HMO) = 89.7% versus postintervention 91.4%, p = 0.004), infants in need of neonatal intensive care (baseline = 16.1% versus postintervention 7.3%, p = 0.001), and percent of women initiating breastfeeding with previous experience (baseline = 47.9% versus postintervention 37.6%, p = 0.038) were significantly different between the two groups. Odds ratio analysis was allowed for gestational age, maternal age, extent of prenatal care, and need for neonatal intensive care and performed to analyze effect on breastfeeding initiation and breastfeeding duration.
Data are mean ± standard deviation values or number (%). Not all characteristics sum to total due to missing data.
p < 0.05 indicates a significant difference.
—, not applicable; HMO, health maintenance organization; LOS, length of stay; NICU, neonatal intensive care unit; SJ, St. John Hospital & Medical Center.
Prenatal intervention
Postintervention subjects attended the prenatal clinic and were seen an average of 3.2 times (SD = 2.7, range: 1–26) by an IBCLC for breastfeeding education. The breastfeeding education intervention had a significant effect on breastfeeding initiation (Fig. 1), with 71.9% of women breastfeeding in the postintervention group and 51.5% of women breastfeeding in the baseline group (p < 0.0001). Even when controlling for significant demographic and clinical differences, mothers in the postintervention group were significantly more likely to breastfeed (p = 0.027, OR = 1.7) compared with mothers in the baseline group.
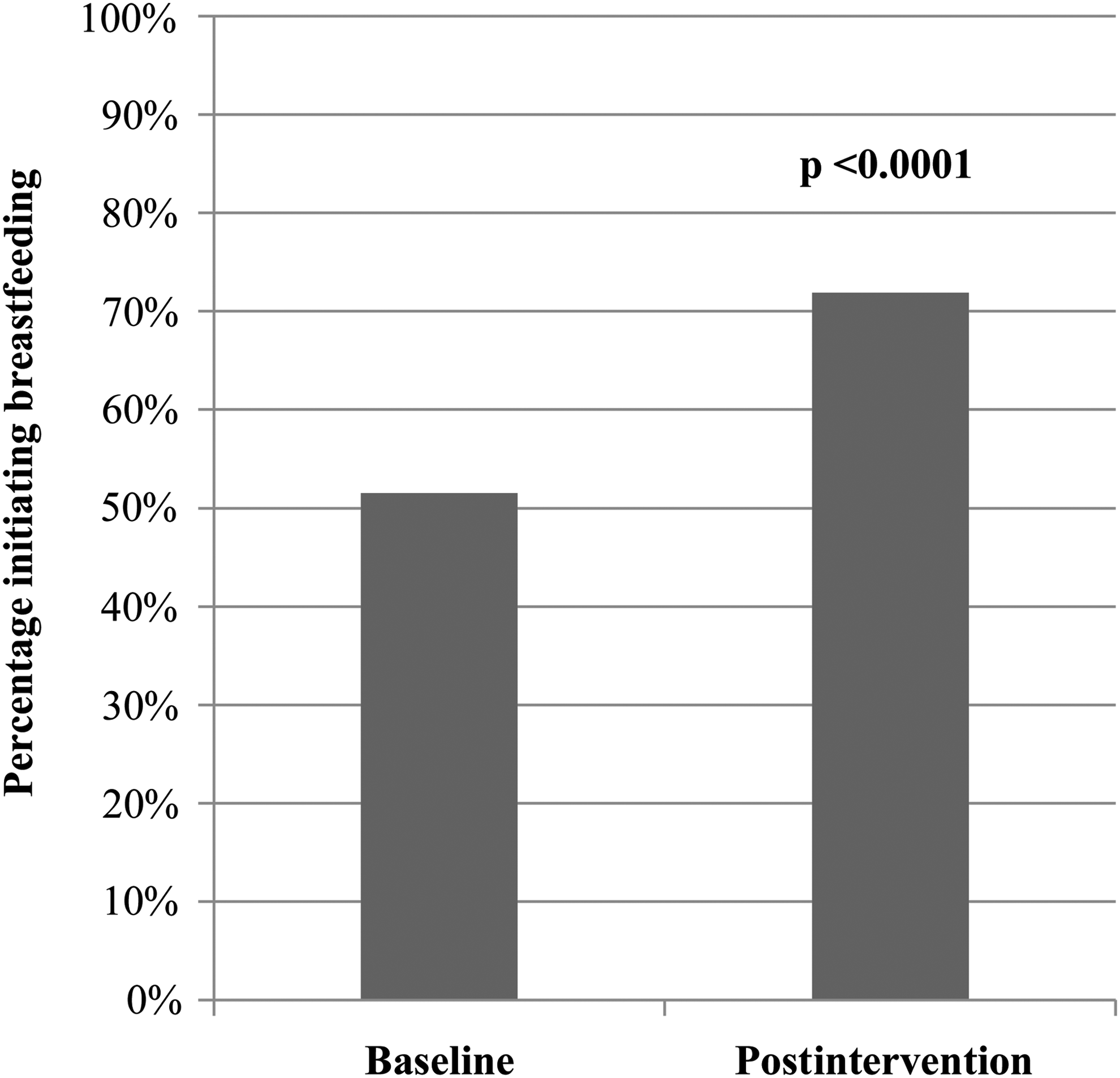
