
Abstract
Abstract
Purpose:
Lactation often affects calcium metabolism and induces bone loss. Calcium supplementation and a high calcium diet are recommended to prevent bone loss, especially during inadequate calcium intake. Our study aimed at determining bone loss in breastfeeding mothers, and if it occurred, whether it was site specific and there were correlations between serum bone turnover markers.
Materials and Methods:
Since the 6-month exclusive breastfeeding is usually recommended in several countries, our study examined bone mineral density (BMD) in early (1–2 month), mid (3–4 month)-, and late (5–6 month) lactation compared with nonpregnant, nonlactating control women. Site-specific bone loss was monitored in lumbar vertebrae and femora. Bone turnover markers, that is, C-terminal telopeptide of type 1 collagen and N-terminal propeptide of type 1 collagen (P1NP), were determined by electrochemiluminescence immunoassays.
Results:
The onset of bone loss in exclusive breastfeeding mothers was site specific, for example, in the lumbar bone at mid-lactation and in the femoral bone in late lactation. Serum ionized calcium levels in late lactation were lower than the normal levels. In addition, a correlation was found between bone turnover marker, P1NP, and femoral BMD.
Conclusions:
The onset of bone loss in exclusive breastfeeding mothers was site specific, and the lumbar bone was a vulnerable and perhaps better representative site for bone loss detection. It was suggested that the optimal starting time for calcium supplementation should be before the mid-lactation when the bone loss was observed. In addition, the biochemical marker that best predicted the onset of bone loss in lactating women was P1NP.
Introduction
D
Recent investigation in rats showed that pre-suckling calcium supplementation in divided doses is more effective than a daily single dose in preventing lactation-induced osteopenia. 5 However, it is not known whether a similar supplementation regime would be effective or practical for breastfeeding mothers, especially in early lactation when mothers are still adapting to new routines, with the newborn babies as their first priority. Besides, if an effective calcium supplement program, in terms of dosage, timing, and frequency of supplementation, were to be designed, it would be necessary to know when the onset of bone loss generally occurs in nursing mothers and which skeletal site is the prime indicator of early bone loss.
In the clinical assessment, biochemical markers of bone turnover, such as C-terminal telopeptide of type 1 collagen (CTx) and N-terminal propeptide of type 1 collagen (P1NP), are usually determined together with bone mineral density (BMD). Carneiro et al. reported that PN1P and CTx levels in lactating women were significantly higher than those in nonlactating women.9,10 Although CTx has been proposed as a potential biochemical marker for early state of bone loss in postmenopausal women, 11 there has been no investigation on the correlation between biomarkers and bone mass in lactating women.
Besides calcium, other minerals, for example, phosphate and magnesium, which contribute to the maintenance of normal bone strength, are also required for milk production.12,13 Iron is another mineral of considerable importance because deficiency and anemia are commonly reported in pregnant and lactating women.14–16 A previous investigation showed that iron deficiency in rats led to poorly mineralized bone and microstructural bone defects. 17 Therefore, to address the issue of effectiveness of calcium supplementation in the prevention of bone loss in lactating women, the study must be carried out in breastfeeding mothers free of iron deficiency or overt anemia.
Therefore, the main objectives of this study were to study whether bone loss occurred exclusively in breastfeeding mothers with a normal mineral status, and if it occurred, whether it was site specific; the second objective was to see whether there were correlations between serum bone turnover markers during the entire lactating period.
Materials and Methods
Volunteers
Sample collections were conducted at the Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand. The volunteers were divided into four groups: (1) nonpregnant nonlactating women (control), (2) early (1–2 month), (3) mid (3–4 month)-, and (4) late (5–6 month) lactating women for the BMD study. Blood samples were collected from the three phases of lactation (Groups 2–4) for the bone turnover marker study (Fig. 1). Body weight, height, congenital diseases, history of diseases relevant to bone metabolism, drugs, calcium diet, and calcium supplementation were recorded. The inclusion criteria included healthy volunteers aged between 18 and 35 years with a body mass index (BMI) within the normal range (18.5–24.9 kg/m2). The exclusion criteria included a history of diseases affecting bone metabolism, that is, inflammatory rheumatic diseases, inflammatory bowel disease, hepatic or renal diseases, hyperthyroidism, hyperparathyroidism, type 1 diabetes, malignancy, or any bone metabolism disorder. This study was approved by the ethics committee of Siriraj Hospital [515/2556(EC2)]. Written informed consent was obtained from each patient before sample collection.
