
Abstract

T
Everyone knows the phrase, “The road to hell is paved with good intentions.” It captures the message that change needs more than good intention. To promote breastfeeding, we need intentional, definitive action and I will tell you what I mean by that. Making a healthy choice is a good intention of many of us. One that often eludes us. Intentional illuminated action is manifest by a phrase I use often—“When the easy choice is the healthy choice. Then we have arrived.” Compare a ten dollar salad that is very healthy to a two dollar cheesesteak. Which is the easy choice? Obviously it is the cheesesteak. And so how do we change it so we make the easy choice is the healthy choice?
As a general internist, I've spent a lot of time helping people who have very common, unhealthy habits. I help them to migrate toward habits that are unfamiliar and healthy. That migration is often challenging. When adopting breastfeeding, a woman may be the first person in her family system to do so. This is comparable to the journey of moving from the familiar and less healthy (bottle feeding) to the unfamiliar but healthier (breastfeeding). So how do we make breastfeeding the easy choice?
Sometimes having compelling data works. Many times we need to take risks, to overcome barriers and create opportunities.
There are compelling data that support the conclusion that breastfeeding promotes the health of both a woman and her child. The maternal pro-health arguments—well documented by multiple authors—include those in the short term, the faster involution of the postpartum uterus, less postnatal bleeding, and increased postdelivery weight loss. All outcomes that women may find appealing. Longer term health advantages included lower rates of obesity, diabetes, and cancer prevention.1,2 These longer term advantages, especially in young women, may not be as appreciated or valued as those that are short term. So framing the benefits in a way that is perceived to be value added is important.
For infants, the health promotion list is far longer. We have less late-onset sepsis, lower rates of preterm infant births. Also lower rates of sudden infant death syndrome (SIDS), necrotizing enterocolitis, otitis media, diarrheal illnesses, and respiratory infections. Longer term benefits include lower rates of diabetes, cancers, and childhood infections.3,4
However, in contrast to maternal benefits, the challenge is how do we present this as value added to a pregnant mother? For first-time mothers, pregnancy can be a time of anxiety (e.g., “Is this normal?” “Should this be happening?” “What if..?”). For other mothers and for most people, avoiding unpleasant possibilities is more likely than spending precious energy on “scary” what-ifs.
A value-added approach would be to present benefits in a way that frames it from a functional impact. So, for example, a severe diarrheal illness can happen in the middle of the night, resulting in an emergency department visit. Preventing that disruption by breastfeeding would be very helpful.
So, instead of “You should breastfeed so the following things don't happen to you infant” you could present this as “Do you really want to be in the emergency room at 2:00 or 3:00 in the morning with your child having a respiratory or diarrheal illness? If breastfeeding can prevent this from happening, would that not be better?” You could also engage women with a vision of her soon to be newborn as a healthy toddler, child, and adult. For example, “What if your child could avoid having weight problems (obesity), getting diabetes, or even getting cancer, just by breastfeeding him or her?”
When we look at who is at risk for not breastfeeding, we see the impact of poverty. As a nation, we have moved from the “haves” and “have-nots,” to many desperate, destitute, developing country-like conditions in our urban centers.
One such in my city of Philadelphia is North Philadelphia. But we are not unique. All of our cities (and even our rural poor) have too many similar places. When I was in the Executive Leadership in Academic Medicine (ELAM) program, we had colleagues who were from the Americas (e.g., United States and Canada).
In the last week of the fellowship, one of our colleagues coordinated a car tour to showcase our respective Philadelphia medical institutions. And as we went to North Philadelphia, our colleague from Canada, a pediatric endocrinologist, looked out the window. She looked at the boarded shops. She looked at the litter. She looked at the homeless, and she started to cry. And she said, “How can you choose to do this to your own people? This does not make any sense. You are the richest country in the world and yet you choose to let this happen.” With her comments, the car went quiet. She was right. The blight we all drove by and ignored on many days was suddenly seen. Her comments hit home regarding our collective responsibility.
The devastating issues of poverty and the devastating concentration in terms of communities in poverty need to be something that we address. Some authors speak of our zip codes being a health hazard. Breastfeeding demographics vary based on poverty, race, and age. About one in five (21%) of women who live six times above poverty level breast feed. In contrast to the only 12% who live below the poverty line. Other authors emphasize this point by highlighting that mothers below poverty line are 19 percent less likely to breast feed than mothers 350 percent above it.5,6
Racial difference include that the highest rates of breastfeeding occur in women who are white (21%), with the mean rate, and those found in Hispanic women, the second highest rate (16%). The lowest rates are among women who are black (9%). Age of mother also plays a role. Teenagers are at highest risk. We'll discuss why that may occur shortly.
Poverty and discrimination are overt, but there are also multiple, hidden burdens that preclude breastfeeding. First and foremost, if not fundamentally, are issues associated with trauma, specifically psychological trauma. Trauma often plays a role in individuals' lives.
But before we delve deeper, let's evaluate how normal brain functioning occurs. When we are faced with a challenge and successfully resolve it, our brains use their neural pathways to problem solve and we get rewarded with a bit of pleasure-associated hormone (e.g., dopamine). If we don't resolve it, we may not get the pleasure hormone and may be a bit frustrated. In contrast, individuals who have had trauma have impeded neural pathways. In fact, their pathways look like intertwined, tangle bundles. When they become challenged, they often get stuck in an endless loop.
