
Abstract
Abstract
Objective:
To report breastfeeding complaints of women diagnosed with cancer during pregnancy and correlate success with characteristics of their treatment.
Materials and Methods:
This is a prospective cohort study of women diagnosed with cancer during pregnancy who attempted breastfeeding. We surveyed participants about breast engorgement, milk let down, and consistent breast milk production through mailed questionnaires. Treatment details, including the type and number of chemotherapy cycles given during pregnancy and antepartum or postpartum depression, were collected. A single pathologist evaluated surgical specimens to note lactational changes while blinded to patient's treatment. The primary endpoint was successful breastfeeding without reporting any lack of or decreased breast milk production.
Results:
When comparing women who underwent chemotherapy during pregnancy to women who did not, there was a significant difference in reporting a lack of or a perceived decrease in breast milk supply and the need to provide supplemental feeding to their infants (63.5% and 9%, respectively, p < 0.001). In the women who received chemotherapy, there was no significant difference in maternal age, cancer type, or stage with regard to breastfeeding difficulties. Gestational age at the first cycle and the number of cycles were significant factors associated with breastfeeding difficulties (p = 0.006 and p = 0.0003, respectively). Antepartum and postpartum depression was not associated with decreased breast milk production. A lack of lactational changes and significant lobular atrophy were noted in the women given neoadjuvant chemotherapy.
Conclusion:
Women who undergo chemotherapy during a pregnancy are more likely to report breastfeeding difficulties.
Introduction
T
Breast milk has many benefits to the mother and her newborn. 10 It provides the infant with the essential nutrients, antibody-specific immunoprotection, and the development of a favorable gut microbiome.11,12 Infants who are breastfed have a reduced risk of asthma, atopic allergies, and obesity. 10 Breastfeeding also benefits the mother while providing an important maternal–neonatal bonding experience. Breastfeeding is associated with a decreased risk of type II diabetes, cardiovascular disease, and ovarian and breast cancer.10–13
There are limited data about the feasibility of lactation after chemotherapy during pregnancy. Breastfeeding while receiving chemotherapy is contraindicated as neonatal leukopenia and thrombocytopenia have been reported in an infant receiving breast milk from his mother undergoing treatment with cyclophosphamide.14,15 Often when chemotherapy is given during pregnancy, the goal is to protect a 3-week period between chemotherapy exposure and delivery. Whether or not any chemotherapeutic agents will be excreted into the breast milk after this 3-week window depends on multiple factors, including concentration, half-life in the maternal plasma, lipid solubility, molecular size and ionization, protein binding, and the phase of breastfeeding itself. 16
In a previous study of the psychological impact of a cancer diagnosed during pregnancy, 74 women enrolled in the Cancer and Pregnancy Registry completed the Brief Symptom Inventory-18 and Impact of Event Scale on average 3.8 years (standard deviation 2.5) following their cancer diagnosis to address potential variables related to distress. One of the factors related to a higher risk of long-term distress on multiple regression analyses was not producing sufficient milk to breastfeed their infant. 17
To our knowledge, a decreased production of breast milk has not been reported after antepartum chemotherapy. This article will report the breastfeeding experiences of new mothers diagnosed with cancer during pregnancy. Comparisons will be made between the groups with minimal or no breast milk production determined by self-report and those reporting an adequate supply, with regard to the type of treatment during pregnancy, including chemotherapeutic agents, the number of cycles, and/or duration of chemotherapy, anxiety, and/or depression.
Materials and Methods
Subjects who attempted to breastfeed after a pregnancy complicated by any cancer diagnosis were identified from the Cancer and Pregnancy Registry maintained at the Cooper University Hospital. The Registry was established in 1997 and has been approved by the Cooper University Hospital Institutional Review Board. All subjects were enrolled and delivered between July 1998 and August 2013. Enrollment occurs at the time of a cancer diagnosis, so that oncologic, obstetric, and pediatric information is collected prospectively. All participants provided written informed consent. Data collected includes the primary cancer diagnosis, surgical and/or chemotherapy treatment (regimen, doses, number of cycles, gestational age [GA] at first and last treatment during pregnancy), and delivery information, including birth weight, presence or absence of congenital anomalies and complications in the immediate newborn period. Within the first 6 weeks of delivery, patients were sent a questionnaire asking if they planned to breastfeed their infants and in addition if they experienced engorgement of the breasts or “let down sensation” postpartum, change in the color of the nipple, or if the Montgomery glands on the nipple increased in size. Patients who planned to breastfeed were specifically asked if they perceived an adequate production of milk to sustain their infant. For the purpose of this article, “successful breastfeeding” was defined as the patient perceiving an adequate amount of spontaneous breast milk production for their infant. Patients were then asked to report any problems they perceived during breastfeeding. Through questionnaires, patients and obstetricians were surveyed about whether a diagnosis of depression was made either during the pregnancy or postpartum period. No particular depression instrument was given to patients.
