
Abstract
Abstract
Breastfeeding is an experience that only a mother and her infant(s) can share. Infants who can feed from the breast receive not only the best nutrition but also, due to the close physical contact between mother and child, it is the optimal nurturance they can receive from their mother. When breastfeeding is trouble free, maternal well-being is uniquely heightened. However, breastfeeding remains a challenge for many mother-infant dyads and more so for those whose infants are born prematurely. This article introduces a conceptual model of the breastfeeding challenges facing preterm mother-infant dyads. It distinguishes between a maternal caregiving and an infant growth/development components. Within the maternal component, two primary elements are considered, that is, maternal behavioral and nutritional care. The two primary elements within the infant component include infant non-nutritional and nutritional growth/development. It is proposed that an improved understanding of the factors associated with these four elements and how they interplay with each other within individual dyads will facilitate the identification of the breastfeeding challenges facing these mother-infant entities. Due to the intimate relationships existing between a mother and her infant(s), it is further advanced that breastfeeding studies would be optimized if mother-infant pairs are studied as one entity rather than mother and infant separately. It is proposed that this conceptual model will assist health professionals develop personalized breastfeeding management plans for individual preterm mother-infant dyads, while furthering the development of evidence-based interventions to optimize their breastfeeding experiences.
Introduction
T
For the majority of mothers whose infants are born term, this process evolves naturally. However, it is not so when mothers are stressed and/or their infants are sick. For instance, following a premature delivery with infants cared in neonatal intensive care units (NICU), the mother-preterm infant dyad is threatened by the fragility and immaturity of the baby and the unique stress that their mothers experience in the NICU environment.16,17
In an attempt to better understand the breastfeeding challenges facing preterm mother-infant dyads, a conceptual model is introduced that distinguishes between two components, that is, a maternal caregiving and an infant growth/development component (Fig. 1). In turn, the maternal caregiving component comprises two elements, maternal behavioral care and nutritional care/lactation, whereas the infant component distinguishes between their non-nutritional and nutritional growth/development. This model is based on the working premise that, during breastfeeding, these four elements are intimately connected and continually feedback positively or negatively on both partners of the dyad, modulating their interactions. It is advanced that in examining their individual interplays, a clearer understanding would be gained as to how a mother and her infant reciprocal responses impact on one another's actions.
