
Abstract
Abstract
Background:
Approximately one in five Western women who breastfeed are likely to experience acute mastitis. This study investigated the incidence and risk factors of acute mastitis in a cohort of Iranian women.
Subjects and Methods:
Subjects were 672 participants of the Shiraz Infant Feeding Study conducted between June 2014 and March 2015. Mothers were recruited from the maternity ward and followed up at 1, 3, 4, and 6 months postpartum to obtain information on their breastfeeding practices and experiences. The occurrence of acute mastitis in the first 26 weeks postpartum was self-reported and the occurrence of acute mastitis in the first 4 weeks and between 5 and 12 weeks postpartum was treated as separate outcomes. The risk factors for acute mastitis were explored using multivariable logistic regression analysis.
Results:
In total, 130 mothers (19.3%, 95% confidence interval: 16.3–22.3%) experienced at least one episode of acute mastitis. Having expressed breast milk and use of a pacifier were significantly associated with acute mastitis in both the first 4 weeks and between 5 and 12 weeks postpartum. Persistent problems with cracked or sore nipples, or engorged breasts, and a reduction in breastfeeding were associated with acute mastitis between 5 and 12 weeks.
Conclusions:
The incidence of acute mastitis experienced by this cohort of Iranian women is similar to that reported for women in Western countries. The risk factors of acute mastitis identified in this study are potentially modifiable and could be prevented or ameliorated with adequate support and anticipatory guidance provided in the early postpartum period.
Introduction
L
Studies of women in Western countries suggest that as many as one in five breastfeeding women will suffer at least one episode of acute mastitis in the first 6 months postpartum,5–8 with roughly half of all episodes occurring in the first 4 weeks.5,7,9 Few studies have reported the incidence of mastitis in low- and middle-income countries. A study in China reported that 6.3% of women experienced at least one episode of mastitis in the first 6 months postpartum, with approximately half of the initial episodes occurring in the first 4 weeks postpartum. 10 A recent study from western Nepal reported that 8% of women experienced mastitis in the first month postpartum. 11
In Iran, breastfeeding is a near-universal practice with most women continuing to breastfeed well into the first year and beyond.12,13 To our knowledge, there have been no studies that have reported the incidence of mastitis among women in Iran or any other Middle Eastern country. The purpose of this study therefore is to report the incidence and risk factors of acute mastitis in a cohort of Iranian women and its impact on breastfeeding duration.
Subjects and Methods
The Shiraz Infant Feeding Study (SIFS) is a prospective cohort study conducted between June 2014 and March 2015. In addition to investigating acute mastitis, the focus of this article, SIFS was designed to investigate a variety of infant feeding practices, including the introduction of prelacteal feeds, formula, and solids and the duration since birth of exclusive breastfeeding. Mothers were recruited within 48 hours of giving birth from the maternity wards of three government and two private hospitals in Shiraz, a city in the south west of Iran. Mothers were eligible for inclusion if they were older than 18 years and had delivered a healthy, singleton full-term infant (≥37 weeks) weighing 2,500 g or more. Women were ineligible if they were considered by the nursing or medical staff to be too ill to participate in the study or resided outside of Shiraz.
Participants were followed up at 1, 3, 4, and 6 months postpartum when they attended scheduled appointments at their local Maternal and Child Health (MCH) clinic for routine postnatal maternal and infant care and monitoring. Mothers were interviewed at baseline and follow-up visits by trained research staff using questionnaires adapted from those used in the first and second Perth Infant Feeding studies.14,15 These questionnaires have been adapted and translated into local languages to study infant feeding practices in a number of Islamic countries.16,17 Additional questions related to mastitis were adapted from the Mastitis in Glasgow Study. 5
The study was approved by the Curtin University Human Research Ethics Committee (HR 31/2014) and the Local Research Ethics Committee of Shiraz University of Medical Sciences (209/2014). All mothers provided signed informed consent and were advised that their participation was voluntary and that they could decline to participate or withdraw from the study at any time without prejudice.