All patients attempting to breastfeed did not receive chemotherapy within 3 weeks of delivery. Patients who reported decreased milk production were compared to patients who reported no need to stop breastfeeding or provide any supplementation to their infant. Comparisons included the type of chemotherapy and number of cycles, GA at first and last chemotherapy course during pregnancy, breast surgery during pregnancy, and a diagnosis of antenatal or postpartum depression. A Student's t-test was used to evaluate relationships between quantitative variables, and a Pearson's chi-squared test was used for categorical variables. An association was considered to be significant when p < 0.05. To capture any neonatal effects of breastfeeding after chemotherapy during pregnancy, the pediatricians caring for the children who were breastfed were contacted by mail and asked to provide any blood work performed during the first 6 months of life, and report if the child was treated for infections, medical conditions, or was receiving special developmental services during follow-up.
In a few cases, the pathologic specimens of cancer patients were reviewed by a pathologist blinded to treatment during pregnancy to document the histologic changes of peritumoral lobules in lactation, atrophy, and inflammatory infiltrates.
Results
Ninety-six women in the Registry attempted breastfeeding after a diagnosis of cancer during pregnancy. Cancer diagnoses varied. Breast cancer was the most common diagnosis during pregnancy (65) followed by Hodgkin's (8) and non-Hodgkin's lymphoma (6), ovarian cancer (4), colorectal cancer (3), and thyroid cancer (3). The remaining cancer types included cervical and central nervous system (two each) and one each of acute leukemia, melanoma, and Ewing's sarcoma. Of the entire group, 45 women produced breast milk and successfully sustained their infant on breast milk alone, 32 women did not produce any breast milk, 19 women produced some milk but felt this was not enough to sustain the infant on their breast milk alone and formula or donated breast milk was used. Seventy-four of the 96 women who attempted breastfeeding had received chemotherapy during the second and or third trimesters of pregnancy. There was a significant difference in the percentage of women who reported decreased or no milk production between the chemotherapy exposed group and the group not receiving chemotherapy before delivery. Of the 74 women treated with chemotherapy during pregnancy ending at least 3 weeks before delivery, only 33.8% exclusively breastfed their infants. Forty-nine women (66.2%) reported experiencing breastfeeding difficulties such as no milk let down or production or a decreased amount compared to only 2 women, or 9% of the 22 who did not receive chemotherapy (p < 0.001). Ninety-one percent of the women who did not have chemotherapy during pregnancy were successfully able to breastfeed their infants. Mean maternal age was not significantly different for women who were unable to adequately breastfeed their infant compared to women who breastfed successfully 32.8 ± 3.8 versus 33 ± 4.9, p = 0.734. Among the chemotherapy exposed group, the mean GA at the first chemotherapy treatment in pregnancy was significantly earlier in the group experiencing difficulty compared to the group successfully breastfeeding: 18.5 ± 4.8 versus 21.9 ± 5.3 for those not reporting difficulties (p = 0.006). The average number of cycles for those experiencing minimal or no breast milk production was 5.5 ± 2.3 compared to those reporting ability to breastfeed exclusively 3.8 ± 1.4 (p = 0.0003). The probability of noting a decrease in breast milk production if chemotherapy began at 17 weeks is 75% and 50% at 24 weeks. The GA at the last treatment and the days from last treatment to delivery were not significant factors affecting breastfeeding (p = 0.843 and p = 0.304, respectively; see Table 1).
GA, gestational age; SD, standard deviation.
No relationship between breastfeeding difficulty and maternal depression (p = 0.779); cancer type (p = 0.080); or cancer stage (p = 0.29) was noted. Having lumpectomy during pregnancy compared to postpartum also did not affect breastfeeding success (p = 0.80). In addition, having breastfed a child before the index pregnancy complicated by cancer, or parity itself, did not affect breastfeeding success.
There was a significant difference in the mean GA at delivery for children of mothers receiving chemotherapy (36.7 ± 2.78 weeks) compared with mothers not treated with chemotherapy during pregnancy (38.2 ± 2.93 weeks), p = 0.04. However, this earlier GA at delivery did not affect breast milk production. There was no significant difference in the mean GA at delivery of mothers who received chemotherapy and experienced decreased or no breast milk production compared with mothers who received chemotherapy and did not report any issues with breast milk production, p = 0.17.
