
Abstract
Abstract
Background:
Breastfeeding is the optimal form of infant nutrition, yet national rates are below recommendations with persistent disparities. Breast pumps may address the reasons that mothers discontinue breastfeeding.
Objectives:
To determine whether breast pump use increases exclusive breastfeeding at 1.5–3.5 months postpartum.
Materials and Methods:
We reviewed charts for maternal-infant descriptors and feeding type for infants born between November 2013 and June 2014 who received any breast milk at a visit <14 days of age in our inner-city pediatric practice. We compared feeding at 1.5–3.5 months between those with breast pump and those without breast pump.
Results:
Of the 905 infants with feeding type recorded, 487 (54%) received any breast milk, of whom 355 (72.9%) had a visit at 1.5–3.5 months [95.4% African American (AA)]. Rates of any breastfeeding (93.8% vs. 38.9%) and exclusive breastfeeding (50.0% vs. 17.8%) were significantly higher in non-AAs than in AAs. Due to small numbers of non-AAs, further analyses were conducted for AAs only. The rate of exclusive breastfeeding at 1.5–3.5 months (19.4% vs. 16.3%) was similar between those with a breast pump and those without a breast pump, whereas rates of any breastfeeding were higher among those with no breast pump (46.9% vs. 31.4%, p = 0.004). Also, among AA mothers, rates of feeding at the breast were lower (21.5% vs. 44.4%, p < 0.0001) and rates of feeding expressed breast milk were higher (16.6% vs. 8.2%, p = 0.02) among those with a breast pump versus those without a breast pump.
Conclusions:
Although breast pumps were free, breast pump use among predominantly AA WIC-eligible mothers was not associated with increased rates of exclusive breastfeeding at 1.5–3.5 months postpartum.
Introduction
B
Breast pumps have been around for almost a century; however, over the past 20 years, they have gained in popularity and could be considered an asset for breastfeeding mothers. 19 Expressing breast milk for infant feeding is one way that mothers can address some of the common issues cited as reasons for discontinuing breastfeeding. These include decreased supply, concern about infant nutrition and weight, inadequate latch, mother or infant medical conditions, and returning to work or school.14,20,21 Studies have shown that within an infant's first 24–48 hours of life, 28–46% of breastfeeding mothers had expressed breast milk,22,23 with rates that continue to increase over the first 6 months of life before trending down between 6 and 12 months of life.22,24–27 Other studies suggest that less than 1–6% of mothers exclusively use expressed breast milk.23–25 After implementation of the Affordable Care Act (ACA), insurance companies are required to provide comprehensive lactation support and counseling, in addition to covering breastfeeding equipment. 28 Two prior studies reported that a breast pump loan program for participants in WIC (Special Supplemental Feeding Program for Women, Infants and Children) was associated with higher rates of breastfeeding initiation 29 and delayed requests for formula. 30 This suggests that breast pump use may have the potential to increase rates of breastfeeding duration and exclusivity. In a qualitative study that also enrolled low-income African American (AA) WIC participants, mothers described breast pumps as offering a “sense of security,” since expressing milk with a breast pump was considered by some as more acceptable than feeding at the breast. 31 However, research is limited, and questions remain about the impact of breast pump use on breastfeeding in high-risk populations. 32
Health disparities in rates of breastfeeding by race and ethnicity are well described.31,33–34 Additional disparities that co-associate include poverty, WIC participation, lower educational level, and single marital status. Barriers identified by low-income AA women participating in WIC included knowledge deficits about the benefits of breastfeeding, breasts being viewed as sexual objects rather than as a means for nutrition, lack of support within their families and community, in part, due to limited experience with breastfeeding by these individuals, and lack of support by healthcare providers. 31 Our Pediatric Practice (Rainbow Babies and Children's Hospital, Cleveland, Ohio) serves a predominantly inner-city, AA, WIC-eligible population. A retrospective chart review performed by us in 2008 revealed breastfeeding rates that were well below regional and national rates. 35 We planned to update information on breastfeeding rates at our practice. Since that time, among other changes, breast pumps have become available free of cost to the families we serve.