Case definition
Acute mastitis cases were identified initially by self-report at each follow-up interview when mothers were asked if they had experienced mastitis since their last interview. The age of their infant at the time they experienced an episode of mastitis was recorded in weeks. Women were questioned further as to whether they had experienced symptoms typically associated with acute mastitis. While there is no standard definition of mastitis, 7 these symptoms were used to verify the mother's self-report of mastitis. For statistical analysis, a woman was defined as an acute mastitis case if she reported having had a red, tender, hot, or swollen area on any part of her breast, accompanied by one or more of the following: (1) an elevated temperature (either estimated or measured as being ≥38°C) or (2) one or more of the constitutional symptoms of fever (body aches, headaches, and chills).
As the majority of episodes of mastitis reportedly occur in the first 4 weeks postpartum5,7,9,10 and less frequently after 3 months postpartum, we chose to focus our analysis on cases occurring in the first 3 months. The occurrence of acute mastitis in the first 4 weeks postpartum and between 5 and 12 weeks postpartum was treated as separate outcomes to determine if the risk factors differed according to stage of lactation.
Explanatory variables
Variables examined in this study as potential determinants of acute mastitis were derived from the literature6–8,18 and included parity and method of delivery collected at baseline. Women were asked at follow-up visits if in the intervening period they had experienced any of a list of common breastfeeding problems (including cracked nipples, attachment difficulties, pain on nursing, and engorged breasts) and whether they had worn a nursing bra, given their infant a pacifier, expressed their milk, or changed the level of breastfeeding (i.e., introduced complementary formula).
Sample size calculation
Assuming the any breastfeeding rate at 6 months to be 60%, with a confidence precision percentage of 0.04, power of 0.8, a sample of 576 mothers would give a 95% confidence interval (CI) of 56–64%. A target sample of 700 mothers allowed for an 18% dropout rate and women were recruited consecutively until the target sample was achieved. Recent studies have reported mastitis incidences from as low as 6% in Chinese women 10 up to 18% in Scottish women. 5 To our knowledge, there is no information about the incidence rate of mastitis among Iranian women, and the mid-point of the range, 12%, was used as the rate for the sample size calculation. With a precision percentage of 0.04, power of 0.8, a sample of 254 mothers would give a 95% CI of 8–16%. Thus, this study which used 672 of the 700 participants recruited into SIFS was amply powered.
Statistical analyses
The acute mastitis incidence density was calculated by dividing the number of episodes of acute mastitis in 4-week blocks by the number of completed weeks of breastfeeding. 7 The potential risk factors associated with acute mastitis occurring in the first 4 weeks postpartum and between 5 and 12 weeks postpartum were explored as separate outcomes first using bivariate logistic regression. All explanatory variables were entered into a multivariable logistic regression model to identify those variables independently associated with the risk of acute mastitis during each time interval with a forward stepwise selection method. Results are presented as crude and adjusted odds ratios with 95% CI. Kaplan–Meier survival analysis was used to investigate the association of acute mastitis and breastfeeding duration and the log-rank test was used to compare the difference between groups. A p < 0.05 was considered as statistically significant.
The small number of cases introduced a small case bias 19 and caused a computational problem statistically with maximum likelihood estimation used in the logistic regression analysis, resulting in a wide 95% CI. The bias is stronger particularly when the number of cases in the less frequent category of a variable (e.g., the occurrence of various breastfeeding-related problems between 5 and 12 weeks) is small. In current literature related to statistical computation methodology, among others, the Firth method 20 provides a possible remedy for reducing the small case bias, hence narrowing the corresponding 95% CI, and was used in this study in both univariate and multivariable logistic regression analyses.
Logistic regression analyses with the Firth method were conducted using Stata package version 14.1 (StataCorp LP, College Station, TX). The other analyses were conducted using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp. Released 2013; IBM Corp., Armonk, NY).