The event triggers remembrances of the trauma wrapped in negative associations and messages and be easily overwhelming to the person. The role of how trauma impairs health and being fully functional can be understood if we compare a computer to a brain.
When just out of the box, loaded with memory and power, your computer can be very fast and effective—a pleasure to use. But often, over time, malware, spyware, and corrupted programs can “get in” to your system resulting in significant slowing. As you try to use your computer, it feels as if something is constantly “playing in the background” and robbing the computer of its memory and speed. The neurocognitive and functional implications of trauma can function in a similar way with humans.
Often when we refer to trauma, we envision the extremes like a prisoner of war. That type of trauma is obvious, however, most is not. For many, it can be overlooked or unnoticed by others. What the event was, how much happened, or the dose or load can all vary. The traumatic event can be devastating, while to some eyes not very significant. But even something seemingly minor can be very traumatizing to an individual. In simple terms one can say that within the brains of some traumatized patients, it is as if the post-traumatic stress symptoms are constantly “playing in the background.” This results in a patient being hypervigilant and reactive.
Needless to say, having this disruption impedes performance. Events can trigger memories that instead of being effectively or efficiently processed within the lightning fast neural pathways become entangled in webs that are bound up in ways that revisit past trauma and its associated feelings.
Another consequence of a trauma history is that it affects the person's filter that they use to view the world. This results in anticipation and interpretation that may be skewed. For example, if the taxi bypasses you, you may experience a “meltdown” and get upset “of course they treated me poorly!” This negative event then triggers the remembrance of other bad experiences.
Without past trauma, you have the resilience to say “This ticks me off, but I'm not going to let it ruin my day.” Trauma plays an important and often overlooked role in the lives of women. So a history of trauma leaves a tangled web in brain processing, affects thinking, emotion, and decision-making. Screening to assess this is important for good healthcare.
If you could look inside the brains of a healthy newly born child, you would find a lot of white space or white matter and very few nerve bundles. Very quickly after birth, the network of nerves rapidly starts to develop to generate a nervous system. This occurs in nontraumatized infants.
It is a different story for newborns who live in traumatic households. Babies developing in this environment are highly stressed. Their stress hormones, known as “fight or flight” hormones, are elevated and stay elevated since there is no relief to the stress. Looking at these children's brain development, we see a different picture.
Instead of rapidly growing and developing a robust neural network, the brains stay unpopulated of neurons with only white matter due to stress hormones, which are known to be neuro-inhibitory. As these newborns grow, this trauma effects normal brain development, especially the frontal lobe that is responsible for judgment, language, and problem solving. So trauma is neuro-inhibitory in human development.
One of my colleagues, Dr. Sandy Bloom, has greatly contributed to the field of trauma.7–10 Her work expands that of the Adverse Childhood Experiences Study (Fig. 1). The sentinel article in the trauma field by Felitti and Anda in 1998 evaluated categories of childhood trauma exposure in about 13,000 adults in a Health Maintenance Organization (HMO) setting in San Diego.
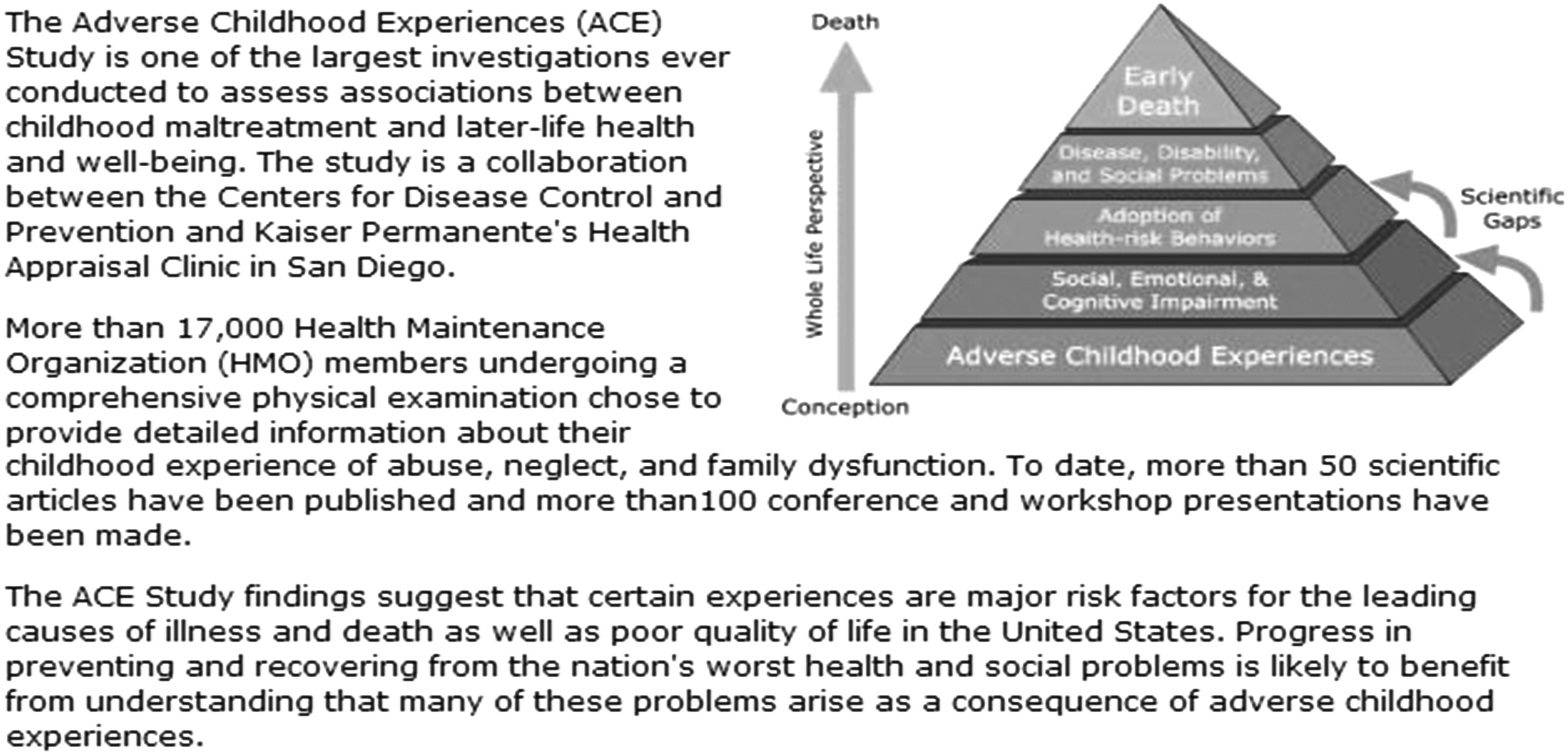
The role of adverse childhood experiences on later poor health outcomes. Created by A. Núñez.
