
Abstract
Abstract
Background:
In-hospital experiences among women with gestational diabetes mellitus (GDM) could impact breastfeeding success. We sought (1) to determine changes in the prevalence of hospital breastfeeding experiences between 2004–2008 and 2009–2011 among women with GDM and women without diabetes; (2) to determine whether GDM is associated with higher occurrence of experiencing Baby-Friendly hospital practices because of their known higher rates of breastfeeding difficulties.
Materials and Methods:
Data from the 2004 to 2011 Pregnancy Risk Assessment Monitoring System, a survey of women with a recent live birth from 16 states and New York City, were used based on inclusion of an optional survey question about hospital breastfeeding experiences. We examined the association of in-hospital experiences with GDM within each survey phase using chi-square tests. Weighted multivariable logistic regression was used to determine the association between GDM and hospital breastfeeding experiences.
Results:
Among 157,187 (8.8% GDM), there were crude differences by GDM status for at least 60% of hospital experiences despite increases in positive hospital experiences between time periods. Women with GDM were less likely to report breastfeeding in the first hour (adjusted odds ratio: 0.83, confidence interval [95% CI] 0.73–0.94), feeding only breast milk in the hospital (0.73, 0.65–0.82), and feeding on demand (0.86, 0.74–0.99) compared with women without diabetes. Women with GDM were significantly more likely to report receiving a pump (1.28, 1.07–1.53) and a formula gift pack (1.17, 1.03–1.34) compared with women without diabetes.
Conclusions:
Although women with GDM experienced improvements in-hospital breastfeeding experiences over time, disparities in breastfeeding practices remained for five in-patient (hospital) practices that included four negative practices (breastfeeding in the first hour, feeding only breast milk in the hospital, told to feed per mother's preference, receiving a formula gift pack) and one positive practice (receiving a pump).
Introduction
B
A recent meta-analysis found that implementation of the BFHI increased exclusive breastfeeding by 49% (confidence interval [95% CI], 33%–68%) and any breastfeeding by 66% (95% CI, 34%–107%). 2 Additionally, BFHI and its elements of hospital support increased the proportion of women breastfeeding in the first hour (relative risk = 1.11; 95% CI, 1.06–1.16), breastfeeding exclusively in the first 5 months (relative risk = 1.46; 95% CI, 1.37–1.56), and any breastfeeding in the first 6 months (relative risk = 1.40; 95% CI, 1.30–1.52). 2
Although the long-term beneficial health effects of breastfeeding for infants are well known, lasting maternal health benefits of lactation among women with prior gestational diabetes mellitus (GDM) have recently been supported by more rigorous prospective evidence. Specifically, higher lactation intensity and longer duration are associated with lower 2-year incidence of type 2 diabetes mellitus (T2DM) after GDM pregnancy. 3 Considering women with prior GDM are seven times more likely to develop T2DM over their lifetime compared to women without the same history, 4 interventions aimed at modifying lactation behaviors, including through improving hospital breastfeeding experiences, may be a practical, timely, and low-cost approach to increase breastfeeding and ultimately prevent T2DM among women with GDM. 3
Women with GDM are more likely to be obese and have an increased risk of perinatal complications than women without GDM, both of which are associated with formula use during the hospital stay.5,6 Considering early formula use leads to shorter breastfeeding durations, 7 breastfeeding education and support experiences in the hospital could be an important modifiable factor to improve breastfeeding outcomes. Thus, this study had two objectives: (1) to determine changes in the prevalence of specific types of hospital breastfeeding experiences between 2004–2008 and 2009–2011 among women with GDM and women without diabetes; and (2) to determine whether GDM are more likely to experience Baby-Friendly hospital practices because of their known higher rates of breastfeeding difficulties.
Materials and Methods
The Pregnancy Risk Assessment Monitoring System (PRAMS) collected population-based data on self-reported maternal behaviors and experiences before, during, and after pregnancy among women who have had a recent live birth. 8 A stratified systematic sampling method is used to over-sample mothers with adverse birth outcomes and racial/ethnic minority groups 2 to 6 months after giving birth from a frame of state's birth certificate files. The PRAMS questionnaire includes core questions that are asked by all states and standard questions that states can choose. In Phase 5 (2004–2008), 10 states (Colorado, Florida, Illinois, Louisiana, Maine, Missouri, Nebraska, Oregon, Vermont, West Virginia) and New York City and in Phase 6 (2009–2011), 12 states (Colorado, Maine, Nebraska, Oregon, Vermont, West Virginia, Alaska, Arkansas, Minnesota, New Jersey, New York, Texas) and New York City chose to include an optional survey question about hospital breastfeeding experiences. Among women who answered yes to “Did you ever breastfeed or pump breast milk to feed your new baby after delivery?,” the optional question they went on to answer:
“This question asks about things that may have happened at the hospital where your new baby was born. For each item, circle Y (Yes) if it happened or circle N (No) if it did not happen.”