Results
In total, 1,571 women were approached and, of these, 852 failed to meet 1 or more of the inclusion criteria and 19 declined to participate (Supplementary Fig. S1). Of the 700 women who agreed to participate in the SIFS, 672 attended the first month follow-up visit (96.0% retention). The majority of participants were 25 years or older (78.6%), primiparous (54.6%), had received a high school or university education (80.3%), and delivered by cesarean section (70.8%) (Table 1). Overall, 130 mothers (19.3%, 95% CI: 16.3–22.3%) had experienced at least one episode of acute mastitis in the first 26 weeks postpartum. A total of 136 episodes of acute mastitis were reported, with 124 mothers (95.4%) reporting a single episode and only 6 mothers (4.6%) reporting two episodes. In the first 4 weeks, 72 women (10.7%) experienced acute mastitis, representing more than one half (55.4%) of the first episodes, and the incidence fell sharply thereafter (Fig. 1). The incidence density was highest in the first 4 weeks (27.3 episodes/number of women breastfeeding weeks × 1,000) and approximately half of this (12.2 episodes/number of women breastfeeding-weeks × 1,000) in the second 4 weeks postpartum (Table 2). All cases reported symptomatology consistent with the case definition of acute mastitis used in this study, including moderate to severe breast skin tenderness (100.0%), skin redness (83.1%), and/or warmth (91.4%), in combination with an elevated temperature (92.1%) and/or flu-like symptoms (80.2%). All cases were prescribed antibiotics by a medical practitioner.
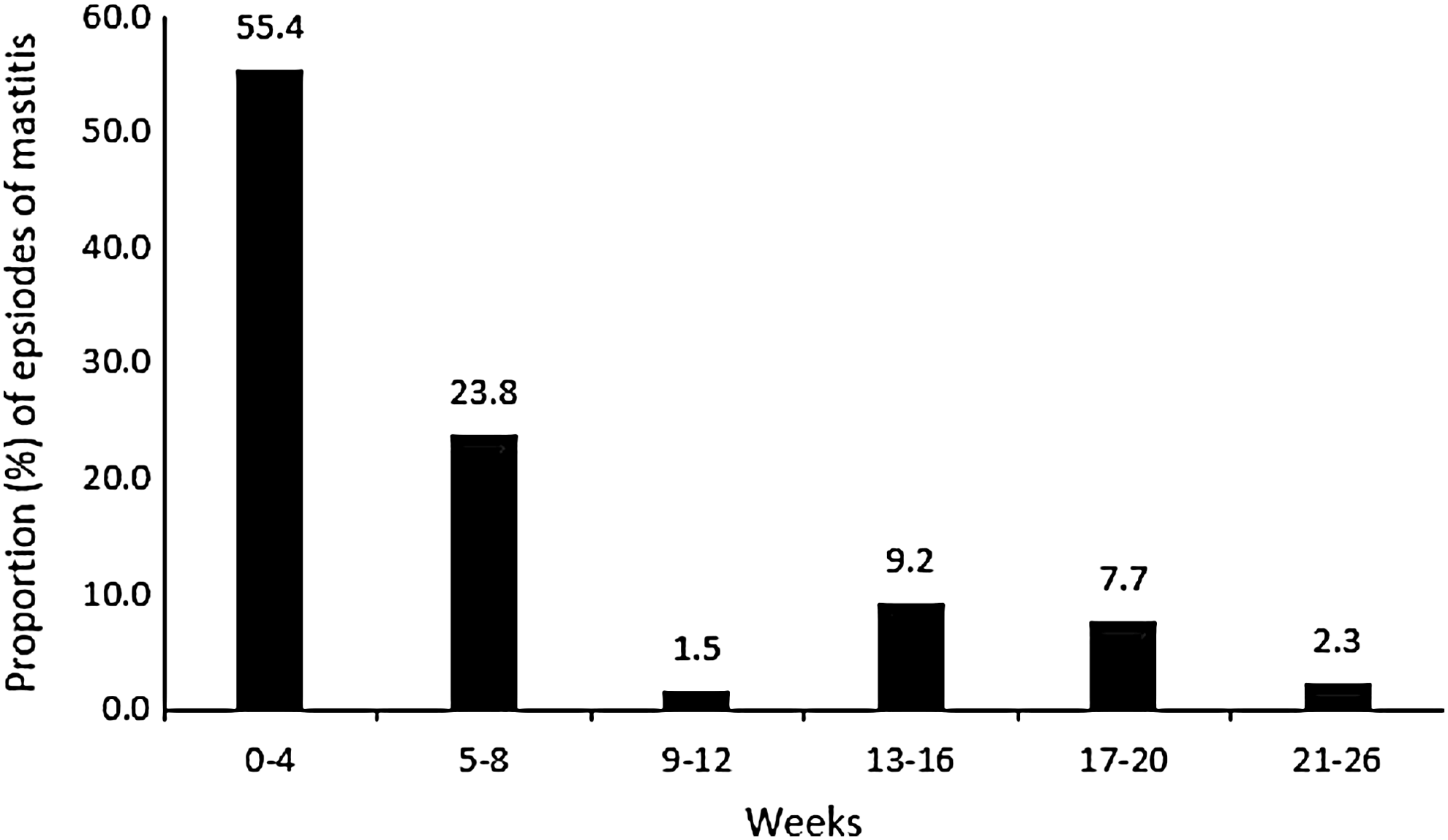
Proportion (%) of first episode of mastitis occurring in each time period (n = 130).
Amir et al. 7
Tang et al. 10
Acute mastitis and breastfeeding duration
In total, 579 (86.2%) of women were still breastfeeding at the 6-month follow-up visit, and there was no association between occurrence of acute mastitis and duration of breastfeeding with 87.0% of cases and 85.0% of noncases still breastfeeding at 26 weeks (log-rank test χ2 = 0.289, df = 1, p = 0.591).