Individuals in this study were predominantly white and college educated patients. There were seven trauma exposure categories, which included various types of abuse, living with someone with mental illness, substance abuse issue, suicidal, or with a history of incarceration. About half the sample scored positive in one category. One quarter of them had more than or equal to two positive categories.
People with four or more categories had poorer health outcomes in 40 conditions. This study highlighted a dose-related impact of childhood trauma on later adverse health outcomes. I found this study very interesting in identifying a common risk factor—childhood trauma and its association with poor health behaviors and outcomes such as earlier smoking rates, unwanted pregnancies, and deaths from heart attacks.
It is important to remember that the Felitti study was done in a reasonably well off community. Trauma rates are likely higher in areas of poverty, stress, and economic turmoil. But to what degree is awareness of trauma and poor health screening for and addressed in clinical medicine? Currently, awareness by healthcare providers is still a bit limited. Pediatricians certainly are effective at screening children. But it is rare that adult healthcare providers ask about childhood traumas, or even any trauma that does not result in a physical outcome. Internists are expected to ask about childhood infectious disease such as measles or physical events such as a fracture. It is not a routine part of the examination to ask “Has anything bad every happened to you? When you were growing up was their violence in your home? Anyone with mental health, substance abuse issues? Incarceration?” We need to do better trauma screening in primary care. Current practice results in missed opportunities that may uncover the underpinning of adverse outcomes.
Regarding breastfeeding this is equally true. Lack of routine trauma history screening is a missed opportunity to uncover and address a barrier as well as identify that healing needs to happen. In the United States, one in four children suffers abuse. If that abuse is sexual, the consequences can result in hypersexualized attitudes toward the body. Breasts are then exclusively sexual organs, not a source of connection and nurturance for a newborn. An issue we will explore later in knowledge and attitudinal barriers.
Dr. Bloom's model is called Sanctuary, and it is a framework to evaluate trauma. She creates interventions to help people heal from trauma. Her acronym for this is S.E.L.F. The following areas aid in the description of a traumatized person and also help in interventions and treatments.
The “S” of S.E.L.F. stands for safety. Traumatized people may never, ever have felt safe in their lives. The “E” of the acronym is for emotions. Often people living with untreated trauma have difficulty accurately identifying emotions and effectively regulating them.
The “L” stands for loss. The transition that occurs when we help others help themselves heal can only occur if the patient “loses” the status quo. For some people who have suffered innumerable losses, it may be too hard to endure another loss. Without the ability to do so, patients are unlikely to improve.
The “F” represents future. The momentum to propel exploring safety and emotions, to lose the status quo happens as a result of embracing optimism. The belief that “things will get better” or that “tomorrow will be a better day.”
Dr. Bloom recommends we shift our language with traumatized patients. Instead of saying “What is wrong with you?” it is preferable to ask “What happened to you?”
Another powerful image that is useful for healthcare providers is the “Trauma Triangle.” Dr. Bloom describes this as having three points—Rescuer, Victim, and Perpetrator (Fig. 2).