a. Hospital staff gave me information about breastfeeding.
b. My baby stayed in the same room with me at the hospital.
c. I breastfed my baby in the hospital.
d. I breastfed my baby in the first hour after my baby was born.
e. Hospital staff helped me learn how to breastfeed.
f. My baby was fed only breast milk at the hospital.
g. Hospital staff told me to breastfeed whenever my baby wanted.
h. The hospital gave me a breast pump to use (asked only in Phase 6).
i. The hospital gave me a gift pack with formula.
j. The hospital gave me a telephone number to call for help with breastfeeding.
k. My baby used a pacifier in the hospital.
Further details of PRAMS methods are described elsewhere. 9
In Phase 5 (2004–2008) self-reported GDM was obtained by asking women whether they had “High blood sugar (diabetes) that started during this pregnancy”; self-reported prepregnancy diabetes was obtained by asking women if they had “High blood sugar (diabetes) that started before this pregnancy.” In Phase 6 (2009–2011) self-reported GDM was obtained by the response to the question “During your most recent pregnancy, were you told by a doctor, nurse, or other healthcare worker that you had gestational diabetes (diabetes that started during this pregnancy)?”; self-reported prepregnancy diabetes was based on responses to the question “Before you got pregnant with your new baby, were you ever told by a doctor, nurse, or other healthcare worker that you had type 1 or type 2 diabetes (This is not the same as gestational diabetes or diabetes that starts during pregnancy)?.” Previous work indicates GDM prevalence from PRAMS shows >94% agreement with GDM reported on the birth certificate.10,11 Women reporting prepregnancy diabetes were excluded (n = 2,260), as were women with missing data on prepregnancy diabetes or/and GDM (n = 3,196) (Fig. 1). Women with both prepregnancy diabetes and GDM were not counted as GDM in this study (n = 984) (Fig. 1), and were excluded from analyses. 11 Thus, women with GDM were compared with women without GDM or prepregnancy diabetes, herein referred to as women without diabetes.
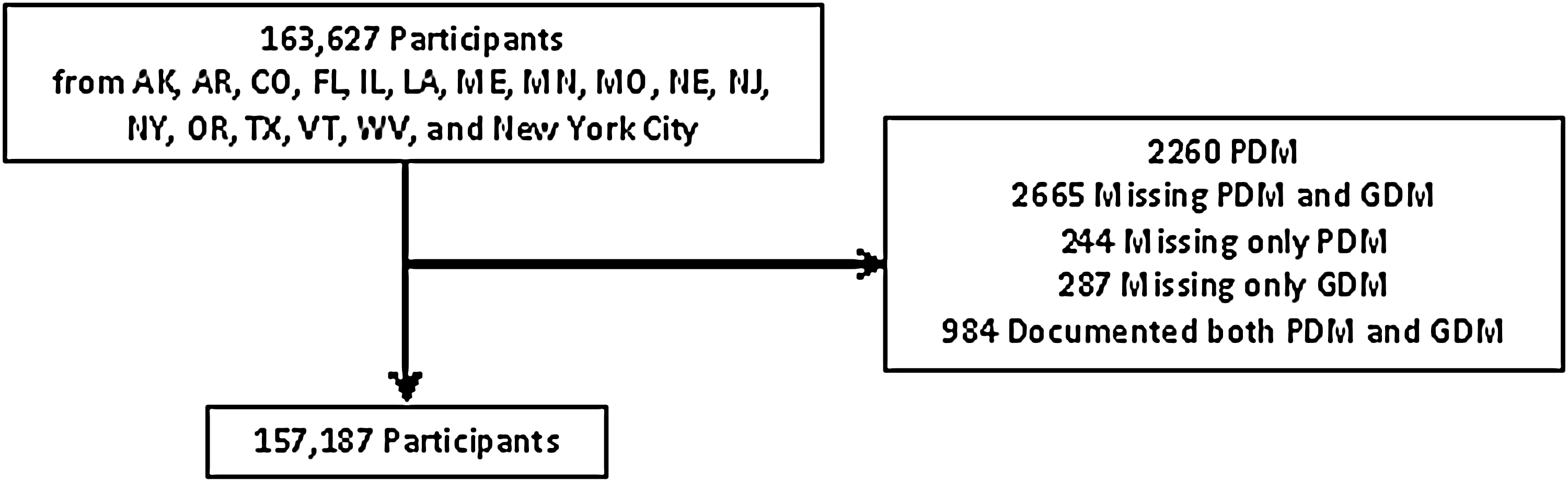
Subject flow diagram. PDM, prepregnancy diabetes mellitus; GDM, gestational diabetes mellitus.