Women initiating breastfeeding (%) in baseline (n = 330) and postintervention groups (n = 320).
Most women reported the prenatal breastfeeding education had an impact on feeding decisions and behavior (Table 2). Ninety-two percent of breastfeeding women in the postintervention group reported prenatal visits with the lactation consultants influenced their feeding decisions, and 79% of breastfeeding women also reported the prenatal visits helped them prolong their breastfeeding experience.
Data are number (%).
—, not applicable.
Postnatal intervention
In addition to participating in the prenatal intervention, some women participated in the peer-led breastfeeding support group. The average number of visits to the group was 3.15 (SD = 9.1, range: 1–50). While breastfeeding continuation was not affected by prenatal education only (Fig. 2A; mean baseline 4.3 ± 4.9 versus postintervention 4.0 ± 4.2 months, p = 0.5), participation in both the prenatal education and peer-led support group significantly increased length of breastfeeding continuation (Fig. 2B). Fifty-nine percent of breastfeeding women who participated in both the prenatal education and the support group breastfed for at least 6 months compared with 28% of breastfeeding women who participated in the prenatal education alone. Over 95% of participating women reported that the support group was influential in their decision to continue breastfeeding (Table 2).
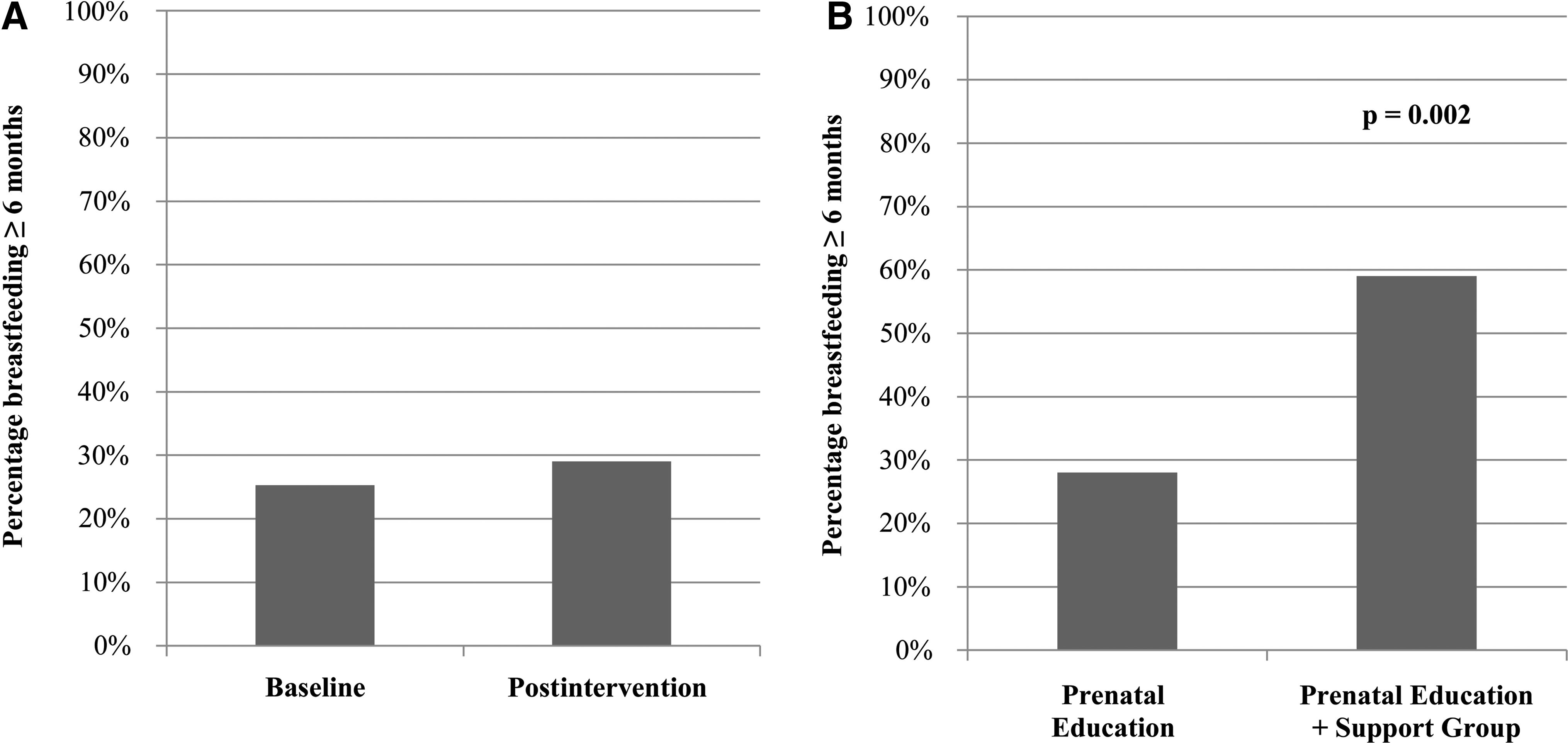
Breastfeeding continuation (%) at or beyond 6 months among breastfeeding women in
Only a small fraction of women from both groups reported meeting their breastfeeding goal, with 35.3% of women in the postintervention group reporting achievement and 28% of women in the baseline group (p = 0.14). Barriers to goal achievement reported by breastfeeding women were not statistically different between the two groups (Table 3). In both intervention and baseline groups, milk supply was the most highly cited problem area.
Data are number (%). Not all surveyed answered all questions.
Discussion
Previous studies have examined the effectiveness of prenatal education, especially when delivered one-on-one.30–32 Furthermore, other studies have shown the effectiveness of postnatal breastfeeding support 33 and peer-led support groups.34,35
The two interventions in the present study informed by these findings were instituted to expand breastfeeding support and foster increased breastfeeding initiation and duration. While an increase in breastfeeding initiation was observed following participation in a breastfeeding-focused curriculum, breastfeeding continuation was prolonged only with additional continued postdischarge peer support. Our findings suggest that both breastfeeding education and support throughout the prenatal and postnatal period are required to impact breastfeeding initiation and prolong breastfeeding in an urban population with lower breastfeeding rates. Our study design allows for the demonstration of the impact of a continuum of breastfeeding support that extends upstream and downstream from beyond the hospital setting.
