
Abstract
Abstract
Introduction:
An emerging trend in Academic Medical Centers (AMCs) is to coordinate breastfeeding care, research, and trainee education through “medical director” positions. Little is known about their duties, supports, and challenges.
Objective:
To determine the duties and challenges of directors of breastfeeding medicine in AMCs.
Methods:
A survey was distributed four times over a 3-month period to three listservs with a total of 860 members. Physicians directing breastfeeding programs or services at AMCs were included. Participants were asked about details of their employment, time distribution of the position, their role in education, billing practices, and major hurdles.
Results:
Thirty-two physicians responded to the survey: 25 from the United States, and seven international. Only 22% of respondents had formal job descriptions and only 31% reported being paid for their breastfeeding work. Most positions were created in the past 10 years (75%), were housed in Departments of Pediatrics (75%), and provided clinical services for breastfeeding in inpatient and outpatient settings. Ninety-one percent of respondents educated trainees and provided oversight of lactation consultants. Major hurdles included difficulties with billing for services, lack of protected time and personal reimbursement, lack of formal structure and job descriptions, and lack of buy-in at the institutional and sometimes governmental levels.
Conclusions:
Medical Directors of Breastfeeding Services may be increasingly prevalent in AMCs and are engaged in inpatient and outpatient clinical work, trainee education, and lactation consultant oversight. Both financial and structural hurdles were reported by those holding these positions.
Introduction
B
Nevertheless, with more than 50 years of breastfeeding advocates in the medical field, there is a growing group of physicians specializing in the care and management of breastfeeding, creating programs to support breastfeeding mothers, conducting research in breastfeeding, and training the next generation of providers. For these physicians, duties have historically been included under other employment conditions: working in a newborn nursery, pediatric, obstetric, or family medicine practice, or in a research position. 14 Making breastfeeding a primary career focus has tended to require personal efforts to establish and grow private outpatient practices, although there are little data on how many such centers currently exist. Shaikh and Smilie reported in 2008 on 13 physician-led outpatient breastfeeding practices. 14 They described that 10 of these practices had affiliations with teaching hospitals or AMCs, 6 educated medical students, and 9 educated house staff.
Due to the work of these pioneers and advocates, an emerging trend is to formalize such activities in AMCs by creating positions of medical directorship. These may serve to highlight a center's commitment to the field, increase focused resources, improve possibilities for quality improvement, increase access to appropriate care, and increase market share.
Anecdotally, physicians providing breastfeeding medicine services report having many competing interests, responsibilities outside of breastfeeding medicine, and a lack of protected time, job description, and pay for their breastfeeding-related work.
Objective
To determine the job descriptions, educational duties, reimbursement, and challenges of directors of breastfeeding medicine in AMCs.
Methods
An e-mail listserv was created through the Academy of Breastfeeding Medicine (ABM), an international organization of physicians dedicated to the promotion and protection of breastfeeding, to serve as a networking and liaison for medical directors of breastfeeding. A survey was created with input from medical directors at academic centers and input on survey questions was solicited from the listserv members. The survey was distributed four times over a 3-month period to the following three e-mail groups: the Medical Directors ABM listserv (n = 42), the general ABM members listserv (n = 288), and the American Academy of Pediatrics (AAP) Section on Breastfeeding listserv (n = 530). Snowball sampling methods were used to extend the reach of the survey and ensure capture of known medical directors. Inclusion criteria were physicians directing breastfeeding programs or services at AMCs. Participants were asked about details of their employment, time distribution of the position, their role in education, billing practices, and major hurdles.
Results
Thirty-two physicians responded to the survey: 25 from the United States, two from Canada, and one from each of the following: Croatia, Bolivia, Mexico, New Zealand, and Spain. While only 17 (53%) had job titles of “medical director” for breastfeeding, another four respondents had job titles specifically related to breastfeeding leadership. Despite this, only 7 (22%) had formal job descriptions associated with their breastfeeding roles and only 10 (31%) reported being paid for their breastfeeding work (as opposed to other clinical or research work). Most positions were created in the past 10 years, and 11 (34%) were created in the past 0–2 years (Fig. 1). All but three respondents had held their position as long as it had been in existence.