The associations of categorical variables with GDM status were evaluated using the chi-square test of independence: maternal age (≤19, 20–24, 25–29, 30–34, ≥35 years), maternal race/ethnicity (non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, non-Hispanic Other, Hispanic), maternal education (<12, 12, >12 years), marital status (married, other), prepregnancy insurance status (Medicaid [no private], other insurance), prepregnancy body mass index (BMI: <18.5, 18.5–24.9, 25–29.9, ≥30 kg/m2), parity (no previous live births, one or more previous live birth [s]), mode of delivery (cesarean section or vaginal), gestational age (<37 weeks [preterm], or >37 weeks [term]), pregnancy intention, neonatal intensive care unit (NICU) admission, multiple birth (singletons or multiples), and ever breastfed or pumped milk after delivery.
For the first objective, we examined the association of in-hospital experiences with GDM status within each survey phase using the chi-square test of independence. Hospital practices corresponding to questions d–k above were restricted to only those women who responded yes to “I breastfed my baby in the hospital.” For the second objective, weighted multivariable logistic regression was used to determine the association between GDM and each of the hospital breastfeeding experiences by combining the data across both Phases. Adjusted models included variables associated with GDM in the descriptive analyses (p < 0.05) to estimate the adjusted odds ratios (ORs) for the hospital practice. Collinearity was assessed among the variables included in each model. Potential confounders met the criteria of independent association with the exposure and the dependent outcome based on p-values and alteration in the ORs by at least 10%. Data were analyzed using survey procedures in SAS version 9.3 (SAS Institute, Research Triangle Park, NC). This study was deemed exempt by the Nationwide Children's Hospital Institutional Review Board. All significance tests were one-sided and criteria based on p < 0.05.
Results
The dataset included 157,187 respondent mothers from both Phases combined, 8.8% with GDM. Characteristics of respondents and comparisons by GDM are listed in Table 1. Maternal age, maternal race, maternal education, Medicaid status, prepregnancy BMI, parity, mode of delivery, gestational age, pregnancy intention, NICU admission, and proportion of women delivering multiples differed among those with GDM and no diabetes.
Based on 2004–2011 data from AK, AR, CO, FL, IL, LA, ME, MN, MO, NE, NJ, NY, OR, TX, VT, WV, and New York City. All sample sizes and percentages are based on weighted sample distributions to account for survey design; p-value is from the chi-square test of independence between GDM category and the characteristics. Missing values: maternal age (6), race (9,952), education (1,539), married (84), Medicaid (488), prepregnancy BMI (8,445), primiparous (449), mode of delivery (518), gestational age (1,055), intended pregnancy (2,347), NICU admission (2,012), multiples (8,556), ever breastfed or pumped milk (5,049).
BMI, body mass index; GDM, gestational diabetes mellitus; NICU, neonatal intensive care unit; SE, standard error.
In both Phases, there were crude differences by GDM status for at least 60% of hospital experiences (Table 2). In Phase 5 (Table 2), compared to women without diabetes, women with GDM were significantly less likely to report their baby staying in the same room (73.6% versus 78.3%, p < 0.0001), breastfeeding in the hospital (this does not include pumping) (73.0% versus 75.7%, p = 0.01), breastfeeding in the first hour (55.7% versus 65.5%, p < 0.0001), hospital staff helping (80.0% versus 82.5%, p = 0.03), feeding only breast milk in the hospital (41.0% versus 52.4%, p < 0.0001), and feeding on demand (81.2% versus 83.6%, p = 0.04). In both women with GDM and women without diabetes, the prevalence of reporting positive hospital experiences universally increased from Phase 5 to Phase 6, but disparities among women with GDM persisted. Specifically, in Phase 6, compared with women without diabetes, women with GDM still were significantly less likely to report their baby staying in the same room (77.8% versus 81.8%, p = 0.003), breastfeeding in the hospital (this does not include pumping) (88.2% versus 91.9%, p < 0.01), breastfeeding in the first hour (60.2% versus 68.6%, p < 0.0001), and feeding only breast milk in the hospital (39.4% versus 52.7%, p < 0.0001). New differences emerged in Phase 6 compared with Phase 5 including fewer women with GDM reporting the hospital providing a phone number for breastfeeding help (81.6% versus 84.6%, p = 0.03) and more women with GDM reporting receiving a pump (39.5% versus 31.8%, p < 0.0001) and a formula gift pack (71.0% versus 65.9%, p = 0.002) compared with women without diabetes.
