
Abstract
Abstract
Objective:
The aim of this randomized controlled experimental study was to evaluate the effect of breastfeeding on the pain of babies during vaccination.
Materials and Methods:
The sample of the study consisted of 100 babies who complied with the sampling criteria between July and November 2012. The babies breastfed from their mothers 5 minutes before, during, and after the vaccine injections. The Neonatal Infant Pain Scale (NIPS), duration of crying, heart rate, and oxygen saturation were evaluated before, during, and after the vaccine injections. Data were evaluated by descriptive statistics, chi-square, Cronbach's alpha consistency coefficient, independent sample t-test, and Mann–Whitney U test.
Results:
The babies in the control group experienced severe pain and the babies in the breastfeeding group felt moderate pain during the vaccine injections (p < 0.05). The NIPS score of the babies in the breastfeeding group was lower than the control group during the vaccine injections. The breastfeeding group spent less time crying, and had lower heart rates and higher oxygen saturation values during vaccine injections
Conclusion:
Breastfeeding prevented increased heart rates, duration of crying, NIPS, falling oxygen saturation, and reduced pain during the invasive procedures in newborns more than control group.
Introduction
R
Vaccination pain causes increased stress for babies and parents, sensitivity toward pain during the next vaccination, and has an influence on the mother–infant relationship. Various studies have shown that vaccination applied to babies in a short space of time causes intensive stress.5,6 Considering the fact that vaccination is the first pain experience of healthy babies, pain management is of great importance. If babies experience more than one pain associated with vaccinations on the first occasion, they become more sensitive to the next vaccination and feel a greater pain. 7
A recent systematic review 8 showed that breastfeeding consistently reduced behavioral responses of cry duration and composite pain scores during and following vaccinations compared to no treatment, oral water, oral dextrose, maternal cuddling, massage, vapocoolant spray, and topical anesthetic (EMLA). Even though the literature involves studies indicating that breastfeeding is effective in reducing pain associated with routine vaccinations in infants,9,10 there is no study indicating that it is effective in reducing the pain associated with two different vaccinations applied in babies.
The aim of this randomized controlled experimental study was to evaluate the effect of breastfeeding on reducing babies' acute pain due to two different vaccinations.
The hypothesis of the study
H1- During the second month of vaccines administered sequentially to two different body sites, breastfed babies will feel less pain than not-breastfed babies.
Materials and Methods
This comparative, randomized controlled study involved 100 babies who came for routine vaccinations to the Vali Saim Çotur Family Health Centre between July and November 2012, who complied with the sampling criteria. The sample of the study was the babies who came for the routine vaccination application within the study period and who met the following criteria. Research sample includes 100 babies, 50 for the breastfeeding group and 50 for the control group. Babies were selected for the groups randomly from an opaque envelope (Fig. 1).

Flow diagram for this randomized controlled trial of breastfeeding on the pain of babies during vaccination.
Sampling criteria for babies
The study included babies whose gestational ages were between 38 and 42 weeks, whose birth weights were 2,500 g or more, who were fed at least half an hour before the procedure, whose mothers' agreed to breastfeed the infant during and after the procedure, and who had not received any pharmacological or nonpharmacological treatments.
The newborns' pain severity was evaluated using the Neonatal Infant Pain Scale (NIPS) developed by Lawrence 1993. 11 Oxygen saturation and heart rate were measured using a pulse oximeter device. The crying times of babies were recorded using a video recorder (Sony DSC-HC 21) before, during, and after the vaccinations. The NIPS measures six behavioral responses, facial expression, crying, manner of respiration, arms, legs, and wakefulness, to evaluate the pain of newborns. While crying is scored with three points (0-1-2), other behaviors are scored with only two points (0–1). The highest and lowest possible scores on the NIPS are 7 and 0, respectively. Scores between 0 and 2 are considered to be pain free. Scores of 3 and 4 indicate moderate pain, and scores over 4, severe pain. 11 The general pain status was evaluated before the vaccine applications using this scale, and changes during and after the procedure were observed.
Written consent was obtained from the Akdeniz University Non-Invasive Clinical Trials Ethics Committee (decision number 254 and dated 27.06.2011), from the hospital where the study was conducted and from the parents.