Factors associated with acute mastitis
Relatively few mothers reported mastitis at the 4- (n = 18) and 6-month follow-up interviews (n = 11), thus potential risk factors were investigated only for mastitis reported at the 1-month (n = 72) and 3-month (n = 35) interviews. Based on the bivariate logistic regression analysis, the common risk factors associated with developing acute mastitis in both time intervals included experiencing cracked nipples, engorged breasts, wearing a nursing bra, expressing milk, and giving their infant a pacifier. In addition, women who continued to experience pain with nursing and problems with positioning beyond 4 weeks and those who had decreased their level of breastfeeding were at greater risk of experiencing acute mastitis between 5 and 12 weeks postpartum (Table 3).
Obtained by Penalized Maximum Likelihood Estimation as proposed by Firth. 20
CI, confidence interval; COR, crude odds ratio.
The results of the multivariable analysis are shown in Table 4, and mothers who were multiparous, had engorged breasts, expressed their breast milk, and given their infant a pacifier were at greater risk of acute mastitis in the first 4 weeks and between 5 and 12 weeks postpartum. However, experiencing pain during nursing, having damaged nipples, and wearing a nursing bra were found only to be independently associated with experiencing acute mastitis between 5 and 12 weeks. Mothers who had decreased the level of breastfeeding were at lower risk of acute mastitis in the first 4 weeks, but at greater risk of acute mastitis between 5 and 12 weeks.
Adjusted for all variables in the table in addition to the method of delivery.
Obtained by Penalized Maximum Likelihood Estimation as proposed Firth. 20
AOR, adjusted odds ratio; CI, confidence interval.