Based on 2004–2011 data from AK, AR, CO, FL, IL, LA, ME, MN, MO, NE, NJ, NY, OR, TX, VT, WV, and New York City. All sample sizes and percentages are based on unadjusted, weighted sample distributions to account for survey design; p-value is from the chi-square test of independence between GDM category and the experiences.
Restricted to women who responded they ever breastfed in the hospital.
Because the prevalence estimates shown in Table 2 were for the entire sample, including those who may experience adverse delivery outcomes that disproportionately impacts women with GDM (Table 1), we evaluated collinearity and potential confounding. We found no evidence of collinearity among the variables included in the models. Addition of the confounders had minimal impact of the ORs (Table 3). Specifically, women with GDM were less likely to report breastfeeding in the first hour (adjusted OR: 0.83, 95% CI 0.73–0.94), feeding only breast milk in the hospital (0.73, 0.65–0.82), and feeding on demand (0.86, 0.74–0.99) compared with women without diabetes. Women with GDM were significantly more likely to report receiving a pump (1.28, 1.07–1.53) and a formula gift pack (1.17, 1.03–1.34) compared with women without diabetes. Baby staying in the same room, breastfeeding in the hospital (this does not include pumping), and hospital providing a phone number for breastfeeding help were no longer significant in adjusted analyses.
Based on 2004–2011 data from AK, AR, CO, FL, IL, LA, ME, MN, MO, NE, NJ, NY, OR, TX, VT, WV, and New York City. Survey years were combined; Adjusted for maternal age, maternal race, maternal education, Medicaid, prepregnancy BMI, parity, mode of delivery, gestational age, intended pregnancy, neonatal intensive care unit admission, multiples, year.
Bold values indicate p < 0.05.
Restricted to women who responded they ever breastfed in the hospital.
CI, confidence interval; OR, odds ratio.
Discussion
In this large, population-based study representing almost 7 million women, we found that although women with GDM experienced improvements in in-hospital breastfeeding experiences over time, they were more likely to report four negative in-hospital practices (breastfeeding in the first hour, feeding only breast milk in the hospital, told to feed per mother's preference, receiving a formula gift pack) and one positive practice (receiving a pump). Even after adjusting for multiple confounding variables, women with GDM were 17% significantly less likely to report breastfeeding in the first hour, 27% less likely to feed only breast milk in the hospital, and 17% more likely to receive a formula gift pack than women without diabetes. These differences are particularly relevant considering each of these practices independently have been significantly associated with effects on breastfeeding outcomes,12–15 and can prevent GDM women from achieving optimal breastfeeding outcomes. Greater severity of obesity among women with GDM may also contribute to the negative hospital practices, despite controlling for maternal BMI.
Increases in the proportions of women reporting positive hospital breastfeeding experiences between the two phases may be due to a small increase in the number of BFHI designated hospitals in the states included in the analysis. 16 However, current U.S. maternity care practices do not universally include all 10 BFHI steps, and the level to which individual hospitals implement any, some, or all steps may vary widely, which may contribute to the observed disparities by GDM. Additionally, the years included reflect a period of improved breastfeeding initiation rates, 16 which may be related to increased breastfeeding awareness among women, providers, and health systems, along with increased lactation consultant availability. This is encouraging considering breastfeeding success in the early postpartum period increases breastfeeding self-efficacy in the late postpartum period. 17 Breastfeeding self-efficacy early in the postpartum period appears to be particularly important to decrease risk of delayed breastfeeding initiation and to lower risk of perceived delayed lactogenesis, 18 commonly cited issues among women with GDM.