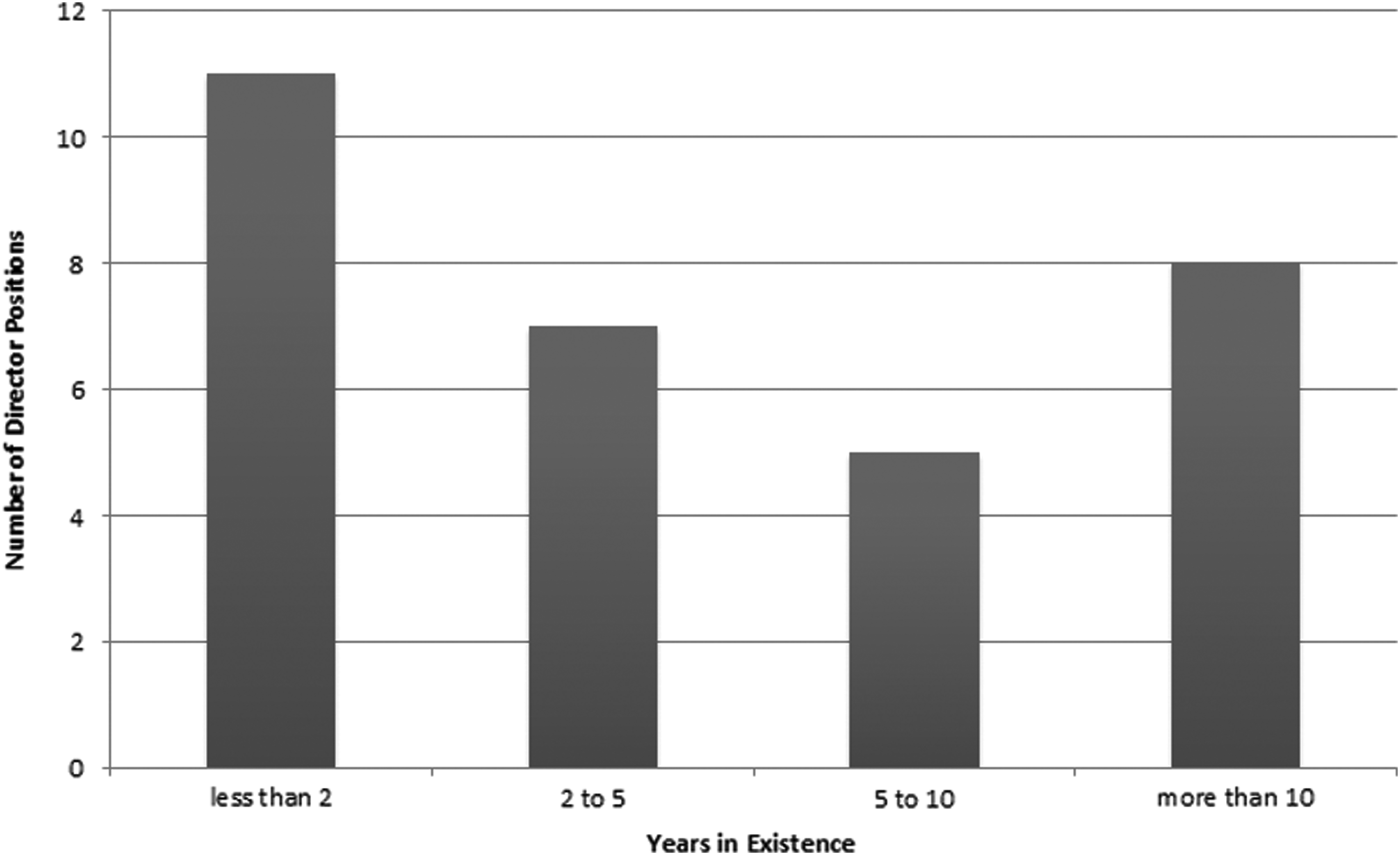
Years in existence of medical director position in academic medical center.