Our primary aim for this study was to determine rates of exclusive breastfeeding, any breastfeeding (combined feeding of breast milk and formula), feeding at the breast, and feeding by provision of expressed milk at the 2 month visit in this population. Our secondary aim was to determine the impact of breast pump use on exclusive breastfeeding, any breastfeeding, feeding at the breast, and feeding by provision of expressed milk at the 2 month visit. We hypothesized that an infant whose mother had a breast pump, compared with one without, would be more likely to be exclusively breastfed or at least to receive a combination of breast milk with formula at 2 months of age.
Materials and Methods
Study design, setting, and population
We completed a retrospective chart review of infants born over a 7-month window (November 1, 2013–June 30, 2014) who were seen at the Pediatric Practice of Rainbow Babies and Children's Hospital, an inner-city, tertiary care center-based practice in Cleveland, OH. The study start date coincided with the initiation of the practice-based breast pump provision under the ACA, and the study duration related to the feasibility of review. All infants born during the study window with a newborn visit in the first 14 days of life were included. Infants whose mothers completed a request form for an electric breast pump and/or had documented breast pump use in the first 14 days of life were classified as having a breast pump. Infants who were ever breastfed, but whose mothers did not have a breast pump request form and/or documented use in the first 14 days of life were classified as not having a breast pump. Infants who were formula feeding only at the newborn visit were considered when calculating breastfeeding rates at our Pediatric Practice, but they were excluded from additional data collection and analyses for this study. Infants who were born outside of the study time window or born within the study time window but did not have their initial newborn visit at the Pediatric Practice within the first 14 days of life were excluded from the study. The population served by the Pediatric Practice is 95% AA, with 89% of families on public insurance and WIC eligible. The breast pump provided by insurances was a Medela™ brand, portable double electric breast pump, which retailed for approximately $275. The study was approved by the University Hospitals Cleveland Medical Center Institutional Review Board.
Data collection and outcomes
Charts were reviewed for all infants born during the study period to determine eligibility, with a detailed review of the maternal and infant paper and electronic medical records of those who met inclusion criteria. Infant descriptors included date of birth, gestational age, birth weight, and gender, and maternal descriptors included age, gravity, parity, type of delivery, race, insurance type, presence of partner in the home, and prior breastfeeding experience. At the newborn visit (within 14 days of birth) and at the 2 month well-care visit, we recorded visit date to calculate the infant's age and type of feeding, including feeding at the breast, expressed breast milk, or formula. The permissible age range of the 2 month visit was defined as 1.5–3.5 months due to late, missed, and rescheduled well-care visits, which are frequent in our practice.
“Exclusive breastfeeding” was defined as the provision of breast milk only (feeding at the breast or expressed breast milk with vitamin drops but no water or formula), and “any breastfeeding” was defined as feeding both breast milk and formula. The provision of “expressed breast milk” was defined as stated. The primary outcome was exclusive breastfeeding at 1.5–3.5 months. The secondary outcomes were other feeding types, including any breastfeeding, feeding at the breast, and feeding expressed breast milk at this visit. We looked at the impact of having a breast pump on both the primary and secondary outcomes.
Data analysis
We first examined infant and maternal descriptors for all eligible maternal-infant pairs, and we compared those infants who did and did not have a 2-month visit by using Chi-square and t-tests. All feeding types at 1.5–3.5 months, including exclusive breastfeeding, any breastfeeding, feeding at the breast, and use of expressed breast milk between non-AA and AA mothers, were explored by using the Chi-square test. Both numerical and categorical forms of gestational age, birth weight, and maternal age were examined. Maternal age was categorized by using age quartiles, whereas gestational age and birth weight were dichotomized by using clinically established cut points (<37 weeks for preterm and <2,500 g for low birth weight). Infant and maternal characteristics that potentially associated with breastfeeding outcomes were identified by using the Chi-square and t-tests. Because of racial disparities that are significantly associated with sociodemographic factors and feeding method,33–34 we determined that a race-stratified analysis was desirable. Given that the population in our pediatric practice is predominantly AA (95%), the available sample size for non-AAs was small. Therefore, we explored the associations between breast pump use and feeding method in non-AA mothers by using Fisher exact test, and in AAs by using the Chi-square test, and we performed our main analysis only for the AA group. Due to the potential for differential impact of breast pump use among mothers of premature versus term infants, we examined low birth weight (<2,500 g) and prematurity (<37 weeks gestational age) combined as a single factor versus breast pump use among AA mothers by using the Chi-square and Fisher Exact tests; due to no impact of the pump on 1.5–3.5 months exclusive breastfeeding, a stratified analysis was not indicated.