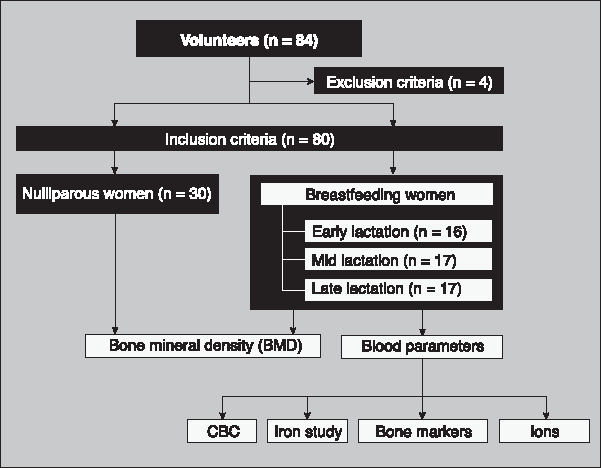
Flowchart for study population selection and experimental design. BMD, bone mineral density; CBC, complete blood count.
BMD measurement
BMD of control and lactating women was measured by using a bone densitometer (Lunar Prodigy DF +15974; GE Healthcare, Madison, WI) by well-trained technicians at Siriraj Hospital.
Blood sample collection and complete blood count, serum ions, and bone markers measurement
Blood samples were collected by a registered nurse, and all blood parameters were measured by technicians at the Central laboratory, Department of Clinical Pathology, Siriraj Hospital. Complete blood count (CBC) was evaluated by an automated hematology analyzer (Sysmex XN-3000, Kobe, Japan or Coulter LH 780; Beckman Coulter, Brea, CA). Serum ion concentrations (i.e., total calcium, phosphorus, and magnesium) were measured by using a photometric method (Cobas 8000, c 702; Roche Diagnostics, Indianapolis, IN). Ionized calcium was evaluated by an RAPIDLab 348EX Blood Gas System (Siemens Healthcare, Erlangen, Germany). Serum ion levels were measured by an automated colorimetric method system (BioSystems A15, Barcelona, Spain). Bone turnover markers, that is, P1NP and CTx, were determined by an electrochemiluminescence immunoassay method (Cobas 8000, e 602; Roche Diagnostics).
Statistical analyses
The results are expressed as means ± standard error. Comparisons between the two sets of data were performed by using an unpaired t test. Correlation analysis was performed to evaluate the relationship between bone markers and BMD by Pearson correlation coefficient. Results were considered significantly different when p < 0.05. All tests were analyzed by GraphPad Prism 6.0 (GraphPad Software, Inc., San Diego, CA).
Results
Characteristics of population, CBC, and blood chemistry changes during lactation
Eighty women were included in this study after four volunteers were excluded due to their BMI being higher than the inclusion criteria (Fig. 1). The included volunteers were aged between 18 and 35 years, with averages of ∼26 to 29 years for all groups. We found that BMI in the early lactating group (21.54 ± 0.49) was significantly higher than that in the control group (24.79 ± 1.11; p < 0.05).
Blood parameters, that is, hemoglobin, hematocrit, red blood cell count, mean corpuscular hemoglobin concentration, and red cell distribution width, in three groups of lactating women were at normal levels. However, mean corpuscular volume was lower in the early lactating group than the normal levels, whereas C-reactive protein level in the late lactating group was higher than the normal levels (Table 1).
Data are presented as mean ± SE. Bold values indicate the levels outside the normal range.
CTx, C-terminal telopeptide of type 1 collagen; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; P1NP, N-terminal propeptide of type 1 procollagen; RBC, red blood cell; RDW, red cell distribution width; SE, standard error; TIBC, total iron-binding capacity.
Serum levels of ions, that is, total calcium, phosphorus, magnesium, and iron, were within the normal ranges, except for ionized calcium, which was at a borderline level in the early and mid-lactating groups and lower than the normal level in the late lactating group. In addition, an iron study showed that transferrin, ferritin, total iron-binding capacity, and transferrin saturation in three phases of lactation were normal, except for lower transferrin saturation in late lactating women (Table 1).