Data collection
Breastfeeding group: Before the procedure, the breastfeeding position recommended by the World Health Organization for mothers was given to babies (baby's head and body are in a straight line; the baby is facing the breast; the baby's nose is opposite her nipple; hold the baby's body close to her body; the baby's whole body, not just the neck and shoulders). 12 Vaccination was started after the mothers breastfed their babies for 5 minutes before the procedure. The baby was ensured to be breastfed from the same breast and at the same position without a break during and after the first vaccination and during and after the second vaccination. Consequently, any change was not made concerning the breastfeeding position of the baby. The nurse, who administered the vaccination, placed herself in the appropriate position when administering both vaccines. Both legs of the baby were held by the other nurse without applying pressure during vaccination to administer properly vaccine to the right location. The babies were ensured to breastfed for more 5 minutes after administering the last vaccination. In the control group, injections were administered with no pain control intervention. The recording process was sustained until the end of the 5th minute after the procedure. The mothers were allowed to hold, talk, or rock the baby after the procedure in both groups.
All the babies received the intervention from one nurse only; a nurse would then come into the immunization room. The nurse administered 0.5 mL of wDPT vaccine by a 2-mL syringe with a 23G 1” needle on the anterolateral aspect of the thigh (left) and 0.5 mL of conjugated pneumococcal vaccine by a 2-mL syringe with a 23G 1” needle on the anterolateral aspect of the thigh (right) to the vastus lateralis muscle of the left and right legs via intramuscular after cleaning the skin with spirit. The injections were given with the baby in the mother's lap, with thigh exposed, and the nurse called aloud “in” when the needles were inserted and “out” when the needles were removed. All events were recorded by the investigator on a digital video camera (model Sony DSC-HC 21) for a total duration of 5 minutes from the removal of the needles. Two investigators analyzed the cry durations and NIPS scores of babies in both groups using the video records after the completion of the application. Because NIPS is a data collection tool based on observation, we videotaped. It is then evaluated by two researchers. A separate recording device is not used for crying time.
A pilot test was carried out with five newborns from each group, to assess the appropriateness and usefulness of the data collection tools. The newborns involved in the pilot test were excluded from the study.
Data analysis
Data were analyzed using the Statistical Package for the Social Science Program, SPSS (20.0) for Windows software. Continuous values are expressed in terms of mean ± standard deviation. Frequencies, means, standard deviations, and percentages were calculated. Between-group comparisons used the independent samples t-test and the Mann–Whitney U test. The significance level was set at p < .05.
Results
The postnatal age, gestational age, birth weight, and birth length were comparable in both groups (Table 1). The mean duration of crying was significantly lower in the breastfeeding group, 20.5 (16.2) seconds, compared to babies in the control group, 45.1 (14.5) seconds (z = 6.52, p < 0.05) (Table 2).
SD, standard deviation.
There was a statistically significant difference in the NIPS before, during, and after needle insertion. Mean NIPS score in the breastfeeding group (0.26 ± 1.03) was significantly lower than in the control group (0.60 ± 1.16) before immunization (z = 2.63, p < 0.05). Mean NIPS score in the breastfeeding group (6.00 ± 1.31) was significantly lower than in the control group (6.64 ± 0.72) during immunization (z = 2.88, p < 0.05). Mean NIPS score in the breastfeeding group (1.86 ± 2.21) was significantly lower than in the control group (6.82 ± 0.75) after immunization (z = 8.71, p < 0.05) (Fig. 2).

Data are mean values. Mann–Whitney tests were performed using a significance of 0.05. NIPS, Neonatal Infant Pain Scale.