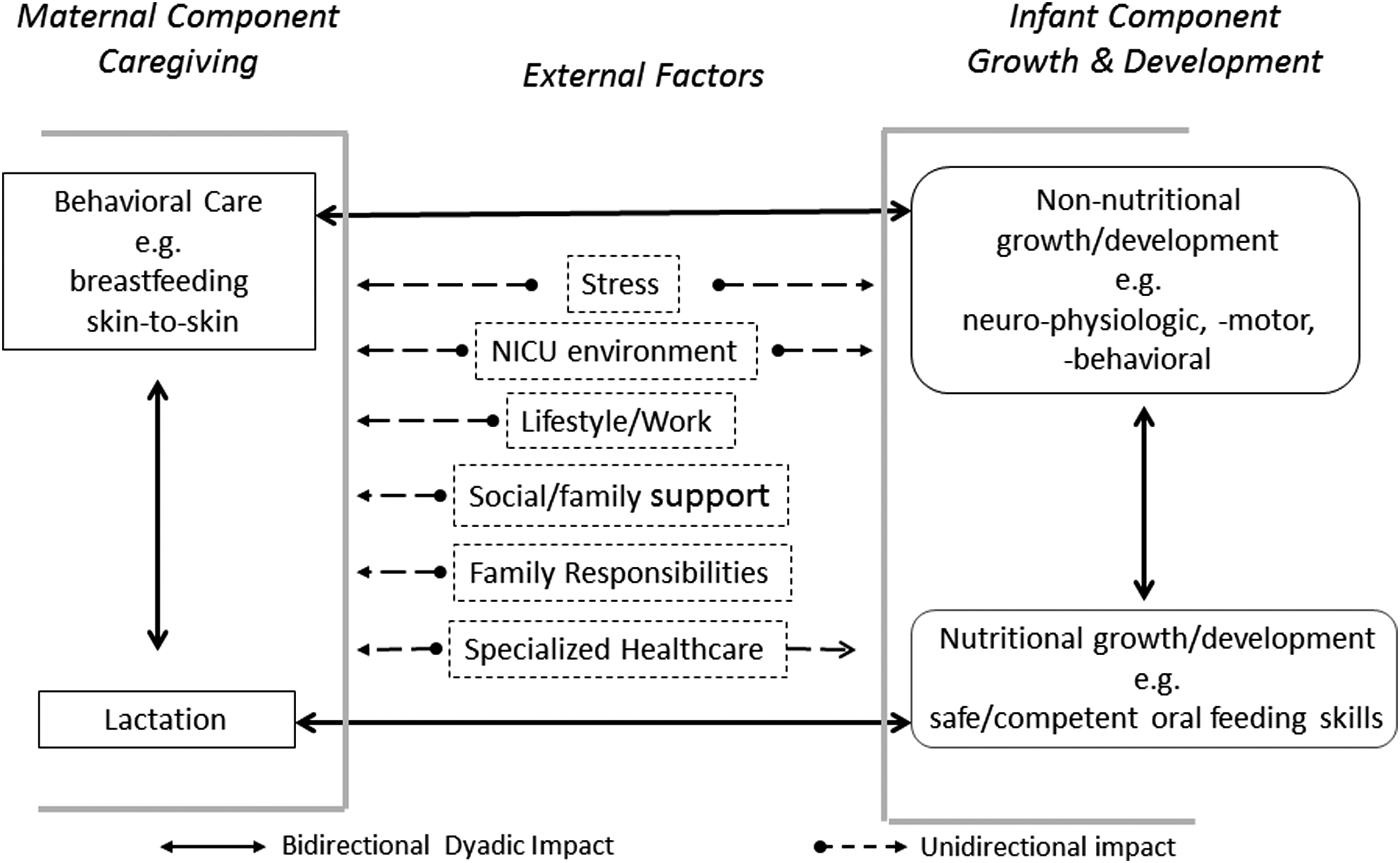
Conceptual model of breastfeeding challenges facing preterm mother-infant dyad—A model presenting four major elements, maternal behavioral and nutritional care and infant non-nutritional and nutritional growth/development, making up the preterm mother-infant dyad with examples of external factors that may impact mother-infant breastfeeding interactions. The bilateral interactions (solid line arrows) between maternal and infant elements represent the reciprocal impact that each partner's actions may have on the other, be they beneficial or detrimental. The external factors (unidirectional dashed arrows) have a unidirectional impact on mother and/or infant as they are not controlled by the dyad, be they beneficial or detrimental
It is well recognized that there exists many more factors that can disrupt the equilibrium described in Figure 1 such as maternal health or attributes, infant's genetic makeup, cultural/societal dogmas, and/or governmental policies. However, it is advanced that the four elements presented in this model are the ones that have the most direct impact on breastfeeding performance. On this basis, one may consider these “disruptive” elements as stressors to the breastfeeding mother-infant dyad.
The Preterm Mother-Infant Dyad
“Breastfeeding” is defined herein as a maternal behavior insofar as it is a mother's prerogative to breastfeed that will allow her infant to feed at the breast rather than from a bottle. In turn, given such opportunity, infants can only breastfeed successfully if their oral feeding skills are sufficiently mature to allow them to remain latched on to the breast for the duration of a breastfeeding session.
The proposed conceptual framework is presented in Figure 1 with maternal behavior and nutritional care under the maternal component and infant non-nutritive and nutritive growth/development under the infant component. In addition, major “external factors,” for example, stress and NICU environment, which may support or hinder a mother and/or her preterm infant relationships are listed.
Maternal behavioral care defines the interactive actions initiated by mothers toward their infant(s), for example, willingness/interest in breastfeeding, milk expression if breastfeeding is not feasible, skin-to-skin holding, and daily routine care for the infant's welfare. Nutritional care (lactation) relates to mothers' ability to provide the appropriate supply of their own milk to meet their infants' nutritional needs. In turn, infants' non-nutritional growth/development addresses their neurophysiologic, neuromotor, and neurobehavioral development, whereas the nutritional element focuses on infants' ability to breastfeed safely and competently to grow. Within the dyad, the relationship that mothers develop with their infant(s) at the time of birth is essential in optimizing the proper establishment of maternal caregiving and infant growth/development.