Factors that independently associated with exclusive breastfeeding in AA mothers were determined by using logistic regression analysis. We present adjusted odds ratios with 95% confidence intervals for exclusive breastfeeding at 1.5–3.5 months. Factors that independently associated with exclusive breastfeeding were considered and estimated from a stepwise model selection procedure that included all available information. In addition, the pattern of change in exclusive breastfeeding from the newborn to the 2-month visit between mothers with and without a breast pump was examined by using the longitudinal generalized estimating equation model. An interaction between visit and breast pump was added in the model to determine whether the change in exclusive breastfeeding from the newborn to 1.5–3.5 months was similar between the breast pump and no breast pump groups. All analyses were performed by using SAS version 9.4 (SAS, Inc., NC). Two-sided p-values were presented, and p < 0.05 was considered as statistically significant.
Results
Population: A total of 932 eligible newborn visits occurred over the study period. Records were available for 905 (97.1%), with 487 mothers (53.8%) providing any breast milk, of whom 229 out of 487 (47%) had documented breast pump use or a submitted breast pump request form. At 1.5–3.5 months, 355 maternal-infant pairs (72.9%) had a visit and were included in analyses. Maternal and infant descriptors, including maternal age, race, delivery type, parity, presence of a partner in the home, infant birth weight, and gestational age, did not differ between those with a visit and those without a visit at 1.5–3.5 months (data not shown). Among the 355 mothers, mean maternal age was 24.2 years (SD 5.2), 332 (95.4%) were AA, 204 (57.5%) were multiparous, 252 (71.2%) delivered vaginally, and 170 (49.6%) had a partner in the home. Among the infants, mean birth weight was 3,155 g (SD 531) and mean gestational age was 38.3 weeks (SD 1.7); 56 (15.8%) were of either gestational age <37 weeks or birth weight <2,500 g.
Overall Breastfeeding Rates: The rate of exclusive breastfeeding among all mothers at 1.5–3.5 months was 19.2% (68/355). The rate of any breastfeeding was 41.4% (147/355), with 34.7% (123/355) feeding at the breast, and 13.2% (46/349, 6 missing) providing expressed breast milk.
Maternal and Infant Characteristics Associated with Breastfeeding Rates: The maternal and infant characteristics associated with exclusive breastfeeding at 1.5–3.5 months are shown in Table 1. In this unadjusted analysis of all maternal-infant pairs, the following factors were significantly associated with exclusive breastfeeding at 1.5–3.5 months: older maternal age, being of non-AA race, having a partner in the home, and a term birth or normal birth weight infant. Feeding method overall and by race (AA vs. non-AA mothers) at 1.5–3.5 months is presented in Figure 1. Although more AA than non-AA mothers had a breast pump (48.6% vs. 28%, p = 0.045, data not shown), the rates of all breastfeeding types, including exclusive breastfeeding (50% vs. 17.8%), any breastfeeding (93.8% vs. 38.9%), feeding at the breast (75% vs. 32.5%), and feeding of expressed breast milk (31.3% vs. 12.5%), were significantly higher for non-AA mothers than for AA mothers (p < 0.05 for all).