The percentage of women reporting breastfeeding difficulties according to the chemotherapy regimen they received during pregnancy is listed in Table 2. For women who were treated with chemotherapy (all cancer types), a trend was noted with 5 fluorouracil/adriamycin/cyclophosphamide (FAC) having a 5.7-fold higher risk of breastfeeding issues compared to adriamycin/cyclophosphamide (AC), p = 0.1238 (Table 3). Peritumoral lobular changes, including atrophy, lymphoplasmacytic infiltration, and portion of the lobules with lactational changes, were evaluated histologically in six surgical breast tissue specimens by a pathologist blinded to patient treatment for breast cancer during pregnancy. In two women receiving adjuvant chemotherapy after surgery, 95% of the lobules demonstrated lactational changes, no lobular atrophy, and minimal to mild lymphoplasmacytic infiltrates. Of the four women who had undergone neoadjuvant chemotherapy before breast cancer surgery, only 5% of lobules in two women, 20% in one woman, and 25% in another woman showed evidence of lactation. Mild (1), moderate (1), and severe (2) lymphoplasmacytic infiltrates were noted and mild to moderate lobular atrophy with varying fibrosis was also observed (Figs. 1–4).
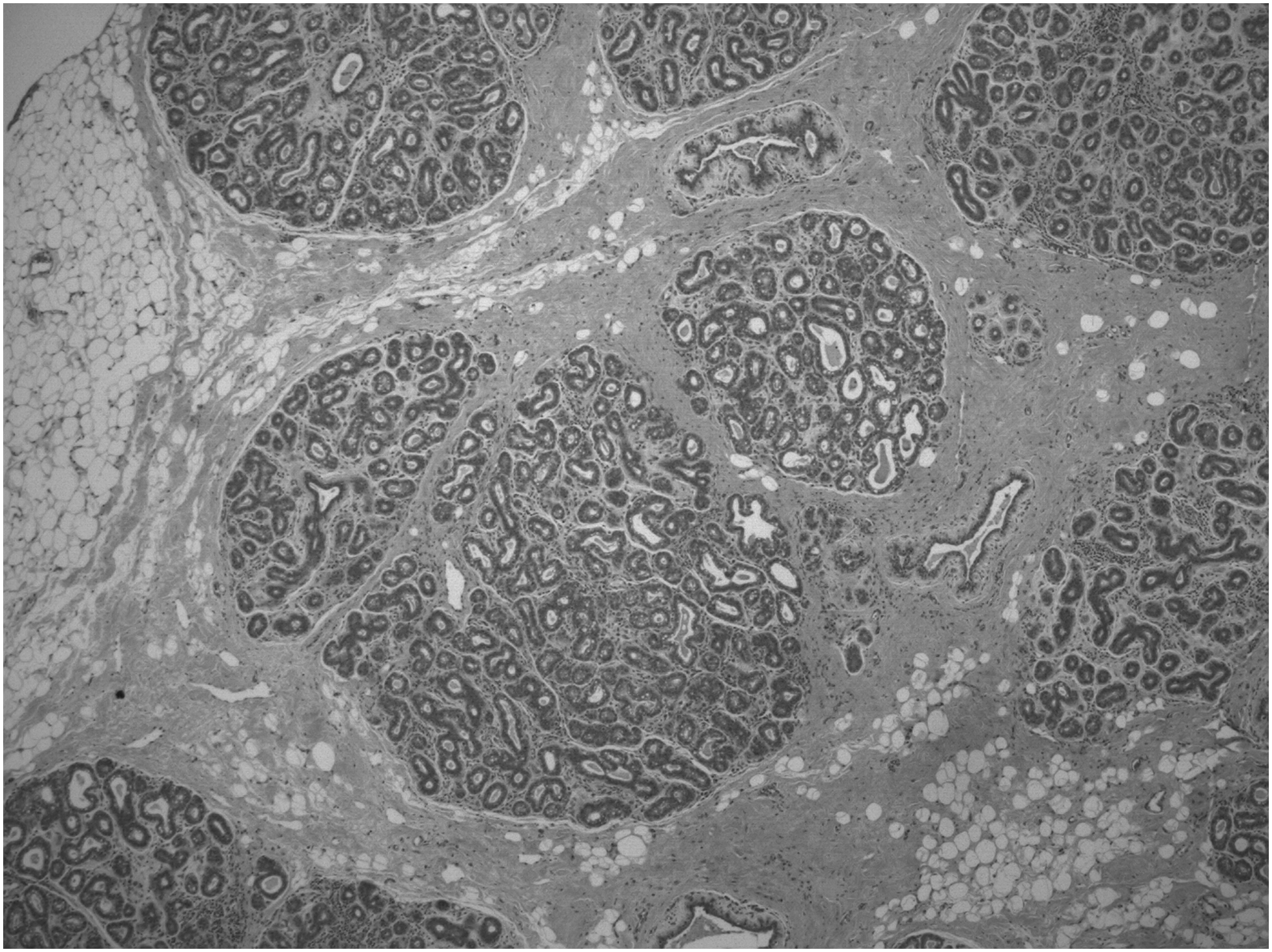
Patient unexposed to chemotherapy before delivery, well-preserved lobules. HE × 40.