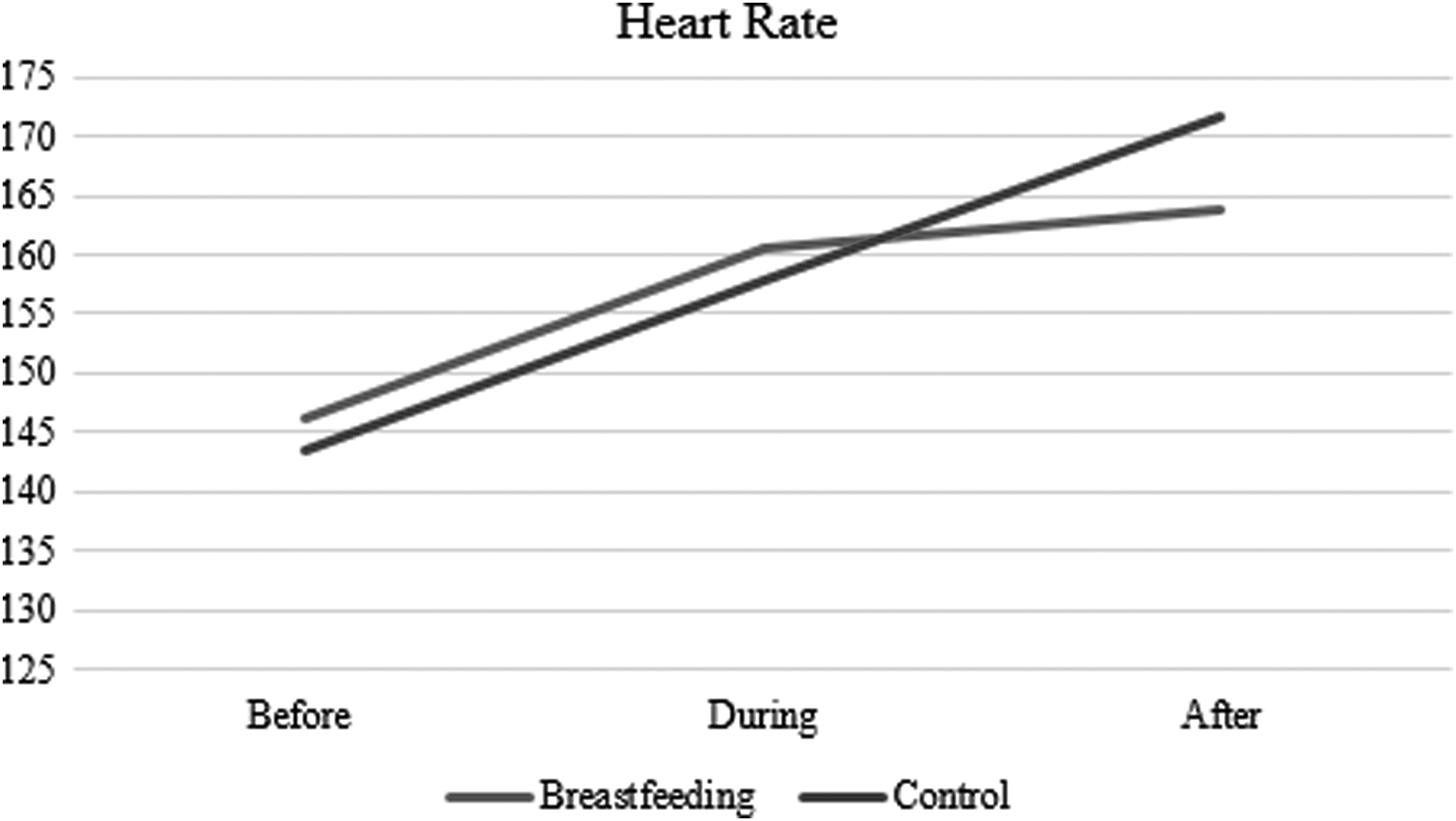
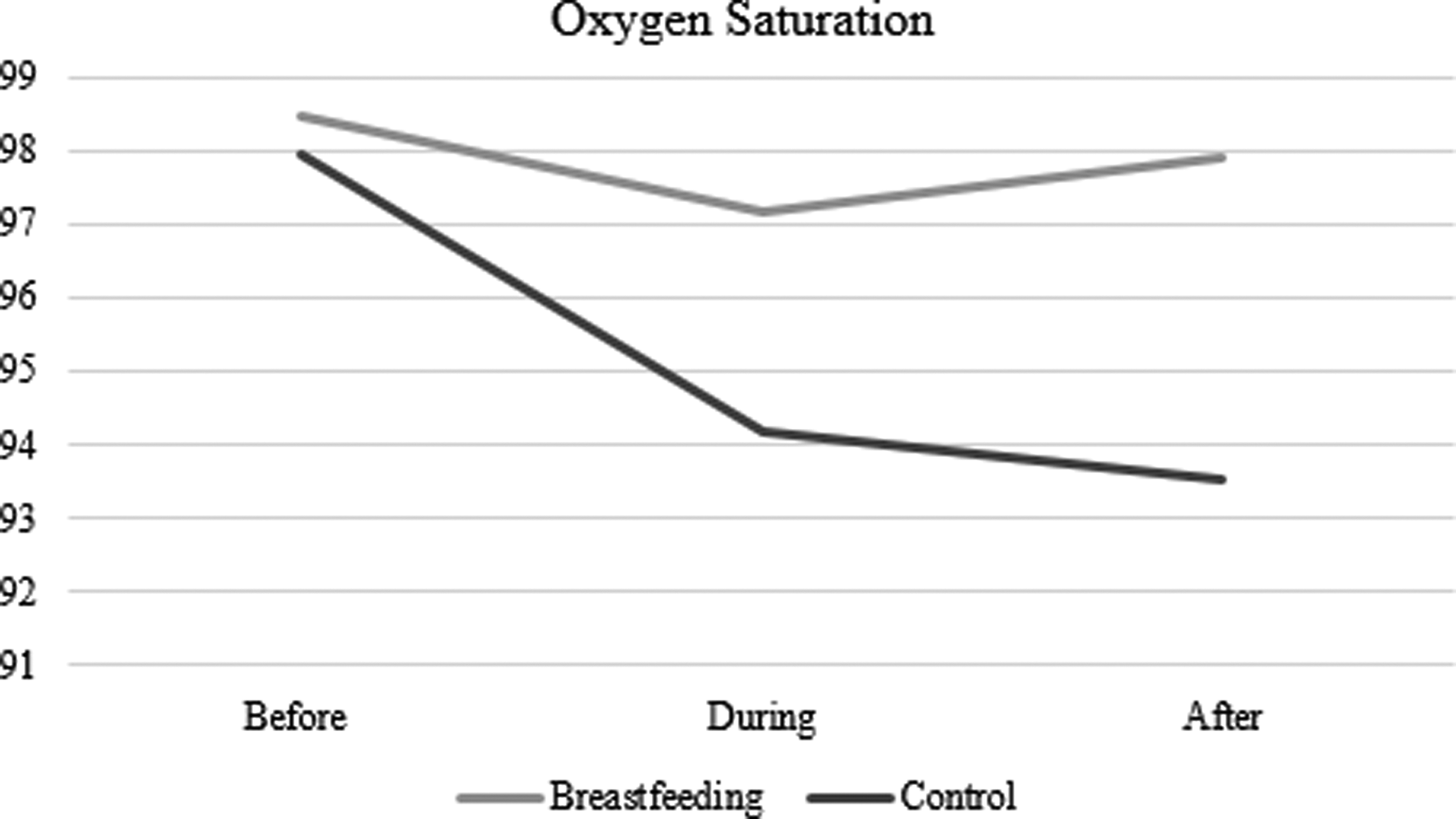
It was determined that the mean heart rate of the breastfeeding group (163.78 ± 16.62) was found to be significantly lower than that of the control group (171.68 ± 14.78) after immunization (z = 2.28, p < 0.05) (Fig. 3). The mean oxygen saturation levels of the breastfeeding group (97.18 ± 3.94) were found to be significantly higher than those of the control group (94.18 ± 12.71) during immunization (z = 2.11, p < 0.05). The mean oxygen saturation levels of the breastfeeding group (97.90 ± 3.08) were found to be significantly higher than the control group (93.52 ± 6.96) after immunization (z = 4.15, p < 0.05) (Fig. 4).
Continuous values are expressed in terms of mean ± standard deviation. Mann–Whitney U test was used in the intergroup comparison. p ≤ 0.05 was accepted as significant in all analyses.
Continuous values are expressed in terms of mean ± standard deviation. Mann–Whitney U test was used in the intergroup comparison. p ≤ 0.05 was accepted as significant in all analyses.
Discussion
Our study demonstrated that babies who were breastfed had a significantly shorter duration of crying, and a lower pain score during and after vaccination, compared to the control group.
Systematic review 8 showed that six studies9,13–17 (547 infants in total) reported cry duration during immunization. It was shown that there was a significant reduction in crying time in seconds in the breastfeeding groups compared to the control groups. Systematic review's results showed parallelism with our study result.