Departmental ownership and duties
Most positions were housed in Departments of Pediatrics (n = 24, 75%), four were housed in Obstetrics and Gynecology (OBGYN) departments, three were in Family Medicine, one was joint Pediatrics and OBGYN, and one was joint Family Medicine and Pediatrics. Two positions were not housed in an academic department, one position was in a Hospital Quality, Education, and Investigation department and no positions were housed in Preventive Medicine. Figure 2 describes the time distribution of duties for these positions and includes 30 positions (94%) that provide outpatient breastfeeding medicine and 24 (75%) that provide inpatient breastfeeding medicine, although 17 positions (53%) had 50% or more clinical time outside of breastfeeding medicine. Most positions included nonclinical time: 29 (91%) had time to provide education, 28 (88%) had some amount of research time, 25 (78%) had time to direct breastfeeding services, and 26 (81%) had other administrative time.
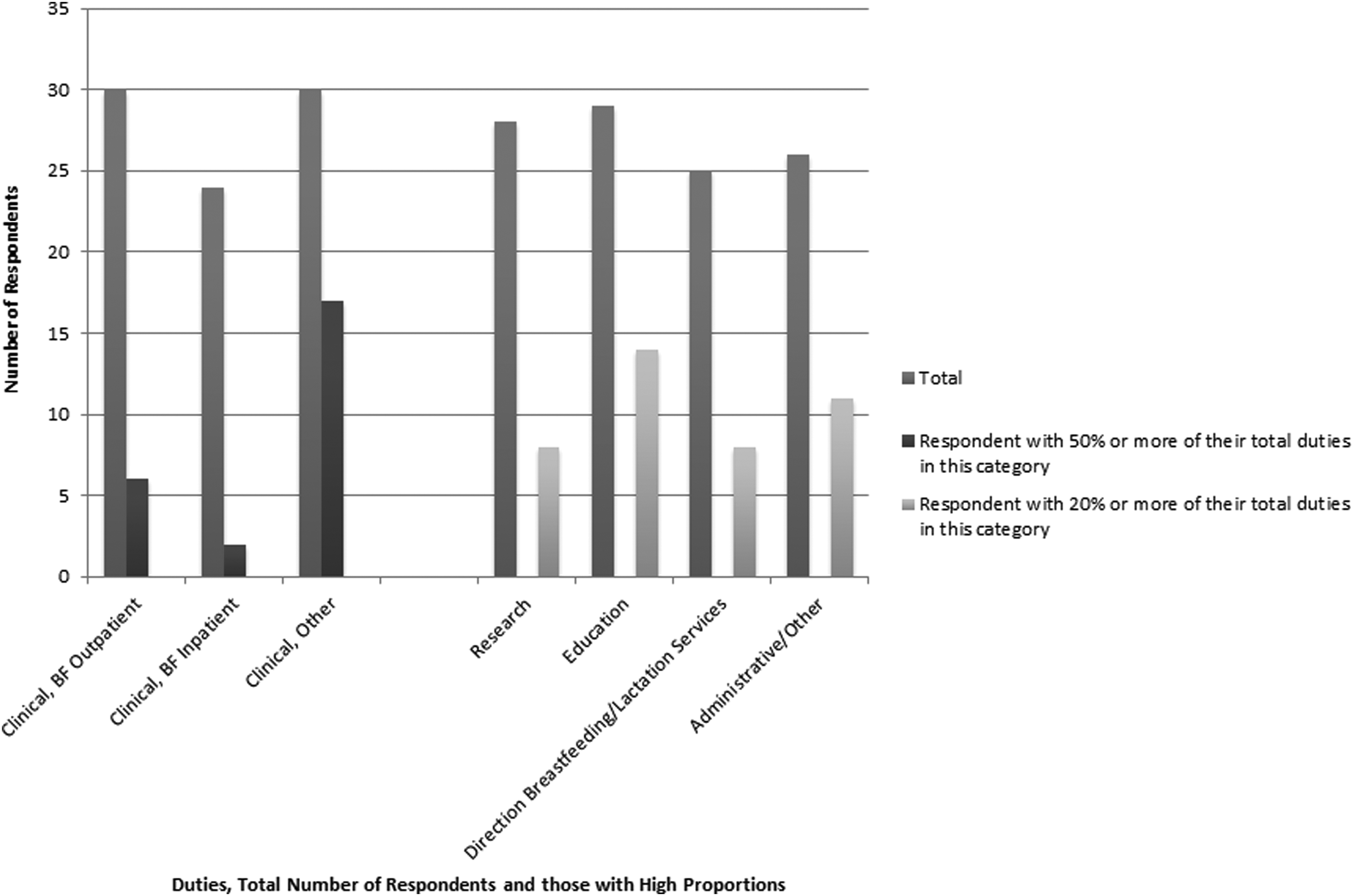
Clinical and other duties of medical directors of breastfeeding at academic medical centers.