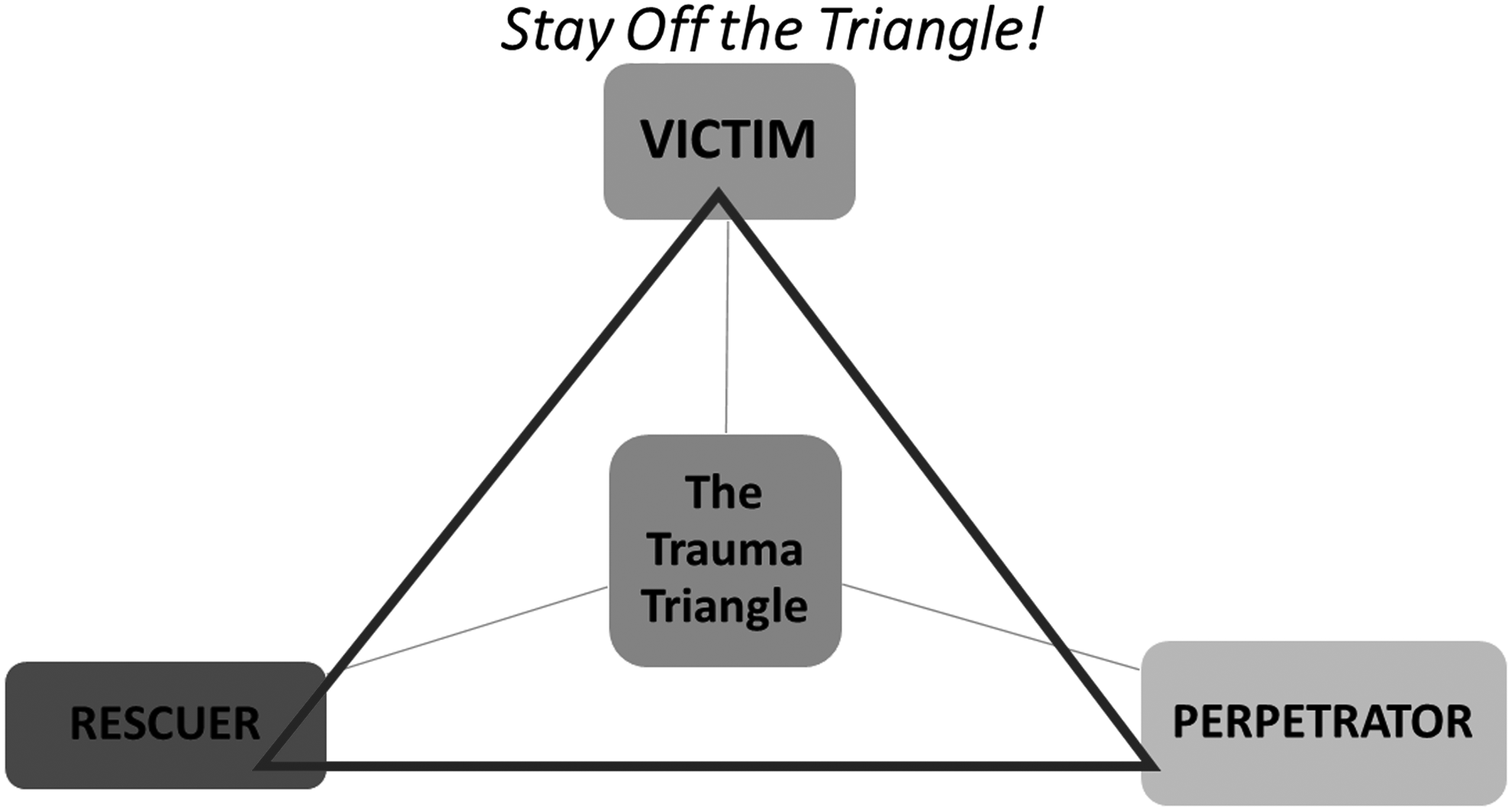
The Trauma Triangle, modified from S. Bloom.
People who are traumatized “live on the triangle,” which is not a healthy place. Additionally, anyone who engages in any role of the triangle must invariably also play out all other roles. This too is unhealthy. It is very alluring to “jump on the triangle” but it is not useful.
To provide an example of the Trauma Triangle and how it may work, imagine a patient coming to see me, a clinician. She states that she is anxious and desperately needs help. So I respond, “I will help you. I will be your rescuer.” Now I ask you, who doesn't go into healthcare who isn't altruistic and wants to help? But here is the challenge. The help that that patient seeks may be from being victimized decades ago. I cannot travel back to when she was nine years old and prevent that bad thing from happening to her.
You can anticipate the outcome. I will fail rescuing her. Her reaction to that failure is that she likely will become angry. She will then lash out against me. So, what am I now? The victim. If I get upset and push back (perpetration), she becomes the victim again and we race across the endpoints of the trauma triangle with no resolution and in an unhealthy way.
In truth, no one can rescue anyone from an event except the person who is traumatized. Now many will be concerned “Does that mean we should be uncaring? Not help?” Caring and empathy are important. But to be effective, we need to develop a professional stance that is helping people help themselves. Not rescuing them. Not fixing them. When you evaluate any behavior change (e.g., smoking or alcohol cessation), you already know that the only person who can make that change is the person themselves. This is true in the case of trauma.
Somewhat related is a term that some authors have referred to is the “cognitive bandwidth of poverty.” 11 The cognitive bandwidth of poverty refers to the external constraints put on sociocognitive abilities as a result of being overtasked with multiple, active worries or concerns.
For example, right now as you sit here, you are, hopefully, not worried about where you are going to sleep tonight, where you are going to get food, or who is taking care of children.
In contrast, imagine a woman who has those worries as she goes to the doctor's office. The energy allocated to those worries narrows her available “bandwidth” of concentration and energy as she is hearing about complex issue (e.g., “here is the prednisone taper dose you need for your child. Each day's dose is different.”).
It should come as no surprise that much of what is said at this visit does not “land” and is not heard. The distraction makes accurate and complete information transfer difficult. So as we counsel patients, it is useful to assess the cognitive bandwidth of our listeners. Parsing our message to effectively be conveyed, keeping in mind this bandwidth of poverty, is a useful skill.