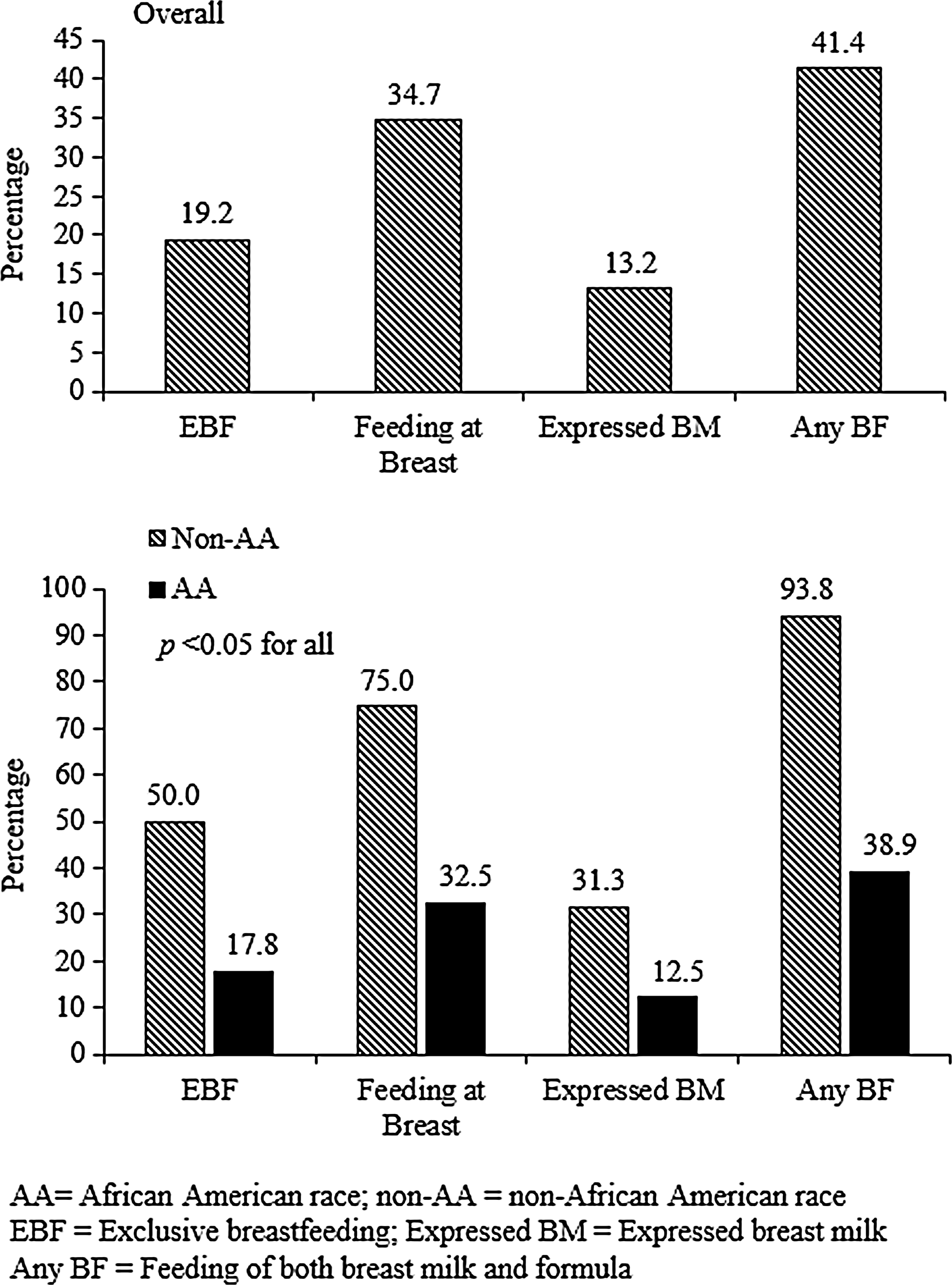
Feeding method at 1.5–3.5 months overall and by race.
AA, African American; BW, birth weight; EBF, exclusive breastfeeding; SD, standard deviation.