Clinical services
Clinical services for breastfeeding were provided in inpatient and outpatient settings. Most respondents indicated personally providing breastfeeding services in outpatient hospital-affiliated practices (n = 18, 56%), six in private outpatient practices, and one in a government-affiliated outpatient practice. For inpatient breastfeeding, many provided services in the neonatal intensive care unit (NICU) or newborn nursery (n = 15, 47%), while eight provided services on inpatient pediatric floors, seven on inpatient obstetric floors, and two reported providing services university wide (Fig. 3).
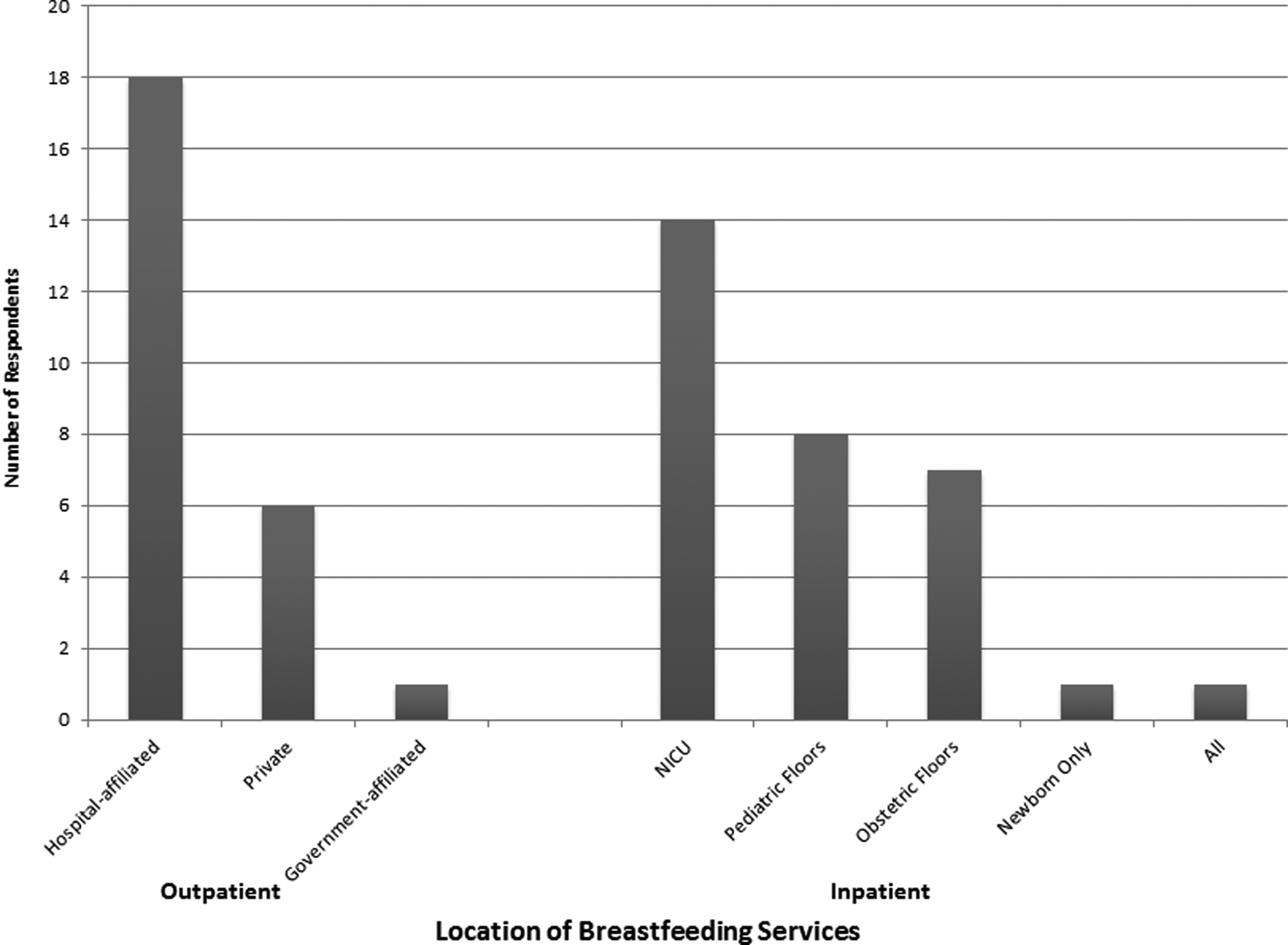
Breastfeeding service delivery locations.
Lactation oversight and billing
Almost all respondents reported providing oversight of lactation consultants or others providing lactation services (n = 29, 91%), although only six (19%) use incident-to billing (billing “behind” the International Board Certified Lactation Consultant (IBCLC), who sees the patient before the physician, United States) and none use the Medicaid S-codes (Affordable Care Act provision to cover lactation services delivered by an IBCLC). Other billing practices for physician time included using E + M codes (billing for time, n = 17, 53%), consult codes (n = 3), fee-for-service (New Zealand, n = 1), Régie de l'assurance maladie, Quebec, Canada (n = 1), and billing out of pocket (Mexico, n = 1). Five reported not billing for services, although two of those billed under different headings (clinical services NICU and National Health Service). Of those billing (n = 27), 17 (63%) bill for the baby, 15 (56%) for the mother, and 10 (37%) for both.
Education