So let's shift gears to focus on attitudes and behaviors and knowledge, and how they contribute to barriers in breastfeeding behaviors. Lack of knowledge and perception of childhood development and a woman's body can impede breastfeeding efforts. There are many members in the community who feel that babies are just “little people.”
So imagine a picture of a toddler dressed in a business suit. If a toddler is actually a young man—not a child, how can you attach him to your breast? Isn't that a bit “creepy”? So, if I hold these beliefs—the infant is a man, although a little one, I am unlikely to engage in breastfeeding. This attitude of children as “little adults” is often seen by pediatricians who have treated newborn infants. For example, the mother may say, “I think that baby just gave me the finger!” When informed that that is not true, is an erroneous attribution, and that the infant is just moving his fingers, the mother may remain unconvinced. Health education can help patient understanding that babies are not little people.
Perception about how best to raise a child can also impede in breastfeeding adoption. In some communities, there is a concern that breastfeeding will “make them soft.” Breastfeeding is perceived as coddling. With all the challenges of the world, many mothers view it as a “tough world out there” and want to avoid “making them soft.” So breastfeeding is out of the question. Consider too, how you might need to frame the discussion of bonding, attachment, and intimacy as it supports developing a strong, healthy man?
Fathers' attitudes about breastfeeding impact behavior. Some men express to their partners that her breasts belong to him, not the baby. The father does not want to share and discourages breastfeeding.
In addition to attitudes, health knowledge can influence breastfeeding behavior. So consider a vagina, what is it and what does it do? If a vagina is exclusively something to put a penis or a digit into, then normal functions of healthy menstruation are viewed as abhorrent or “gross.” What are breasts for? If breasts exist exclusively as sexual objects, then breasts as an anatomic feature for nurturance would be rejected.
The lack of health knowledge is readily evident for those who work with teens. Some sexually active girls when asked by their pediatricians, “Are the boys wearing condoms?” responded, “I do not know what he is doing down there.”
The absence of health information knowledge is a bit mind boggling when we consider that it was the 1970s when women were encouraged to get to know and understand their bodies. Back then, college campuses hosted parties that helped young women use mirrors to locate and see their cervixes. Yet today, we work with incarcerated women who have no idea about any aspect of female anatomy, pregnancy, or health changes in pregnancy even after having given birth to five children.
Regrettably, the lack of health education in public schools and abstinence-only initiatives has contributed to poor health literacy about sexuality. In the Philadelphia schools, if lucky, you might get four weeks that address health. And of those weeks, there is no guarantee that sexual health is covered. It is important to recognize that the lack of health literacy is not limited to women in poverty.
We worked with talented domestic violence counselors on a sexual health project. These women were bachelor's and master's level trained professionals. As we discussed contraceptive options such as the female condom, one woman's question highlighted that the audience was unaware of basic female anatomy. Specifically, what orifices existed in the perineum: Where were they, how many are there, and what was their function? Although a recent episode of the show Orange Is the New Black comedically portrayed the confusion of pelvic anatomy, this lack of knowledge may be more prevalent than most think. This audience did not comprise vulnerable, educational disadvantaged women. Rather they were middle-income ladies.
If we fail at college and master's level, what chance do we have to those with lesser educational opportunities? We have lost significant ground from the level of awareness in the Our Body Ourselves era. Or perhaps we failed to make significant inroads in communities of color all along.
Attitudes about competence can impact the likelihood a woman choosing breastfeeding. Imagine a stressed woman who has to cope with feeling incompetent about trying to breast feed. How can she handle this? How does she handle functioning with no or limited sleep? Or if breastfeeding is natural, how come it is not easy to do or is not working? Many women have to balance competing demands. Remember, I mentioned that a traumatized person may have a limited capacity to handle one more loss. Is this feeling of incompetence one loss too many? How can we work with women to help them help themselves and deal with potential challenges of breastfeeding?
When we evaluate the influence of social norms, it is useful to assess the messages portrayed by social media. If you search the term breastfeeding in a popular browser, you will find about 300 images, as I did. Within these are only three images of African Americans—one very, very light skinned.
All the rest are white. Curiously, there is one image of a man. He is not breastfeeding, but the search result included his picture. Images serve a purpose of presenting visualization that something is possible. If she looks like me, then I can, for example, be a judge, be a scientist, or breast feed my infant.
If I search for pictures that represent realistic ethnic images that promote healthy social norms about breastfeeding, can I find them? I did just that. I searched for images of African American and breastfeeding using the terms black women and breastfeeding. What I found were lots of black women in Africa. Mostly indigenous women.
What message does this portray? It is very interesting in terms of media messages and social norms. My interpretation, solely based on the images I found, was that breastfeeding was something white women did and that black women who did so only did so in developing countries. Not the message we want to convey.
The other thing I learned in terms of browser search is that there is a message that apparently women with infants and toddlers at the same time don't exist—at least there are very, very few pictures of them.
The Internet search of “mother with children” had limited results with only a few women who had, at most, only one other child. In those images, the child is angelic and usually kissing the forehead of the infant. Two other pictures revealed two toddlers who appear to be delightful. They are sitting on the ground and playing and entertaining themselves or reading books. None of them is throwing cereal and running about. None resembles real life.