One factor that may have contributed to the success of the prenatal breastfeeding education intervention in improving breastfeeding initiation is the one-on-one delivery of the prenatal education. Contact with an IBCLC has repeatedly been found to improve breastfeeding outcomes.36,37 Prenatal one-on-one counseling with an IBCLC is unique, as typically interactions between dyads and IBCLCs in a hospital setting occur postnatally. In addition, the prenatal education and the breastfeeding support group were both staffed through the same department to ensure consistent messaging.
Second, the hospital-based nature of the breastfeeding support group may have contributed to its effect on continuation. The hospital setting was familiar to the mothers and may have contributed to attendance and retention. The provision of food and transportation represented important incentives. Food was considered important to the breastfeeding support group due to widespread food security issues in the study area, and Detroit lacks an adequate public transportation system. The model has been sustainable during funding gaps as the health system has supported the breastfeeding support group given the illustrated benefit. Multiple transportation methods have been explored to reduce cost, including for-profit options and Medicaid. The provision of food has also been sustainable through private food donations from local businesses.
Our study differs from previous studies, in which the design allowed us to examine the additive effect of these two interventions. A significant strength of the study is the prolonged follow-up (up to 2 years). This allowed us to address intervention effect on breastfeeding continuation.
The findings are limited by some confounding factors. Women who were not interested in breastfeeding may have been more likely to decline participation in the study. The hospital offered comprehensive inpatient lactation support before Baby-Friendly engagement with the partial implementation of evidence-based care, but during the intervention timeline, the birthing center began participating in the BFHI and preparing for designation. Quality improvements on the birthing center, with the integration of comprehensive evidence-based maternity care practices, may have influenced breastfeeding initiation and continuation. However, the interviews conducted show the mothers feel that the prenatal education intervention specifically influenced their decision to breastfeed. Our study is also limited by its reliance on subject recall for some measures, including breastfeeding continuation. Moreover, the population represented in this study is difficult to contact by telephone, and those who could not be surveyed could not be included. At the time of the study, texting patients was not an option due to privacy constraints
Next steps
The prenatal education and the breastfeeding support groups have continued after the conclusion of the study. The prenatal education curriculum has been changed to a more culturally competent and literacy-sensitive Baby-Friendly compliant educational curriculum that is also being used by local WIC agencies and the local home-visiting community, providing consistent breastfeeding messaging to the broader care continuum. The education in the prenatal clinic is currently delivered by peer counselors and lactation consultants-in-training. The support group remains active and vibrant and is now integrated into a local Strong Start for Mothers and Newborns initiative. The Strong Start initiative also provides prenatal clinical support that is consistent with the prenatal clinic breastfeeding messaging.
Conclusion
Meaningful prenatal breastfeeding education increases breastfeeding initiation, but both prenatal education and postnatal support are needed to improve breastfeeding continuation. Breastfeeding outcomes can be improved in the low-income African American population with application of these interventions. This study is of particular relevance for hospitals on the Baby-Friendly pathway. In addition to mandated prenatal education, such programs should consider the creation of a hospital-based support group to allow for continuity and consistency of prenatal and postnatal education. This will represent meaningful and effective implementation of the Baby-Friendly pathway.
Future studies should focus on improving breastfeeding outcomes further by improving delivery, content, and cultural competency, so that mothers will feel that they achieve their breastfeeding goals. Coordination of breastfeeding messages with the local healthcare community should also result in improved outcomes for all, regardless of geography and demographics.
Footnotes
Acknowledgments
This research was supported by grants from the W. K. Kellogg Foundation, Blue Cross Blue Shield of Michigan Foundation, and Comerica Charitable Foundation. We like to acknowledge the lactation consultants of St. John Hospital and Medical Center, who tirelessly delivered the prenatal education: Mary Maher, BSN, RN, IBCLC; Carol Pokladek, BSPA, RN, IBCLC; Jeannene Sulewski, BSN, RN, IBCLC; Blair Malian, BSN, RN, IBCLC; and Kim Winarski, BSN, RN, IBCLC. We like to acknowledge Monica Washington, peer counselor, who led the Mother Nurture Club with kindness and enthusiasm.
Disclosure Statement
No competing financial interests exist.