In this study, it was found that the Neonatal Infant Pain Scale (NIPS) was significantly lower in the breastfeeding group compared to the control group. Systematic review 8 showed that five studies15,16,18–20 (n = 310 infants) reported NIPS scores during immunization. It showed that this evidence was of moderate quality as data were primarily from infants younger than 6 months. Systematic review's results shown parallelism with our study result. Recently conducted Cochrane reviews of pain management strategies in the newborn period demonstrated that breastfeeding, as shown in studies by Harrison et al. 8 and Shah et al., 10 sweet solutions of sucrose, as shown in a study by Stevens et al., 21 and glucose, in a study by Bueno, 22 reduced behavioral responses and composite pain scores during painful procedures. In addition, systematic reviews of sweet-tasting solutions beyond the neonatal period up to 1 year of age demonstrated analgesic effects during needle-related painful procedures when compared to water or no treatment.6,23
The breastfeeding method prevented the increase of heart rates and the decrease of oxygen saturation values of babies, which was consistent with the findings of other studies evaluating the heart rate9,24 and oxygen saturation. 25 Results concerning the heart rate in the study showed no parallelism with the results of Bueno et al., 5 because Bueno et al. 5 used small volumes of breast milk and the babies were not breastfeeding. They reported that single doses and small volumes of milk are not effective for neonatal pain relief; however, larger volumes may present better effects, possibly due to the combination of several mechanisms. Results concerning oxygen saturation showed no parallelism with the results of Upadhyay 26 and Efe and Özer. 9 Since changes in the heart and breath rate and blood pressure of neonates during painful procedures also reflect the general stress condition of the body, they are not peculiar to pain. Changes in the heart rate and oxygen saturation of a neonate in pain might be two sided as increases and decreases. 11 Systematic review 8 showed that there was no evidence that breastfeeding had an effect on physiological responses.
Breastfeeding is hypothesized to reduce distress via multiple mechanisms, including physical comfort, sucking, distraction, and ingestion of sweet-tasting and other substances that may have, individually and together, distress-relieving effects. A meta-analysis, including 792 infants, showed a large benefit of breastfeeding during vaccination. 27 The flavor of breast milk is insufficiently sweet on its own for the sweet taste-induced analgesic effects. This is why small volumes of breast milk given via a syringe/bottle are not analgesic. 10 Breastfeeding involves maternal skin-to-skin contact, which stabilizes blood glucose levels, body temperature, and respiratory rate and reduces the release of stress hormones. 25 Finally, breastfeeding involves intimate social interaction between mother and child and may release the antistress hormone, oxytocin. The mechanism of relaxation and analgesia probably works synergistically. 28 Breastfeeding has already been shown to be analgesic during vaccinations, and in addition, there is already evidence of the analgesic effects of sucrose or glucose during infant vaccinations. These strategies are already recommended in high-quality clinical practice guidelines.29,30 A systematic review indicated that sucrose is effective for reducing procedural pain from single events such as heel lance, venipuncture, and intramuscular injection in both preterm and term infants.23,31 In the literature, there is already evidence of the effectiveness of breastfeeding and sweet solutions.
Our study is the first one to demonstrate that breastfeeding is effective in reducing the pain associated with two different vaccinations applied in babies. In our study, the babies were allowed to be breastfed for 5 minutes before, during, and after the vaccination. As a result of our study, a decrease was determined in physiological and behavioral symptoms caused by pain associated with vaccinations in babies in the breastfeeding group.
Accordingly, it could be thought that breastfeeding the babies for 5 minutes before the procedure will be sufficient in terms of duration in our study. In their study, Leite et al. 32 determined that the pain of babies was reduced after being breastfed for 5 minutes before, during, and after the process of having blood taken, which shows a parallelism with our study result.
Recommendations for Practice and Research
There is already sufficient evidence of the analgesic effects of breastfeeding, or sweet solutions. These are already recommended in clinical practice guidelines. Therefore, these strategies should be used. The World Health Organization recommends breastfeeding during infant vaccinations. It is not ethical to expose infants to placebo/no treatment groups due to there being no uncertainty about the analgesic effects of both interventions. Further research should focus on knowledge translation of effective pain management strategies.
It could be recommended to conduct different studies through approaching the breastfeeding durations of babies in terms of different minutes before, during, and after vaccinations.
Conclusion
The findings from this study suggest that breastfeeding is effective in pain reduction in the immunization procedure in babies. It may replace practices with procedures.
Footnotes
Acknowledgments
This study received external funding from the Akdeniz University Scientific Research Project Unit. We are grateful to all the parents who participated in this study.
Disclosure Statement
The authors received no financial support for the research and/or authorship of this article.