Perhaps these images were supposed to portray still life. It certainly doesn't reflect real life. And not the real life of competing demands. We have but two arms. How does a single mother feed active toddlers and balance breastfeeding?
I mentioned that social norms are reinforced by what you see on the Internet. But communities also set and reinforce social norms. The biggest predictor of teen pregnancy, of circumcision, and of breastfeeding is if the mom was a teen and pregnant, if the father was circumcised, and if other people in your family have breastfed. 12
So for some of our patients, have they ever seen someone breast feed? And if they have not, do they have the resilience and support to be the trailblazer? In terms of other social pressures, think about when you last got your coffee at Starbuck's. Can that Barista take a moment if she needs to breast feed or pump? Can she really? Or if she “leaks” at work will her coworkers support her instead of snickering or making unkind remarks? Will this event be sexualized by them? Can she handle these comments and not feel mortified if this happens?
Other media messages promote formula usage over breastfeeding. I came across an advertisement for baby formula. It says “We have learned from the breast.” All the formula advertisements show healthy babies. Is that not what all mothers want? Don't women deserve that? To the uninformed, if formula was not better, why would we provide it from WIC? Formula does not change based on what a mother eats. And if she eats poorly, it will not affect the baby's nutrition. So it should come as no surprise that women, bombarded by messages that promote formula use, end up discouraged about breastfeeding as a viable option.
Another factor that may limit women breastfeeding is their reactions to being “good” during pregnancy. Women often avoid unhealthy behaviors such as drinking alcohol or using illicit substances. Many feel that these behaviors are difficult to maintain for nine months. They may also feel a sense of deprivation and impatience to resume their prepregnancy behavior as soon as they deliver and breastfeeding would delay that.
Women's childcare systems and “buy in” from those who help her coparent can impact whether breastfeeding happens. If a woman has limited childcare options or coparenting negotiation skill abilities, she may have to forego breastfeeding if parents or other support people block her efforts. To intervene, we need to assess what skills our patients bring, what they need, and how we need to identify and train everybody involved.
Convenience plays a role in the breastfeeding decision. I found this interesting study done with undergraduate students who were nutrition majors. 13 Students shared their breastfeeding attitudes related to convenience, nutrition, protection, economic, and father's relationship. Convenience emerged as an important influencing factor. Messages also included “I am a modern woman” if women used formula.
One of our projects, the Philadelphia Ujima™ Collaborative14,15 is a network of individuals and organizations—churches, schools, social service groups who come together to create a community of caring and to create health solutions that promote wellness (Fig. 3). Being able to leverage their interesting and innovative ideas aids in recruiting a community “voice” and in generating effective interventions that are culturally and community appropriate. As a University with a priority of civic engagement, Drexel promotes these efforts.
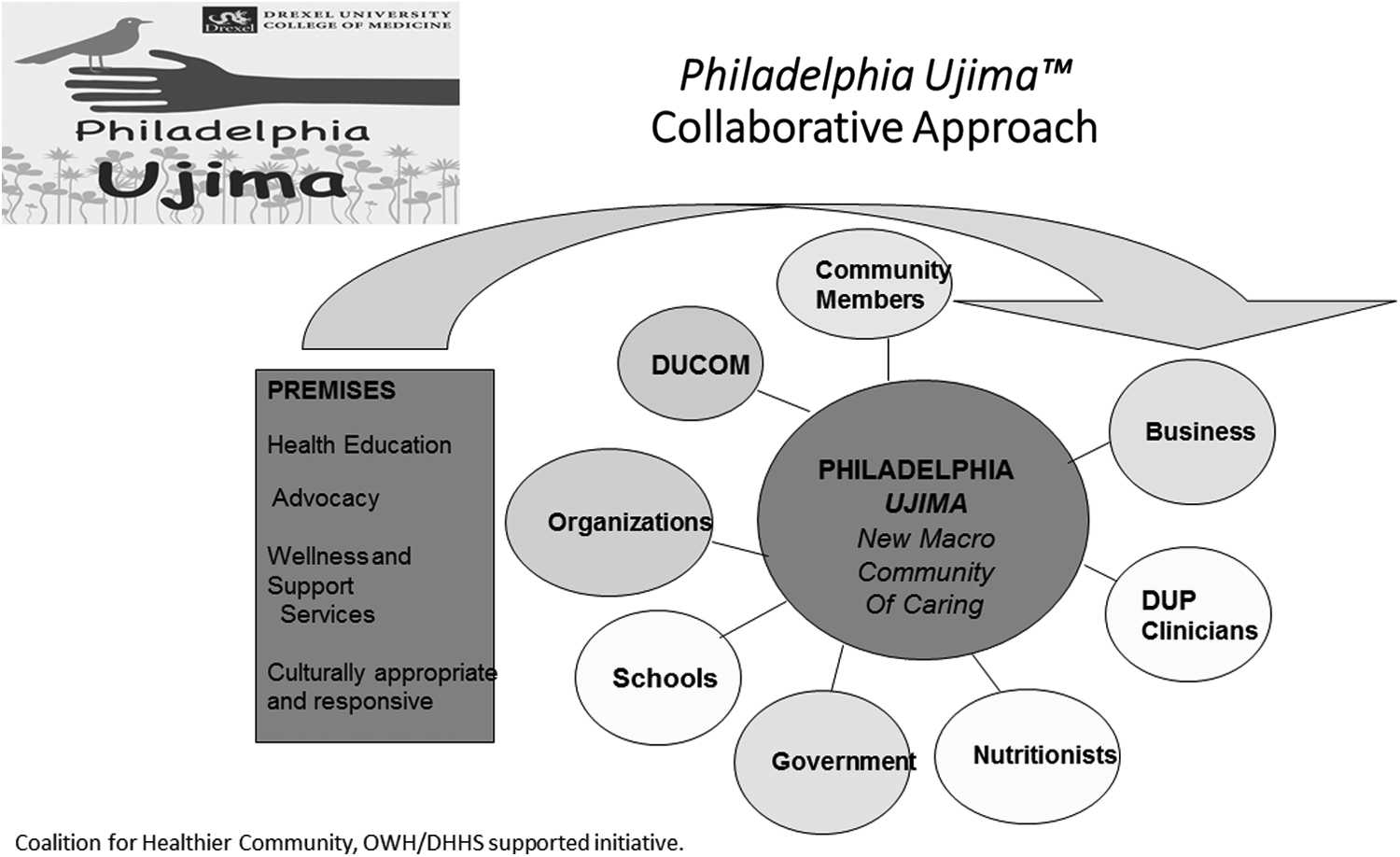
Model used for an innovative community participatory health coalition: The Philadelphia Ujima Project, A. Núñez, Principal Investigator.