Early breastfeeding is correlated with increased duration of breastfeeding. 19 Because women with GDM are more likely to experience cesarean sections or intrapartum complications and/or have their infants admitted to the NICU, 7 these women are at increased risk for separation from their infants after delivery, resulting in delayed contact and as seen in this study, reduced odds of breastfeeding in the first hour. This can result in delayed onset of milk production, independent of any physiology, and may lead to greater weight loss during the first 3 days of life. 20 This cascade of events triggered by early separation, leads to the “medical” indications for in-hospital supplementation, which in turn reduces breastfeeding duration. 12
Our findings that infants of women with GDM are less likely to receive only breast milk in the hospital are consistent with previous literature.5,6 In-hospital supplementation is of concern as multiple studies document that formula supplements during delivery stay are associated with shortened durations of both exclusive21,22 and any breastfeeding.1,23 Although the most common reasons for in-hospital supplementation disproportionately affect infants of women with GDM (delayed lactation, 24 perceived low milk supply, 25 disrupted mother–infant interaction due to cesarean section 7 or neonatal intensive care unit admission, 7 inhibited infant suckling, 26 hypoglycemia, 27 neonatal weight loss, 28 jaundice 28 ), the actual need for supplementation for these infants is not as clear as it is for other infants (e.g., preterm or low birth weight infants). Thus, clear hospital policies regarding supplementation including specifics on appropriate conditions for supplementation, type of supplement, and amount to supplement 21 are needed to avoid unnecessary hospital supplementation and preserve breastfeeding 21 via appropriate education and support. However, mothers may not know that they have choices with regard to formula introduction during hospital stay and/or may not know that formula use can and should be temporary. 29
Both the hospital staff perceptions of the need for formula 30 and/or preconceived viewpoints about breastfeeding difficulty among women with GDM or obese women, 7 would likely be associated with women with GDM being more likely to receive a formula gift pack. In addition to the hospital policy issues mentioned above, distribution of formula gift packs should be reassessed, particularly for those women with GDM who do not require supplements in the hospital or do not express intention to formula feed.
Women with GDM in this study were more likely to report receiving a breast pump from the hospital than women without diabetes. Receiving a pump can be a positive breastfeeding practice because it suggests that the mother and/or hospital staff are trying to ensure the infant receives human milk. Alternately, this may represent an attempt to enhance milk production, particularly during mother-infant separation or perceived low milk supply. Furthermore, delayed lactogenesis is somewhat more common among women with GDM, 31 and early pumping can facilitate milk production. 32 Interestingly, there was about a 5% difference, regardless of GDM status, between women who said they ever breastfed or pumped breast milk, but did not breastfeed in the hospital, indicating that a small proportion of women only pumped during their hospital stay even after adjusting for conditions that might impair direct breastfeeding. We previously showed that women with GDM initiated pumping significantly sooner than women without diabetes (median 3 versus 7 days after delivery), which did not impact pumping duration. 5 However, we also showed that women with GDM engage in shorter durations of at-the-breast feeding. 5 Pumping is certainly a good strategy to address milk production issues and is recommended for at-risk mothers,33,34 but not a specific step in the BFHI. Moreover, pumping should not deter from at-the-breast feeding since both strategies can and should be used to maintain and increase milk supply, particularly for women with reported difficulty producing enough milk. 32 The data used in this study predate the Affordable Care Act (ACA) which, beginning in August 2012, included coverage for breastfeeding supplies such as breast pumps. Before the ACA, insurance coverage for breast pumps was much more variable, strengthening the differences observed in this study.