BMD in early, mid-, and late lactating groups
According to the World Health Organization (WHO), T-score and Z-score, known indicators of osteopenia and osteoporosis, are the standard deviations of a volunteer's BMD as compared with the standard BMD of reference mean in young normal and age-matched normal groups, respectively. Although the average T-score and Z-score of all lactating groups were in the normal range (≥1; WHO classification) (Table 2), BMD of the lumbar spine (L) 1–4 in the mid- and late lactating groups was significantly lower than that of the control group (Fig. 2A). For site-specific measurement of the lumbar, only L1 of the late lactating group showed a significantly lower BMD than the control (Fig. 2B). Moreover, total femoral BMD was also significantly lower in the late lactating group than the control group (Fig. 2C). A site-specific measurement further showed that BMD in wards, trochanter, and shaft of femurs of the late lactating women was significantly lower than that of the control group, whereas BMD of the femoral neck only showed a tendency to be lower (Fig. 2D). It was noted that the late lactating group had a lower BMD in the lumbar and femur than the other two lactating groups, though not significantly different.
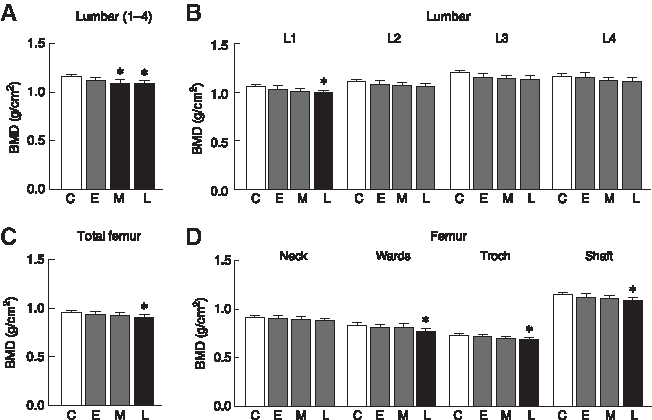
BMD of lumbar (L) 1–4
Data are presented as mean ± SE.
Bone turnover markers and correlation with BMD
Interestingly, P1NP and CTx levels were markedly higher than the normal levels in all three lactating groups, but no significant difference was observed among the three groups. In addition, the highest ratio between these two biomarkers was found in the late lactating group (Table 1). Furthermore, there was a strong positive correlation between these two markers (r = 0.73, p < 0.001; Fig. 3A). Lumbar BMD did not show a correlation with P1NP or CTx (data not shown), whereas BMD of the total femur and the trochanteric part of the femur in all lactating women was negatively correlated with P1NP but not CTx (Fig. 3B–E).
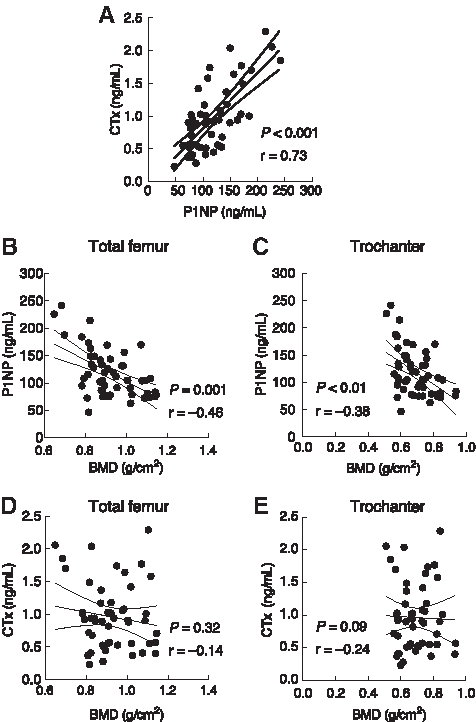
Correlation between serum P1NP and CTx levels in lactating women
Discussion
In this study, we determined whether lower BMD still occurred in calcium-replete breastfeeding Asian women. Although T-score ≤1 was not seen in any lactating groups, we found that BMD of the lactating groups was lower than that of the nonpregnant, nonlactating control women. Low BMD at L1–4 was first detected in the third to fourth month postpartum (mid lactation), whereas low BMD in the total femur, wards, trochanter, and shaft of femur occurred in the fifth to sixth month postpartum (late lactation). Although BMD at the femoral neck of the lactating groups was lower than the control group, the difference was not significant. Our results were consistent with previous reports of decreased lumbar BMD at the third month postpartum for lactating women. 4 For other sites of bone, Chan et al. reported that in addition to L2–4, BMD of the trochanter and femoral neck was also decreased at the third month for Hong Kong Chinese lactating women. 1 It was apparent that the onset of low BMD was between the third and sixth month postpartum depending on the skeletal sites. Based on the present finding, low BMD still occurred in calcium-replete lactating mothers, and calcium supplementation for breastfeeding mothers can be started after the first month postpartum.