Discussion
This is the first study to report the incidence of acute mastitis in Iran or any other Middle Eastern country. Roughly one in five women experienced an episode of acute mastitis in the first 26 weeks postpartum. The overall incidence reported in this study is comparable with incidence rates over the same follow-up period reported for Western countries such as Scotland 5 and Australia.6,7 In a recent study conducted in Nepal, an 8% incidence of mastitis during the first month postpartum was reported, 11 which is comparable with a first month incidence in this study of 10.7% (72/672) and 9.5% in Scotland. 5 This is one of few studies to report acute mastitis incidence density in 4 weekly blocks, which allows for direct comparison between studies. The incidence density in this study of 27.3 episodes/number of women breastfeeding weeks × 1,000 in the first 4 weeks postpartum was comparable with 35.0 episodes/number of women breastfeeding weeks × 1,000 reported for Australian women, 7 but more than double that reported for Chinese women for the same period. 10
Lactation mastitis has been identified as a significant factor in weaning decisions.21–23 However, while some women may give mastitis as their reason for discontinuing breastfeeding, most women who suffer the condition continue to breastfeed. We found no significant association between acute mastitis and duration of breastfeeding and this is consistent with the findings of an Australian study. 7 On the other hand, studies conducted in Scotland 5 and New Zealand 8 reported that a history of mastitis was associated with longer overall duration of breastfeeding, and it has been postulated that mastitis is an indicator of ample milk supply. 8
A number of potentially avoidable risk factors for mastitis associated with poor nursing technique were identified in this study. Cracked nipples have consistently been associated with mastitis in Western countries,6–9,24 and nipple trauma related to inappropriate nursing technique18,24,25 may provide an entry point for pathogens that lead to mastitis.7–9 Cracked or sore nipples are common problems in the early postpartum period, 26 and almost half (46.7%) of all women in this study had experienced cracked and/or sore nipples in the first 4 weeks following discharge from hospital. While nipple trauma and pain during nursing were not found in this study to be independently related to mastitis in the first 4 weeks, if these problems persisted beyond the first 4 weeks, they were independently associated with mastitis between 5 and 12 weeks. This highlights the importance of the mastery of correct nursing technique in the early postpartum period. In Iran, the first routine MCH clinic visit is scheduled at 1 month postpartum and there is no community midwifery service to assist new mothers to successfully establish breastfeeding in the early postdischarge period. Thus, a greater emphasis on supporting mothers to correctly attach and position their infants while in hospital may minimize the risk of cracked nipples, and subsequently mastitis, postdischarge.
While nursing technique is no doubt important, recent studies suggest that pain on nursing and cracked nipples may be a clinical sign of mastitis 27 possibly caused by the highly virulent exfoliative toxins produced by Staphylococcus aureus, 28 a bacterial species more commonly found in the breast milk of women with mastitis compared with healthy controls. 29 Further studies are warranted to determine if cracked nipples are a cause or consequence of mastitis.
Breast engorgement was significantly associated with acute mastitis between 5 and 12 weeks postpartum. Breast engorgement is a normal physiological process experienced by new mothers usually within 48–72 hours after delivery. 30 However, it may also occur due to ineffective suckling and insufficient removal of milk from the breast, causing milk stasis or blockage of milk ducts. In an engorged breast, the nipple can be stretched flat and the baby may be unable to pull the nipple into their mouth, consequently the nipple may become cracked.1,25 Thus, breast engorgement and cracked nipples can occur in concert and predispose the mother to mastitis. In an effort to reduce the likelihood of engorgement and associated problems, mothers should receive anticipatory guidance on the risks associated with missing or delaying feeds and the advantages of demand feeding.
Expressing breast milk was significantly associated with acute mastitis both in the first 4 weeks and between 5 and 12 weeks, which is consistent with the findings of a recent Spanish study that reported the use of breast pumps as a risk factor for mastitis. 4 The majority of women (95%) who expressed milk in the first 4 weeks used a manual pump and while we did not ask how frequently mothers expressed milk, a recent study reported that expressing several times a day was a risk factor for development of mastitis. 9 Milk expression may cause pain in the nipple from overstretching, and inappropriate use of a breast pump may lead to nipple trauma.31,32 On the other hand, expressing breast milk provides an opportunity for mothers to exercise lifestyle choices while continuing to nurse and has been associated with the success and duration of breastfeeding. 33 Furthermore, the association between breast milk expression and mastitis seen in this study may be an example of reverse causality. Expressing breast milk and using breast pumps are commonly recommended to minimize breast engorgement when mothers develop mastitis.2,4 As women were asked if they had expressed milk since their last clinic visit and not asked specifically if they had expressed milk before or after developing mastitis, it is unclear whether breast milk expression was the cause or consequence of mastitis in this study.