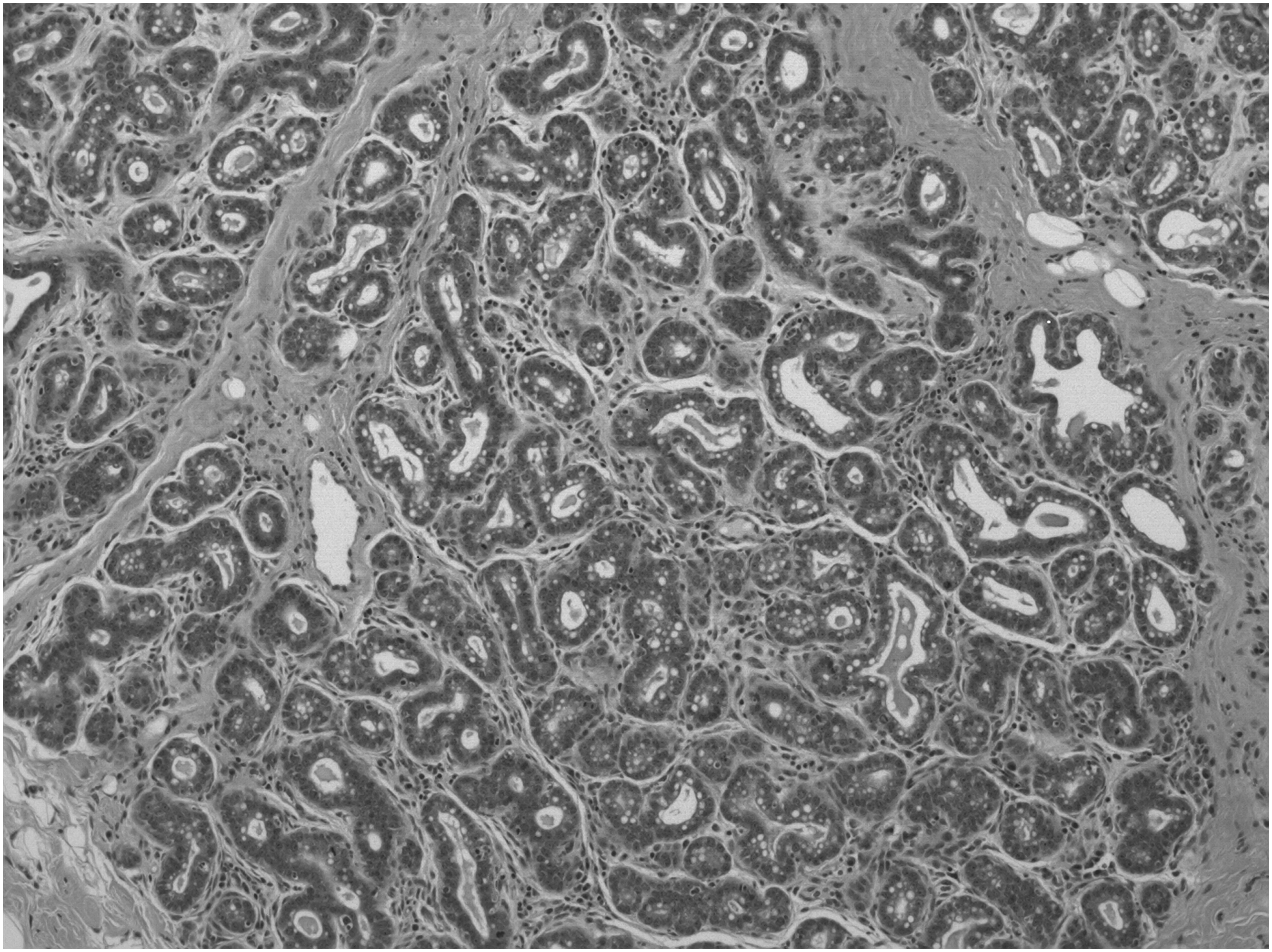
Patient unexposed to chemotherapy before delivery, homogeneous lactation noted in 95% of the lobules and only minimal lymphoplasmacytic infiltration present. HE × 100.