Mother-infant interactions implicate a continual bidirectional feedback system as their respective actions reciprocally impact on one another, be they beneficial or not. This relationship would be optimized if it is mutualistic, that is, a reciprocal “give and take” interaction as both partners benefit from one another's sensory and behavioral exchanges, thereby optimizing the development of the mother-infant dyad.18,19 The external factors predominantly have a unidirectional impact on these four dyadic elements and are relatively “uncontrollable,” that is, their actions being imposed by environmental and social conditions and/or well-intentioned care providers. It is the complexity of all these interactions that often challenges the ability of mothers and infants to succeed in breastfeeding.
The interactive “give and take” that develops between the partners of the dyad may be “balanced” as often observed between a mother and her healthy infant or “imbalanced” when one and/or both partners encounter difficulties of their own.20,21 Following a premature delivery, the “imbalanced exchanges” primarily arise from infants' immaturity, fragility, and unstable medical status that require the care of neonatal specialists. Along with prolonged hospitalization in the stark environment of an NICU, the normal maternal caregiving is disrupted with breastfeeding initiation and maintenance frequently deferred. It is well acknowledged that these unexpected detrimental events become significant stressors for these mothers.22–28
Mother caregiving
Maternal behavioral care
Within the animal kingdom, humans are considered “semialtricial” as newborns are relatively helpless and must rely on mother for nurturance, nutrition, and locomotion.19,29 Mother can be viewed as the active partner of the dyad, the initiator who nurtures and feeds her child. Although infants may appear to be passive recipients, their responses to maternal investment are essential for maintaining the quality of maternal care as both partners' reciprocal feedback is required to ensure the dyad's integrity.19,30–32 Studies have speculated on the genetics of maternal behavior (motherhood) and their potential in affecting maternal caregiving through neurohormonal involvement and activation of specific areas of the central nervous system (CNS), for example, hypothalamus, amygdala, and medial preoptic area.29,31,33–35
Maternal behavioral care includes functions such as nurturing, maintaining close physical contact with the infant through skin-to-skin holding, attachment/bonding, appropriate responsiveness to infant's cues to meet their needs, and provision of needed care that the infant cannot perform.21,36–42 Over time, “balanced” mutualistic exchanges would be achieved if maternal and infant behaviors are synchronized with both partners continually adjusting to their reciprocal growing needs and development.40,43,44 Breastfeeding and skin-to-skin holding strengthen such mother-infant communications.37,45–47
However, a mother-infant dyad can also be tainted by maternal characteristics, stress, and environmental factors, for example, responsibilities toward other children, occupation, and marital relationship.13–15,40 If maternal behavioral care implicates hormonal stimulation, for example, prolactin and oxytocin, in return, its maintenance necessitates the continued presence and feedback of the young by mother's side.33,48–50 Attachment between mother and infant will be “secure” if mother is responsive, protective, and sensitive to her infant's emotional and physical needs, and “insecure” or “anxious” if mother is unpredictable, distant, and neglectful. Such early patterns of “attachment security” can have a long-lasting positive or negative impact on both mother and child.42,49,51–59
Nutritional care
To safeguard lactation, it is necessary to have a good understanding of both the physiology of lactation and maternal interest in lactating.2,60 Under normal circumstances, lactation performance is a function of “supply and demand,” namely, the greater an infant's nutritional need, the greater a mother's milk production/ejection.
Neville early on differentiated between two stages of lactation, namely Lactogenesis I consisting of the mammary glandular and ductal development, that is, their cellular and enzymatic differentiation, followed by Lactogenesis II pertaining to milk synthesis and ejection. 61 It is important to recognize that milk synthesis is dependent upon the adequate presence of lactogenic hormones, for example, prolactin, leptin, opiates, and insulin, while milk ejection from the breast is primarily dependent upon the release of oxytocin from the posterior pituitary. As such, milk synthesis and ejection are regulated by two separate neuroendocrine functions that singly or together can affect the overall lactation performance of a mother (Stress and lactation section below).