A decline in breastfeeding, whereby women changed from full or exclusive breastfeeding to combination feeding, was associated in this study with an increased risk of acute mastitis between 5 and 12 weeks, but inexplicably with a decreased risk at 4 weeks. This latter finding is inconsistent with the literature as an increased risk of mastitis associated with supplementary feeding has been reported previously 6 and there is an increased risk of engorgement and blocked ducts if the level of breastfeeding declines suddenly, particularly in the early postpartum period when milk production is high. 34
The use of a pacifier was a significant risk factor for acute mastitis in the first 4 weeks and between 5 and 12 weeks. Pacifiers may contribute to the development of mastitis in a variety of inter-related ways. First, the use of a pacifier may promote a non-nutritive, superficial sucking habit, which does not effectively strip the breast of milk, 35 leading to engorgement and blocked ducts. 1 The use of a pacifier also has been associated with increased risk of sore and damaged nipples in a number of studies36,37 while the pacifier itself may be a source of oral contamination and transmission of pathogens. 38 Finally, in countries where pacifiers are not routinely used, mothers typically resort to other methods to soothe their infant, which include carrying and rocking, as well as breastfeeding. 39 Given that infant crying and fussiness are a common and frequent occurrence, these mothers are likely to breastfeed frequently, thus reducing the likelihood of breast milk stasis and engorgement and consequently the risk of mastitis.
Of particular concern was the universal prescription in this study of antibiotics for women suffering from acute mastitis. Antibiotics are not routinely prescribed as first-line treatment for mastitis in other countries,5,29 and many women with potential pathogens in their breast milk recover spontaneously with conservative management (effective milk removal and supportive measures). 2 Milk culturing is not commonly practiced in Iran, or elsewhere, and hence antibiotics are prescribed without knowing the etiology or the antibiotic susceptibility of the microorganism involved. Delgado et al. 27 have warned against the indiscriminate use of broad-spectrum antibiotics to treat mastitis as they may lead to a worsening of the symptoms since strains that cause mastitis may exhibit multiresistance to drugs and/or form biofilms. Before discharge from hospital, breastfeeding mothers should be instructed how to recognize the early onset of symptoms of mastitis and to conservatively manage the condition. Antibiotics should only be prescribed if symptoms do not improve after 24 hours and preferably after breast milk culture and antibiotic susceptibility testing have been undertaken, although there is some debate over the value of breast milk culture. 29
The strength of this study is that a large representative cohort of mothers was followed prospectively from birth to 6 months with four follow-up visits during this interval. A limitation of this study was that mastitis was self-reported by mothers. However, we verified self-diagnosis by applying a definition of acute mastitis based on reported symptomatology, which has been used by others.7,9 Nevertheless, cases of subacute mastitis will have been missed as not all women with local breast symptoms have systemic symptoms. 1 A further limitation is that we did not investigate a number of risk factors such as a prior or family history of mastitis and use of antibiotics, antifungal medication, and nipple creams; all of which have been shown in a recent case–control study to be associated with an increased risk of mastitis. 4 The small number of cases identified in this study introduced a small case bias, 19 resulting in a wide 95% CI for a number of explanatory variables. The penalized maximum likelihood estimation proposed by Firth 20 was used to reduce this bias.
Conclusions
The incidence of acute mastitis in Shiraz, Iran, is similar to that reported in Western countries. Most risk factors identified in this study are associated with poor nursing technique and potentially modifiable with appropriate support and anticipatory guidance in the early postpartum period. It is recommended that the breastfeeding support offered in the hospital setting be improved and supplemented with community-based midwifery services for at least 2 weeks. These measures may go some way to help avoid the risk factors of mastitis, which are commonly associated with poor breastfeeding technique.
Footnotes
Acknowledgments
We are grateful to the mothers who participated in this study and the research assistants who helped with data collection.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.