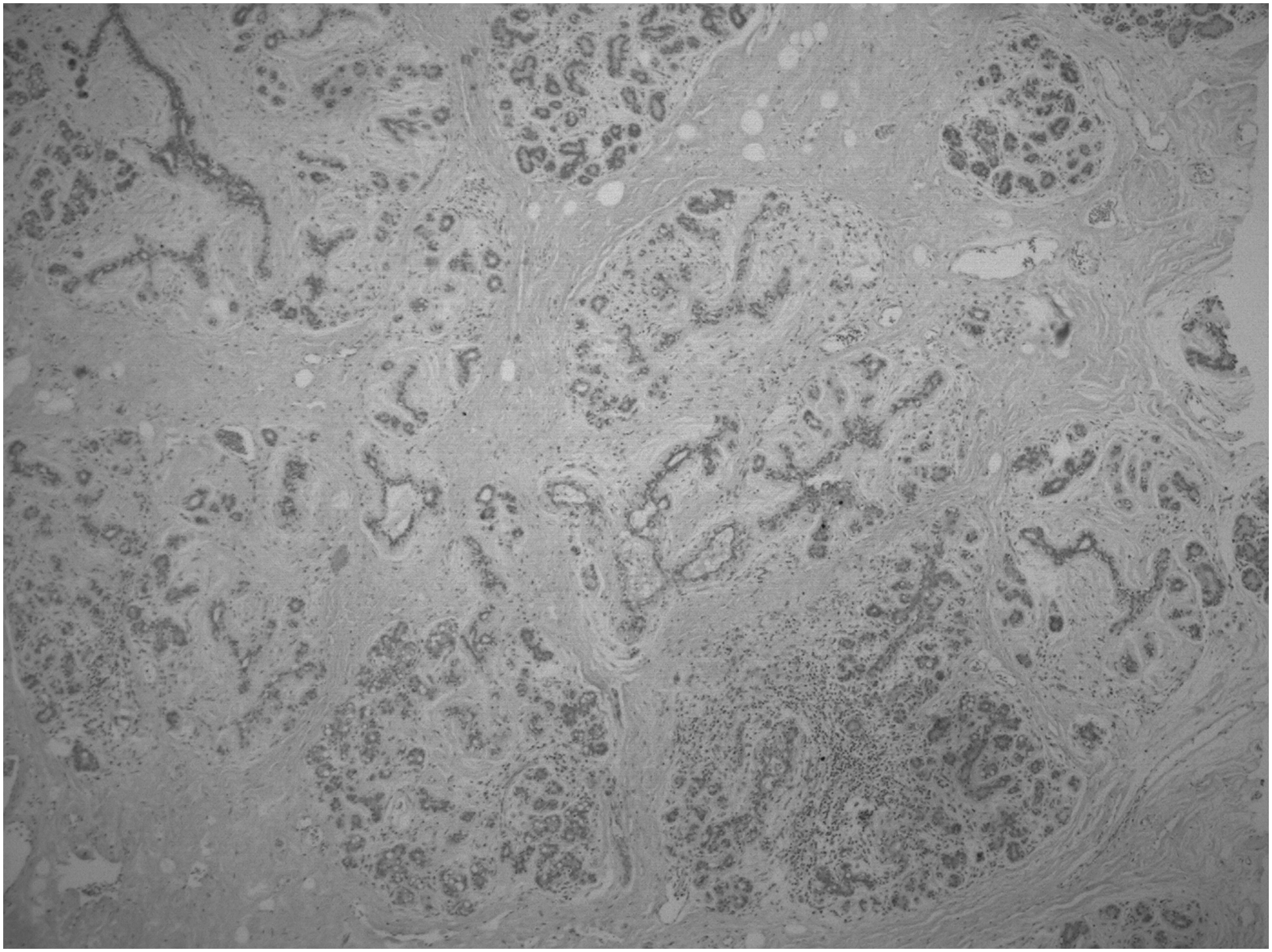
Patient exposed to chemotherapy, lobular atrophy with moderate fibrosis. HE × 40.