Having reviewed the multiple barriers that need to be addressed to promote healthy nutrition for infants, we should ask what can we and should we do about this situation? First, I'll highlight needs for clinicians and medical education, and second, I provide suggestions based upon a socioecological model that spans from the individual to policy considerations.
First, for clinicians, I recommend implementing training so that they can become trauma informed versus trauma reinforcing. These skills will help women help themselves heal from their trauma and then stay off the trauma triangle. As their trauma burden is lessened, these women can have more latitude to select healthier life options. Unattended, imagine how traumatizing it must be to “fail as a woman” because you cannot figure out breastfeeding. Failure does not feel good for anyone, but is worse so for these women.
Second, health centers need to hire culturally similar community aides, medical assistants to aid in brokerage of local norms and medical norms. Training and education of these personnel and mothers about what to expect in normal pediatric development can disrupt the attitudes that children are little adults. It can also disrupt misattributions about behavior and increase healthier mother–infant relationships.
Education needs to also include frank discussions of oversexualization of breasts and family/couple attitudes as well as the usual mother and child benefits of short- and long-term breastfeeding.
Once barriers are identified, motivational interviewing can be used to develop inroads. The “Teach Back” approach that asks the listener to repeat back what they heard of the message is also a valuable tool to assess how well the message was received. This is particularly useful to uncover limitations in cognitive bandwidth that we've already discussed. These educational issues are best initiated early and when reproduction is not eminent.
Bundled with preconceptual counseling or even a quick visit for contraceptive renewal can start and reinforce planning for the baby she plans for in the future.
By reframing breasts as an important body part related to health, not just something for sexuality, and including breastfeeding as part of a holistic reproductive healthcare, women can learn about how wondrous the body is and how they can help themselves and their infants.
From a medical education perspective, many medical schools are engaging in curriculum reform efforts. That is very exciting because where there is change there is opportunity.
Current medical education instructional tools include using simulations, virtual simulations in terms of interviewing people on the phone, standardized patients, the “flipped” classroom, experiential and longitudinal learner exposures, team-based professional education, group run community health education, electronic medical records (EMRs), and patient education portals.
All of these modalities, techniques, and interventions can be mobilized to promote breastfeeding. Imagine an EMR checklist prompt that helps including infant nutrition at a routine examination? Two examples of how to enrich the educational opportunity for students include one in protein biochemistry and another longitudinal scholarship. At Drexel Med, we had a wonderful protein biochemist who lectured on nutrition—including the nutrition in mother's milk.
When initially presented, the students rated it poorly “another biochem lecture.” We collaborated with him and came up with the idea of bringing a nursing mother to the session. Student then heard about the science and met a lactating mother to see the impact of the knowledge. The revised lecture became one of our most popular lectures.
The second example comes from our Sex and Gender/women's health scholar track. To achieve a designation of Sex/Gender Scholar, a student must complete four requirements. First, they complete core course work. Second, they perform service leadership in a community setting. Third, they create health education material to demonstrate their skills at cultural and linguistic effectiveness. Finally, they generate a scholarly project. Students have four years to complete their work.
At Drexel Med, one of our scholars created a new student health navigation program for expecting and new mothers called Moms and Baby Dragons. 16 Our student scholar developed and evaluated the program. Other students developed and evaluated the student navigator curriculum. Student health navigators follow the mothers longitudinally—from pregnancy to postpartum and beyond.
These are just two opportunities but there are many more that educators can create to engage health professional students as they educate them about the benefits of breastfeeding.
But are knowledge, behavior, and education the correct “push or pull points” to create change? (Fig. 4). All areas mentioned thus far can help, but we should not forget or take off of our “to-do” list, a coordinated approach to addressing root causes. If we only treat symptoms and not causes, we will not end up with meaningful change. By a root cause I mean collaborating on advocacy to address concentrated poverty which runs ‘hand in hand’ with unhealthy communities. Poverty is a health hazard. Imagine the impact if all women's health professionals rallied to promote policy changes for unhealthy zip codes? For substantive change in the income gap and therefore the health gap, this is certainly an area that we need to pull together so that we can make a difference.17–19

Highlighting potential systematic change using a socio-ecological approach.