Education of trainees was a component of almost all positions (n = 29, 91%). Those not providing trainee education reported three barriers: (i) not having medical trainees, although education was provided for nurses, (ii) lack of a formal structure for the position, and (iii) lack of university/other department buy-in. The majority of training was provided to Pediatric residents (n = 18, 62%), while fewer reported training Family Medicine residents (n = 15, 52%) and even fewer reported training OBGYN residents (n = 9, 31%). Many reported training medical students (n = 20, 69%), while 12 (41%) trained nurse practitioners, physician assistants, or midwifery trainees and one person each reported training the following: fellows, medical assistants and staff, public health students, and “health professionals.” Most respondents involved with training had formal curricula, including work with a medical provider (physician, midwife, nurse practitioner, or physician's assistant) (n = 26, 90%) and many trainees shadowed an IBCLC (n = 20, 69%). Barriers to providing this education included the following: (i) lack of time (n = 7); (ii) lack of buy-in from departments and training programs (n = 7); (iii) limited opportunities for exposure to trainees (n = 6) especially outside of pediatrics; (iv) no budget (n = 4); and (v) few opportunities for exposure to breastfeeding moms (n = 1).
Major hurdles
Hurdles expressed by medical directors included financial and structural issues. Seven respondents reported experiencing insurance coverage and billing as a major hurdle to their position, four reported lack of salary support for their own position, and three reported a lack of adequate salary support for IBCLCs. On the structural front, five noted lack of support or buy-in from hospitals and medical staff and three reported no formal structure or title for their position as a hurdle. Less frequently reported hurdles included the following: influence from formula companies; lack of role's oversight of IBCLCs; knowledge/quality of IBCLCs; inconsistency of feeding plans in NICU; getting donor milk into the NICU; difficulties in acting as a mediator between physicians and IBCLCs; and not being a board-certified specialty.