In contrast to the present finding, Yumusakhuylu et al. did not find a decrease in BMD at the mid-tibial shaft of lactating women by using quantitative ultrasonometry. 18 Similarly, Cross et al. found no change in the BMD of radius bone in lactating women during the third month when compared with nonpregnant, nonlactating women. 2 These reports together with our finding indicated that bone loss in lactating women was site specific. From a practical point of view, it was important to indicate the representative site for bone loss detection in lactating women. Moreover, the site-specific bone change was able to explain why some studies did not show bone loss during lactation.
The cause of lactation-induced bone loss was likely to be multifactorial, particularly related to an elevation of some hormones, such as prolactin and PTHrP.5–7 Since prolactin has been shown to directly induce bone resorption, 19 high circulating levels of prolactin during lactation, together with inadequate calcium intake probably play a major role in bone loss in breastfeeding mothers. 20 However, either calcium deficiency or a low intake of certain minerals (e.g., iron) could not explain low BMD in our volunteers, as we excluded individuals with a history of calcium inadequacy from the study. Serum mineral concentrations in the present lactating women were in the normal range, except for a decrease in ionized calcium in late lactation. Previous studies by Chan et al. 21 and Krebs et al. 4 also reported normal serum calcium, phosphorus, and magnesium in lactating women, but ionized calcium level was not determined in their studies. In contrast, Cross et al. found slightly higher calcium levels in 3-month lactating women than nonpregnant, nonlactating women. 2 This body of evidence implied that bone loss in lactating women could occur regardless of serum calcium and was unlikely to result from other mineral deficiency. In other words, serum mineral levels, especially total serum calcium, were not appropriate to represent or indicate low BMD in breastfeeding mothers.
Basically, bone loss is caused by an imbalanced bone turnover. Several studies have shown that P1NP and CTx are potential biochemical markers for bone turnover and are used to determine changes in BMD.11,22 In this study, serum P1NP and CTx levels in the three lactating groups were markedly higher than the normal levels and exhibited a strong positive correlation between themselves, confirming that an increase in bone turnover occurred during lactation. Indeed, higher levels of P1NP and CTx were previously associated with high bone turnover in lactating women9,10,23 and bone loss in other conditions such as thalassemia-induced bone loss or even healthy women without any conditions affecting bone turnover, who showed a positive correlation of these two markers.22,24 A negative correlation was found only between P1NP and BMD of the total femur and trochanteric part of the femur, and no correlation was observed for CTx in our study. Similarly, elderly women who had a high risk of osteoporosis exhibited a negative correlation between total BMD and P1NP1. 25 Marques et al. demonstrated in the elderly (age 76 ± 5.5) that there was a weak negative correlation between BMD of the lumbar spine and femoral neck and bone turnover markers (P1NP and CTx). 26 Further investigation is required to investigate the underlying cellular mechanism that helps explain the negative correlation between BMD and bone turnover markers.
Regarding the limitation of the present study, since BMD was determined in a cross-sectional fashion rather than a longitudinal fashion, a variation due to a different population cannot be ruled out. In other words, the time-dependent changes in BMD might result from a developing biological process, a different population tested in each group, or a combination of both.
In conclusion, the onset of bone loss in exclusive breastfeeding mothers was site specific, that is, in the lumbar bone at mid (3–4 months postdelivery)-lactation and in the femoral bone at late lactation (5–6 months postdelivery). Interestingly, low BMD was observed, even though all volunteers had no history of low calcium intake, low iron intake, or iron deficiency. Moreover, the biochemical marker that best predicted the early onset of bone loss in lactating women was P1NP, but not CTx or total serum calcium.
Footnotes
Acknowledgments
The authors thank Prof. Nateetip Krishnamra for proofreading and critical comments on this article. This study was supported by grants from the Cluster and Program Management Office (CPMO), the National Science and Technology Development Agency (P-13-00100), Mahidol University (to N.C.), and the Thailand Research Fund (TRF)—Mahidol University through the TRF Senior Research Scholar Grant (RTA5780001 to N.C.). J.T. is a postdoctoral research fellow awarded by the National Center for Genetic Engineering and Biotechnology (BIOTEC).
Disclosure Statement
No competing financial interests exist.