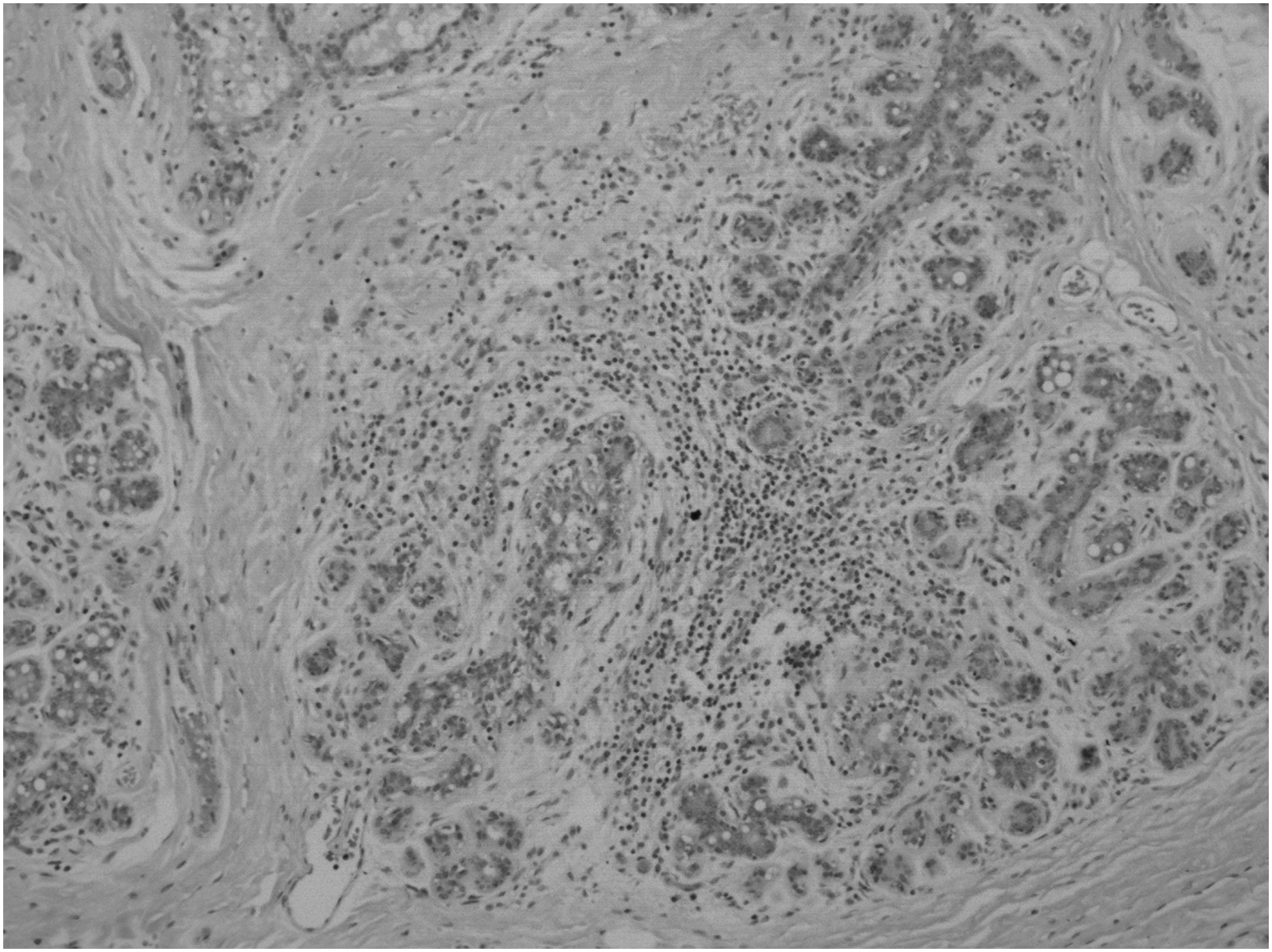
Patient exposed to chemotherapy, severe lymphoplasmacytic infiltrates present, and focal lactation noted in ∼5% of the lobules. HE × 100.
ABVD, adriamycin/bleomycin/vinblastine/dacarbazine; AC, adriamycin/cytoxan; AC + T, adriamycin/cytoxan and paclitaxel or docetaxel; BEP, bleomycin/etoposide/cisplatin; FAC, adriamycin/cytoxan/fluorouracil; FAC + T, adriamycin/cytoxan/fluorouracil and paclitaxel or docetaxel; RCHOP, rituxan/cytoxan/adriamycin/vincristine/prednisone.