This study had some limitations. The data included in this study were from 16 states and New York City and thus may not be generalizable to the rest of the country. Additionally, there is variation in breastfeeding practices between facilities, 35 and although we adjusted for state in our analyses, we could not adjust for individual hospitals. It is possible that women with GDM were differentially distributed among hospitals offering different levels of breastfeeding practices. The survey did not include data on all 10 BFHI steps (data on steps 1, 2, and 10 were not asked). Considering <20% of hospitals in the United States have the BFHI designation we do not anticipate these steps would have had much of an impact on the reported maternal experiences. Furthermore, this work is observational and the possibility of reverse causality, whereby women with GDM may be less likely to seek out breastfeeding help than women with diabetes, should be considered. Breastfeeding intention is an optional question in PRAMS, and was asked only in one state included in the analysis (NY) with 2 years of available data, thus could not be assessed as a potential confounder. PRAMS also has limited data on maternity leave and employment, which could also impact breastfeeding but could not be assessed. The respondents included in this study may differ from those who were excluded: PRAMS excludes women who had stillbirths or fetal deaths, which may be associated with GDM. 36 Our estimates are based on administrative and self-report data and are therefore subject to reporting biases. For example, GDM prevalence is very sensitive to the diagnostic criteria used. In recent years criteria have changed and there has been a lack of consensus about which criteria to use. 37 During our study period it is likely that a mix of these criteria was used, but the survey does not ascertain which criteria were used for GDM diagnoses. Lastly, ∼10% of respondents with missing data were excluded. Analytical guidelines for PRAMS suggest that 25% or more missing data may not accurately represent the population; our levels are well below this cutoff, suggesting the missing data likely did not bias our results. 38 Although PRAMS was not designed to be nationally representative, it represents over 75% of live births in the United States and oversampled specific, high-risk populations to maximize generalizability. 8
This study also offers several strengths. The survey included questions regarding hospital practices beyond the 10 BFHI steps, which can serve as additional points of intervention beyond BFHI. Our analysis included more states and more years than previous related work, which did not consider GDM, even as a covariate. 39
Conclusion
We identified five hospital practices with disparities for breastfeeding among women with GDM: four negative practices (breastfeeding in the first hour, feeding only breast milk in the hospital, told to feed per mother's preference, and receiving a formula gift pack) and one positive practice (receiving a pump). The negative practices may be corrected through effective implementation of specific BFHI steps such as minimizing separation between mother and baby by making “rooming in” possible 24/7, and ensuring adequate support from hospital staff on helping women initiate breastfeeding within 1 hour of birth and learning how to anticipate and manage common breastfeeding problems during the maternity stay. 30 Hospitals are starting to implement steps individually, which can also be beneficial for improving outcomes.40,41 Although in-hospital practices that support breastfeeding are certainly important, they alone are not sufficient for ensuring women who desire to breastfeed can achieve their breastfeeding potential. 42 The establishment of a trusting relationship with a healthcare provider has been shown to be key to improving women's sense of self-efficacy, emphasizing the important role lactation consultants, pediatricians, obstetricians, and other healthcare providers can play in helping women successfully establish early breastfeeding.30,43 Improvements in workplace policies and extended paid maternity leave are essential to reach the Healthy People 2020 objective for continued breastfeeding. 44
Footnotes
Acknowledgments
We thank the PRAMS working group: Alabama—Izza Afgan, MPH; Alaska—Kathy Perham-Hester, MS, MPH; Arkansas—Mary McGehee, PhD; Colorado—Alyson Shupe, PhD; Connecticut—Jennifer Morin, MPH; Delaware—George Yocher, MS; Florida—Avalon Adams-Thames, MPH, CHES; Georgia—Chinelo Ogbuanu, MD, MPH, PhD; Hawaii—Emily Roberson, MPH; Illinois—Theresa Sandidge, MA; Iowa—Sarah Mauch, MPH; Louisiana—Amy Zapata, MPH; Maine—Tom Patenaude, MPH; Maryland—Diana Cheng, MD; Massachusetts—Emily Lu, MPH; Michigan—Cristin Larder, MS; Minnesota—Judy Punyko, PhD, MPH; Mississippi—Brenda Hughes, MPPA; Missouri—Venkata Garikapaty, MSc, MS, PhD, MPH; Montana—JoAnn Dotson; Nebraska—Brenda Coufal; New Hampshire—David J. Laflamme, PhD, MPH; New Jersey—Lakota Kruse, MD; New Mexico—Eirian Coronado, MPH; New York State—Anne Radigan-Garcia; New York City—Candace Mulready-Ward, MPH; North Carolina—Kathleen Jones-Vessey, MS; North Dakota—Sandra Anseth; Ohio—Connie Geidenberger, PhD; Oklahoma—Alicia Lincoln, MSW, MSPH; Oregon—Kenneth Rosenberg, MD, MPH; Pennsylvania—Tony Norwood; Rhode Island—Sam Viner-Brown, PhD; South Carolina—Mike Smith, MSPH; Texas—Rochelle Kingsley, MPH; Tennessee—David Law, PhD; Utah—Lynsey Gammon, MPH; Vermont—Peggy Brozicevic; Virginia—Marilyn Wenner; Washington—Linda Lohdefinck; West Virginia—Melissa Baker, MA; Wisconsin—Katherine Kvale, PhD; Wyoming—Amy Spieker, MPH; CDC PRAMS Team, Applied Sciences Branch, Division of Reproductive Health.
Disclosure Statement
No competing financial interests exist.