Discussion
Medical Directors of Breastfeeding Medicine at AMCs can be found internationally. It appears that these positions may be increasingly prevalent, since most survey respondents held positions created in the past 10 years, and many in the past 2 years. Furthermore, it is possible that many of these positions were created through substantial individual advocacy, as most of the physicians in these positions appear to have originated them. Unsurprisingly, there is wide variation in the duties and clinical services associated with these positions.
Despite their expertise and expressed need for more time, many respondents (53%) had more than 50% of their duties in nonbreastfeeding-related clinical work, which is consistent with prior findings. 14 Most (78%) had no formal job description and were not being paid for their work in breastfeeding (69%), both noted to be major hurdles to respondents. Despite this, almost all (91%) reported being involved in training and working with lactation consultants, which are hopeful signs that advanced breastfeeding knowledge may be increasingly integrated into medical education and that physician co-ownership of the field may be increasingly prevalent. Training was also reported to be well received by trainees and lactation consultants, who are often included in trainee education (69%). Most of the positions (75%) are housed solely in Departments of Pediatrics, which may be a reason why some directors expressed frustration with the lack of access to other types of trainees.
Many reported providing breastfeeding clinical services in outpatient hospital-affiliated settings (56%), which is encouraging given the historically hospital-focused approach of the past Baby-Friendly Hospital Initiative (BFHI). Billing practices varied by site and country, with some respondents unable to bill for services at all. Billing was noted to be a major hurdle for medical directors, both at the national and health insurance level, and creates limitations on the amount of services provided to patients. Respondents also reported a lack of protected time to provide breastfeeding services and a lack of personal reimbursement for their work. A need was expressed for increased physician networking and advancement of this field.
The integration of a new subspecialty such as Breastfeeding Medicine into the mission and practices of AMCs faces particular challenges, particularly when considering the certain role of AMCs in the safety net and the shifting sands of billing and reimbursement. Other types of new subspecialties such as Hospital, Preventive, and Integrative Medicine (IM) have faced similar challenges in recent years. Eisenberg et al. reported on the needs of establishing an IM Program in an AMC, reflecting on the need to “[develop] optimal delivery models whereby individuals can responsibly access IM services safely, effectively, and reproducibly across medical settings in a coordinated and cost-effective way.” 15 Our survey indicates that substantial variation in practice similarly exists in the field of Breastfeeding Medicine within AMCs, and optimal delivery models are lacking and need to be considered. How to manage these services, standardize and implement curricula for trainees, engage in much-needed quality improvement activities, support employees, and develop ongoing quality research are also considerations that should begin to shape the entry of Breastfeeding Medicine into AMCs. Our survey sought to elaborate some basic aspects of current positions and programs, in an effort to begin a conversation that may shape their future development and dissemination.
Limitations
This survey included a limited sample, based on respondents from three commonly used listservs in this population. This limited respondents and did not fully reach an international, non-English-speaking population. However, it is likely that physicians achieving these types of positions would be part of these national (AAP, United States) and international (ABM) groups. In addition, the survey tools were not previously validated.
Conclusions
Medical Directors of Breastfeeding Services may be increasingly common in AMCs and are engaged in both inpatient and outpatient clinical work and education. These positions often include work with IBCLCs and include IBCLCs in their medical trainee education. Major hurdles are reported by those holding these positions, including difficulties with billing for services, lack of formal structure and job descriptions, lack of protected time and personal reimbursement, and lack of buy-in at the institutional and sometimes governmental levels.
Footnotes
Acknowledgments
The author would like to acknowledge the input of Drs. Anne Eglash and Karen Bodnar and the members of the Academy of Breastfeeding Medicine Medical Directors Listserv for their input.
Disclosure Statement
No competing financial interests exist.