Impact of Breast Pump Use on Breastfeeding Rates: We then explored associations between breast pump use and feeding method at 1.5–3.5 months in both non-AA and AA mothers (Fig. 2) and overall. Among AA mothers, there was no significant interaction between use of a breast pump and having a preterm or low birth weight baby (data not shown); this analysis could not be performed for non-AA mothers due to the small sample sizes. There was no evidence that breast pump use was associated with significantly increased rates of exclusive breastfeeding in either race group. Rates of exclusive breastfeeding among non-AA mothers with a breast pump versus those without a breast pump were 40.0% versus 54.6%, respectively (p = 1.0), and among AA mothers they were 16.3% versus 19.4%, respectively (p = 0.46). The rates of any breastfeeding also did not differ significantly among non-AA mothers with a breast pump versus those without a breast pump (100% vs. 90.9%, p = 1.0). However, the rates of any breastfeeding were significantly lower among AA mothers with a breast pump versus those without a breast pump (31.4% vs. 46.9%, p = 0.004). Overall, mothers (both AA and non-AA) who had a breast pump were less likely to feed at the breast (21.5% vs. 44.4%, p < 0.0001) and more likely to feed expressed breast milk (16.6% vs. 8.2%, p = 0.02) to infants at 1.5–3.5 months.
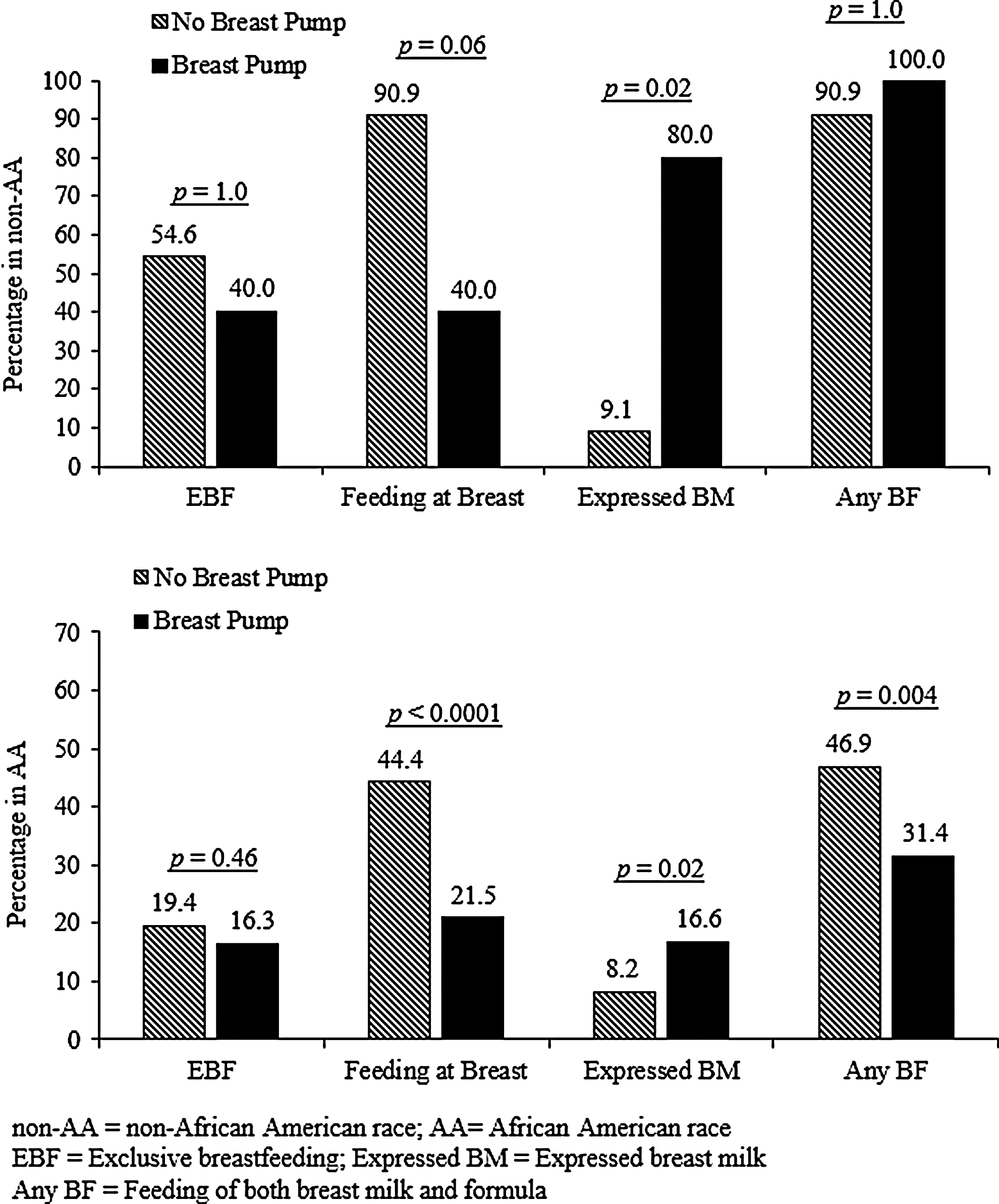
Association between breast pump use and feeding method at 1.5–3.5 months by race.