Forty-three women in the chemotherapy exposed group reported their infant received at least some breast milk. Surveys were mailed to respective pediatricians and responses were received for 41 out of 43 of these children. No medical issues were reported for 37 of these children. To alleviate concerns that children breastfed after chemotherapy exposure may be somehow immunocompromised and susceptible to infections, pediatricians were asked to report the need for antibiotics or other treatment for infections in these children. In four cases, the pediatricians identified the following medical issues: outbreak of herpes on the face, sinusitis and eczema, seborrhea capitis at 7 months and sinusitis at 23 months; recurrent upper respiratory infections and cough; and nasolacrimal duct obstruction at birth causing recurrent conjunctivitis. In the first case, the patient completed four cycles of bleomycin/etoposide/cisplatin 2.75 months before delivery; in the second case, the fetus was exposed to bleomycin/etoposide/cisplatin 5 weeks before delivery, in the third case, four cycles of adriamycin/cytoxan followed by four cycles of paclitaxel were completed 7.5 weeks before delivery; in the last case, adriamycin/cytoxan was discontinued 3 weeks before delivery. The incidence of “recurrent infections” in the breastfed group after prenatal chemotherapy at least 3 weeks before delivery was 4/41 = 0.098 (CI 0.0317–0.2406).
Discussion
Patients with cancer diagnosed during pregnancy who do not require postpartum chemotherapy may be appropriate candidates who can breastfeed to meet their goals to provide safe and beneficial nutrition via breast milk to their children while benefiting from the maternal–infant bond. This study looked at breastfeeding success when chemotherapy is halted or completed at least 3 weeks before delivery. The number of reports detailing the measurement of chemotherapy in breast milk is limited.18–25 Even if chemotherapy agents are excreted into breast milk, the infant's toxicity, if any, would depend not only on the absorbed volume of milk but also on the oral bioavailability of the drug itself (poor for paclitaxel, for example), and the neonate's own pharmacokinetics. 16 In all cases, at least seven full half-lives between the last chemotherapy treatment during pregnancy and delivery transpired before breastfeeding. When breastfeeding was attempted after a diagnosis of cancer during pregnancy and the patient had not received any chemotherapy, 91% of patients were able to successfully breastfeed and did not note any difficulties. Only 37% of women who attempted breastfeeding after receiving chemotherapy, no closer than 3 weeks before delivery, were able to successfully breastfeed their newborn. Sixty-seven percent experienced either minimal or no milk production. An earlier GA at the first treatment and the number of cycles received during pregnancy were significantly related to decreased breast milk production. Neither the type of cancer, stage, maternal age, depression, gestational age at completion of chemotherapy, nor the number of days between chemotherapy completion and delivery significantly affected breastfeeding success. To better counsel patients about realistic breastfeeding expectations after receiving chemotherapy and to avoid additional distress, patients could be warned about the likelihood of experiencing decreased or no breast milk production. The consistent observation of decreased breast milk production after chemotherapy exposure during pregnancy has not been reported or investigated as to the etiology. Mammary gland development begins during fetal life, with epithelial bud development in the 18–19-week fetus. During puberty, ductal development commences and then proliferative lobular development occurs during the luteal phases of the menstrual cycle. Alveolar development begins during early pregnancy, leading to milk secreting units. 26 Lactogenesis then occurs in two stages: the first stage (secretory differentiation) represents the stage of pregnancy when the mammary epithelial cells differentiate into lactocytes (secretory mammary epithelial cells) with the capacity to synthesize unique milk constituents such as lactose, casein, α-lactalbumin, and fatty acids. In humans, lactogenesis stage I occurs midpregnancy in response to progesterone, prolactin, and human placental lactogen. By midpregnancy, there are extensive lobular clusters and development continues until parturition. 27 Seventy-five percent of women who started treatment by 17 weeks of gestation just before or during lactogenesis stage I experienced decreased or no breast milk production.
The second stage, lactogenesis II, or secretory activation, is the initiation of milk secretion that occurs at about the time of parturition. This is triggered by progesterone withdrawal after the placenta is delivered. An increased synthesis by mammary lactocytes of a number of milk components, including lactose and citrate, occurs. In lactogenesis II period, milk is made in copious amounts during the first 4 days postpartum. Patient's perceive milk “let down” or milk coming in around 40 hours postpartum, with the range being 48–72 hours.
A delay in the onset of lactogenesis II has an adverse effect on the success of subsequent lactation. Lactation performance is affected by a preterm birth with milk volume increasing significantly with advancing GA at delivery.28,29 Mothers of preterm infants are more likely to have problems at this stage, as a result of stress, maternal illness, operative delivery, or antenatal pharmacologic therapies. 28 When measured either by change in milk volume or an increase in levels of milk components, GA at delivery predicts the timing of onset of lactogenesis II with women delivering preterm expressing significantly lower volumes of milk even at day 10 postpartum. This is not felt to be secondary to a deficiency in milk prolactin.29,30 There was no significant difference in the mean GA at delivery within the chemotherapy exposure group between women experiencing a decrease in breast milk production and mothers who received chemotherapy and did not report issues breastfeeding their infants. The two unexposed women who reported minimal or no milk production delivered at 36.3 and 39.3 weeks.