Health professional education and policy are important, but we need change from the microscopic to macroscopic scale.
From a sociologic perspective and starting with the individual, we need to (1) help her help herself in terms of potential trauma history, (2) aid her in skills of self-esteem, healthier boundaries, sexual negotiation, and relationships, (3) troubleshoot and intercede in barriers to access, and (4) promote the receipt of quality health education regarding basic women's health and child development.
These interventions will not be effective if “one and done.” They need reinforcement like in school or at the clinical office. They need a longer lead time to solidify efforts that promote behavior change. My big idea about promoting a longer lead time is to create breastfeeding manikins similar to Rescue Annies, manikins we use to teach cardiopulmonary resuscitation.
Imagine if we had a “Lacto-Lakisha,” for example, a manikin that promotes body awareness and health for girls and women while simultaneously normalizing breastfeeding. Lacto-Lakisha could teach girls about how lactation and nutrition “work” and even how to troubleshoot problems with latching.
From the children and youths' perspectives, the manikin is likely to be viewed as engaging and enjoyable. By providing this simulation “playing” with Lacto-Lakisha, if you will, girls can try out breastfeeding well before it is a choice they need to make.
From the interpersonal perspective and from the partner, family, or social support, women need augmented economic support. If she is to work, she may need authorization for two pumps, one at work and one at home.
Compare what we do with what occurs to most European mothers. Many have a caregiver in their home after they deliver to provide physical support. These countries value children and women. Are there ways we can identify mothers at highest need and provide enhanced support? There are high-caliber, new mother in-home visitation programs that our Ujima partners provide. Perhaps expansion of these programs can make a difference. It is often quoted that it takes a village to raise a child. Doesn't it take that same village to aid a mother? How can we create, support, and maintain that village if there isn't one? What do we do and should we do?
From an organizational perspective, Sanctuary-certified training programs exist and exploring certification could help in creating more and safer environments. Having organizations consider how responsive they are to the communities they serve by evaluating their workforce. Are there culturally and community congruent team members there as clinicians, educators, and aides? Organizations can also help by creating and maintaining online or telephone-based support counselors. Supplemented with phone cards with free minutes women can have greater access. Perhaps sites could develop an avatar that functions as a coach to aid in breastfeeding (and health) questions.
From a community perspective, celebrity endorsements, enriching media messages and images can be helpful. Beyoncé endorsed breastfeeding and she should be applauded for that. Yet, there is no image attached to that endorsement, only a picture of her holding her infant.
Celebrity men can play a role promoting male and female attitudes toward healthy infant nutrition. The power of media such as Twitter reaches many people. So recruiting celebrities impacts social norms and future behaviors.
One example that may be useful to replicate is how HIV behavior was impacted by television programming. Writers worked with BET producers to incorporate story lines about HIV—risk, testing, treating. In the resultant shows, barbers told men to “get a grip and get tested.” Actors played men who said “I'm getting tested—that's what I'm going to do.” Another tried to discourage him “You are good guy, you don't need to do that.” He responds “Yeah I do.”
In the show, women who treated others poorly for having HIV were viewed as being abhorrent. Beyond the story line and drama, investigators found higher rates of testing of those who viewed the show compared to those who did not. Imagine infusing normal health, pregnancy, lactation, and breastfeeding as part of a similar show.
Whether it is Oprah, BET, Beyoncé, or creating courses for writers, ideas for story lines that show healthy nutrition for infants need to shared, incorporated, and produced. We also need some music videos to include images of breastfeeding that is not sexualized. Promoting events such as black breastfeeding week is helpful. Finally, we need to identify strategies to augment social media images. What is the best way to yield image results that look like real and diverse people and not stereotypes?
From the policy perspective, I've addressed some of these areas already. Attitudes and behaviors are important but we may need resources if we are going to raise levels of breastfeeding.
What if women in the United States could stay home for three months after delivery? When we have discussions about a living wage, what are the wages of mothers who are performing the integral tasks of raising her children? The invisibility of this effort and insufficient advocacy are areas of needed attention.
Additional policy considerations might be to have an OSHA requirement, similar to those for defibrillators, that workplaces are required to have onsite pump stations for reproductive-aged women. This policy would need resources to ensure auditing and compliance occurs. Auditing and compliance measures are also needed regarding flexible breaks for nursing mothers. Despite a provision of Obamacare, aid for mothers in the workplace is still insufficient. 20
So in summary, breastfeeding helps the health of mothers and children. Trauma is a potent variable for which we need more training and vigilance.
Barrier identification should occur at every level—individual, interpersonal, community, policy, and for clinicians as well as patients. Resources are needed for pilot projects that explore root-cause solutions and advocate for change. Systemic and foundational issues such as wealth disparity, poverty, and the collective concentration in unhealthy communities need rigorous attention to intercede. We need to provide real-life experiences in training for trainees, children, and our patients.
Finally, we should thoughtfully increase the integration and collaborations of practices that support breastfeeding. To reverse the course on health disparities, we need good intention and coordinated intentional action. Change, little or small, can make a difference.
Footnotes
Disclosure Statement
No competing financial interests exist.