Factors Independently Associated with exclusive breastfeeding among AA Mothers: Further analyses were stratified by race due to the statistically significant racial differences in all aspects of breastfeeding and breast milk provision noted in this study and other publications.33–34 Since the number of non-AA mothers in our sample was small (n = 23, 4.6%), further analyses were conducted for AA mothers only. Multivariate analysis (Table 2) shows that exclusive breastfeeding among AA mothers at 1.5–3.5 months was positively associated with having a partner in the home, with older maternal age, and with a term or normal birth weight infant; there was no impact of having a breast pump after adjustment for factors that independently associated with exclusive breastfeeding (p = 0.96). In addition, exclusive breastfeeding rates were similar between mothers with a breast pump and those without a breast pump at both the newborn visit (57.6% vs. 63.1%) and 1.5–3.5 months (16.3% vs. 19.4%), and the pattern of reduction by time was similar between the two groups with no significant interaction (Fig. 3).
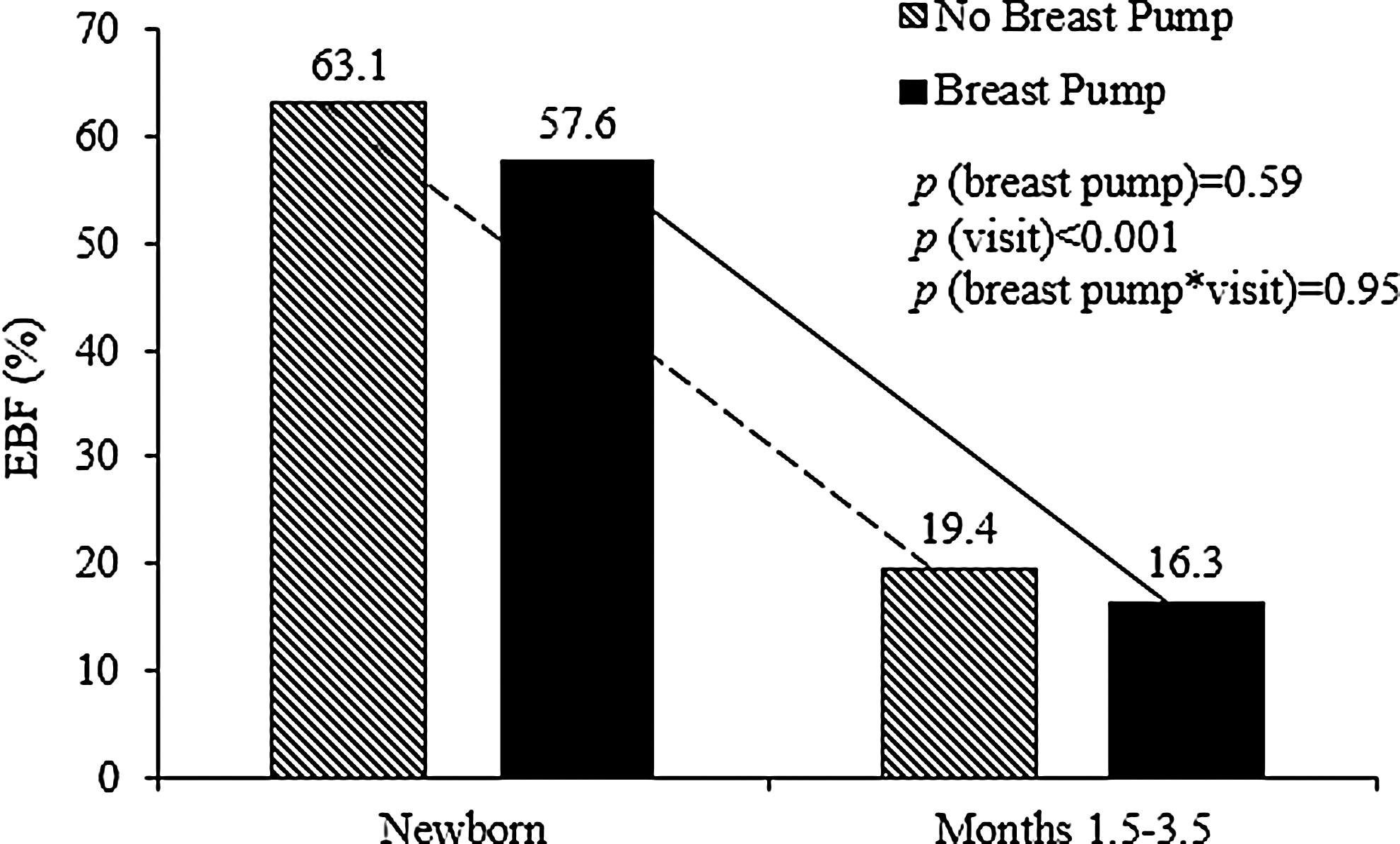
Change in rate of exclusive breastfeeding (EBF) from the newborn visit to 1.5–3.5 months among African American mothers.
n = 332.
OR, odds ratio; CI, confidence interval; LBW, low birth weight.
Discussion
Breastfeeding rates continue to be well below national recommendations in the inner-city, predominantly AA population at our Pediatric Practice. At the newborn visit, 53.8% of infants were breastfed at all, which is less than our birthing hospital's breastfeeding initiation rate of 95% for this period and below the HP 2020 initiation goal. At 1.5–3.5 months, rates drop to 19.2% exclusive breastfeeding and 42.5% any breastfeeding. However, we note improvement from 2008 data that showed a newborn visit rate of 40.8%, with rates of 10.6% exclusive breastfeeding and 24.5% any breastfeeding at a time point equivalent to 1.5–3.5 months. 35 Although in this study we examined associations with breast pump availability, multiple factors have likely impacted these changes, including our birthing hospital's work toward Baby-Friendly designation (achieved December 2014), and local and national increases in breastfeeding rates over time.16,36 Our breastfeeding rates reflect an ongoing health disparity for the AA WIC-eligible mothers who comprise >95% of those served at our Pediatric Practice, as compared with state-wide Ohio data, which show a 3 month exclusive breastfeeding rate of 41.5% ± 7.9%. 36