Xenobiotics such as chemotherapeutic agents can act at various points in the development, maturation, or function of the breast secretory epithelium required for lactation. This can include affecting the quantitative development of functional mammary tissue; the functional development of the secretory cell; systemically altering the hormonal milieu supporting lactation; or the delivery of substrates needed for formation of milk itself. 31 For example, mothers who smoke cigarettes have decreased milk volumes in clinical studies.32,33 Histological evaluation of the few cases in this study revealed lobular atrophy with associated lymphoplasmacytic infiltrates and fibrosis in patients with neoadjuvant chemotherapy during pregnancy, suggesting that chemotherapeutic agents may damage the acinar cells of breast lobules directly. These dramatic differences in the lactational changes appreciated in the pathology specimens support our patients' anecdotal reports that after chemotherapy exposure in pregnancy, breast milk production is decreased. We plan to further expand our pathologic review of patients undergoing breast surgery before and after chemotherapy. Future planned studies may help us to elucidate where in the lactational process chemotherapy exerts an effect on breast milk production for patients diagnosed with cancer during pregnancy.
Acute physical and mental stress can impair milk ejection reflux by affecting release of oxytocin during a feed. If this occurs repeatedly, it could reduce milk production by preventing full emptying of the breast at each feed. Both maternal stress and fetal stress during labor and delivery are associated with impaired lactogenesis. 34 Emotional stress postpartum may impair lactogenesis, but it is unclear if this is a reverse causation in that decreased milk production35,36 leads to emotional stress. Certainly having a cancer diagnosis during pregnancy can be stressful, but presumably even the patients diagnosed with cancer who did not receive chemotherapy during pregnancy would experience a level of distress about their diagnosis, and the delay of treatment until postpartum. We did not find that a history of depression before or during the pregnancy, or developing of postpartum depression was significantly associated with breastfeeding problems in our cohort. Limitations include the small number of patients attempting to breastfeed after a cancer diagnosis and treatment and the lack of standardization by which all children breastfed after a pregnancy complicated by cancer have blood drawn to exclude neutropenia. One of the limitations of our study is that we did not specifically ask about exclusivity of breastfeeding. The patients exposed to chemotherapy did not report problems in exclusively breastfeeding but rather in the initiation of breastfeeding and that milk production was subjectively decreased or not produced at all. Since this was an observational study, we did not ask pediatricians to perform complete blood counts on the children breastfed after chemotherapy exposure in utero, but none of the women was advised to stop due to neonatal side effects. No patients reported that breastfeeding was halted due to any neonatal reactions, side effects, or illness.
Another limitation is the long time period over which data were collected. Given that cancer and pregnancy occur in 1/1,000 pregnancies, it takes time to accumulate a large enough cohort to detect trends or consistencies. Women offered the observation of a decreased breast milk supply spontaneously. After hearing patients' unsolicited distress and concern repeatedly, it was decided to more formally ask patients to report milk let down and breastfeeding experience and hence the collection of data over many years.
Conclusion
Women who undergo chemotherapy during a pregnancy are more likely to report a decreased breast milk supply. For patients in whom at least 3 weeks have passed between chemotherapy during pregnancy and delivery, we found no adverse affects on the children who were breastfed. We did note that the majority of women motivated to breastfeed who were treated with chemotherapy during pregnancy had difficulty either initiating or sustaining milk production. One of the limitations of our study is that we did not specifically ask about exclusivity of breastfeeding. The patients exposed to chemotherapy did not report problems in exclusively breastfeeding but rather in the initiation of breast milk production postpartum. From the beginning, milk production was subjectively decreased or not produced at all by patients exposed to chemotherapy. Exclusivity implies that there is some milk production initially, but this is not what was reported by patients exposed to chemotherapy during pregnancy. These women can be forewarned of this possibility to alleviate distress and may benefit from additional lactational support. Cautiously warning pregnant women treated for cancer during pregnancy of this possible effect of treatment during pregnancy will help alleviate additional distress if exclusively breastfeeding is unsuccessful.
Footnotes
Acknowledgments
The authors thank Candy Beach and Elizabeth Hoover for their help in data collection and documentation. This article would not have been possible without the help of John Gaughan for statistical analysis. Sources of support: The Teal Tea Foundation and the Cooper Foundation are acknowledged for their continued financial support for the Cancer and Pregnancy Registry database.
Disclosure Statement
No competing financial interests exist.