Looking more closely at other correlates of breastfeeding in our population, we found that exclusive breastfeeding at 1.5–3.5 months was associated with having a partner in the home, older maternal age, term gestation, and normal birth weight. Prior studies have found associations between exclusive breastfeeding and older maternal age,11,14,37 as well as with being married,12,14 which may be comparable to our measure, “having a partner in the home.” Exclusive breastfeeding after 10 weeks of age is associated with term, as compared with preterm, gestation. 11 The rate of breastfeeding initiation is lower for infants born before 40 weeks (35–39 weeks) than for those born ≥40 weeks gestational age. 38 Similarly, rates of breast milk provision for preterm infants are lower than those for full-term infants, with, for example, a 67% rate of breast milk feeding at discharge home among very low birth weight infants versus a mean overall hospital breastfeeding rate of 87% in the first 24–96 hours of life among the 111 hospitals studied. 39
Although having a breast pump had no impact on exclusive breastfeeding at 1.5–3.5 months after adjustment for relevant factors, it was associated with being more likely to feed expressed breast milk, and with being less likely to feed directly at the breast. This increased use of expressed breast milk suggests that there is still a possibility, not shown here, that providing mothers with a breast pump may help to encourage use of any breast milk for a longer duration than relying on feeding at the breast alone. However, there is evidence that mothers who use a breast pump in the early postpartum period due to breastfeeding difficulties or return to employment, and particularly those who pump frequently, are at higher risk for a shorter duration of feeding at the breast. 40 In addition, there are limited data that decreased direct feeding at the breast with increased feeding of expressed milk may actually reduce some of the potential benefits of breast milk.41,42 There are other social factors that can play into the decision to use a breast pump, which we were unable to explore in this study. Prior studies found that lower infant birth weight, prematurity, difficulty or no prior experience with breastfeeding, viewing the breasts as sexual objects, cultural norms related to breastfeeding, concern about breast milk supply, higher maternal body mass index, higher socioeconomic status, having a college degree, and planning to return to work by 6 months postpartum are associated with breast pump use.24,26,31,43 Clearly, careful prospective studies will be needed to address the questions raised here.
This study is one of the first to examine the impact of the availability of a free breast pump on achieving HP 2020 goals after implementation of the ACA. Our Pediatric Practice serves an inner-city, predominantly AA population, whose sociodemographic characteristics are identified risk factors for lower breastfeeding rates. Since earlier literature demonstrated the benefits of a breast pump loan program among low-income women receiving WIC,29–30 this is a particularly important question to address in this population. One strength of this study is the meaningful sample size with a predominantly AA WIC-eligible population. This study can serve as a benchmark for future work to determine whether breast pump availability is more prevalent after implementation of the ACA, and it can positively impact the achievement of HP 2020 breastfeeding goals for this population.
Limitations of this study are inherent to our population and the study design. First, the families we serve have many barriers to care, which likely contributed to the high number of missing 2 month well-care visits. However, since we showed that those who missed this visit were not demographically different than those who attended the visit, this is likely not relevant to our results. Second, many pertinent psychosocial variables we had hoped to obtain are unmeasured confounders, such as daycare attendance, when the mother had to return to work/school, maternal smoking status, post-hospital lactation support, WIC participation, and maternal educational attainment. Due to the retrospective nature of the study and inconsistent chart documentation, we could not include these. Third, our study focused on a geographically specific, relatively homogenous patient population at one practice. We recognize that there are factors related to how we measured “having a breast pump” that could impact the analysis, and there is a chance that mothers in the breast pump group may have never had or used a pump, whereas those in the “no pump” group may have used a breast pump. Although breast pumps were free and available at the start of ACA implementation, we acknowledge a possible lag in the actual ability of mothers to receive breast pumps; although our nurses did not report obstacles to service, we did not keep data on this process. Thus, a mother could have requested a breast pump but never obtained it or never used it, or could have obtained a breast pump from elsewhere with no documentation in the record.
Conclusion
Nationally, much progress remains to achieve the HP 2020 breastfeeding goals, particularly among subpopulations who are at risk for not breastfeeding. We found that in an inner-city, predominantly AA, WIC-eligible population, breast pumps were not associated with increased exclusive breastfeeding at 1.5–3.5 months. Breast pumps were associated with increased use of expressed breast milk and decreased feeding at the breast for both AA and non-AA mothers, and, surprisingly, with significantly lower rates of any breastfeeding for AA mothers at 1.5–3.5 months. Coverage for lactation equipment associated with the ACA may ultimately help to address some of the barriers to continued breastfeeding in high-risk, inner-city, WIC-eligible, predominantly AA populations, but clearly, we need to understand much more about the impact of breast pump availability.
Footnotes
Acknowledgment
This work was presented at the Pediatric Academic Societies Meeting in Baltimore, MD, on May 1, 2016.
Disclosure Statement
No competing financial interests exist.