Following the normal gestational period and birth of a term infant, it is generally expected that proper lactation will occur as a result of the normal anatomical and physiologic development of the mammary function. However, it remains uncertain whether following a shortened gestation due to a premature delivery, Lactogenesis I and II have sufficiently advanced to allow for proper milk synthesis and ejection. Understandably, the functionality of Lactogenesis I has been difficult to study at the cellular/molecular level. In regard to Lactogenesis II, results have been inconclusive. As the release of appropriate lactogenic hormones necessary for milk synthesis and ejection is a two-step neuroendocrine reflex, it is dependent upon the proper development of neural networks originating from the mammary sensory receptors to the CNS. Again, following a premature delivery and depending on the shortened gestation period involved, it is uncertain the extent to which such development has occurred.2,62,63
Indeed, if this reflex has not “fully” developed, one may speculate that maternal neurosensory and/or neuroendocrine responsiveness to breastfeeding would be hindered resulting in a decrease in milk synthesis and/or ejection. Peripheral factors such as mother's nipple shape and degree of elasticity and protractility may impede breastfeeding as they can play a determining role in the infant's ability to latch onto the nipple-areola complex. 2 As lactation is a function of supply and demand, any decrease in infant's demand, whether due to infant's inability to latch on, immature nutritive sucking skills, poor endurance, and/or disinterest in breastfeeding would lead to decreased milk availability.
Infant growth/development
Non-nutritional growth/development
The non-nutritional benefits offered by breastfeeding to the preterm dyad relate to the impact that the frequent and close physical contact between mother and infant has in stimulating infant growth/development. This is substantiated by a number of studies in animals and humans showing the benefits of tactile stimulation.46,64–69 Infant growth/development can be measured by outcomes such as weight gain and maturation of physiological and neural functions. However, motor movement is one of the most examined areas of development because it is a resultant of the maturation of combined anatomical, peripheral, and central neurophysiologic and neuromotor functions. In addition, its ease of observation facilitates the identification of objective measures to follow its evolution.
Thelen 70 has proposed that motor behavior or movements are observable “outputs” that emerge in a “self-organizing manner,” be it appropriate or not, from interactions between diverse subsystems, for example, physiological, biomechanical, and psychological. 71 Under such definition, infants' ability to safely and competently breastfeed may be considered one of the earliest markers of non-nutritional growth/development.
It is also believed that brain plasticity reorganizes sensorimotor areas in response to repetitive beneficial or detrimental practices.72,73 If such “practice makes perfect” approach is constructive, preterm infants' physical isolation that limits sensory stimulations during their NICU stay would put them at a disadvantage. From the infants' standpoint, their direct physical/sensory contact with mother would be crucial for their growth/development. 74 Therefore, the multisensory exchanges between mother and infant play an essential part in the safeguard of a close-knit relationship, proper development of maternal behavioral care, and infant growth/development.
Nutritional growth/development
Preterm infants' inability to transition readily from tube to independent breastfeeding or bottle feeding is an example of the motor developmental model discussed above. Unlike term infants, preterm infants have less endurance and may not have yet acquired the mature nutritive sucking skills that allow them to feed by mouth efficiently and safely.75,76 This is due to their immature nutritive sucking skills and their inability to coordinate suck-swallow-respiration-esophageal function.76–79 Indeed, with nutritive sucking occurring at 1 suck/sec, 80 accumulation of milk in the oral cavity due to any delay in bolus formation and/or transport down to the stomach through the pharynx and esophagus would increase risks of adverse events, for example, choking, regurgitation, oxygen desaturation, and penetration/aspiration into the lungs.
Caregivers do not have a means to assess the maturity level of their infants' nutritive skills and often have taken to accelerating the advancement of daily oral feedings without necessarily evaluating its appropriateness for their individual patients. This, not only puts infants at risk of adverse events but also raises the risk of long-term oral feeding aversion.2,81 Therefore, one may speculate that oral feeding experience will be successful and safe, if sucking, swallowing, respiration, esophageal activity, their coordinated activities, infant behavioral states, and feeding positions are appropriate.82–84
Preterm mother-infant dyad interplay
Figure 2 shows how the four elements presented in this conceptual model are so intricately linked that alterations in any one of them can readily lead to an unsafe disequilibrium between mother and infant. Such imbalance, if remained undetected, can lead to a multilevel downward spiral, not only threatening breastfeeding success but also the integrity of the whole dyad. This scenario does not pertain only to mother-preterm infants, but any high-risk infant with chronic conditions, for example, bronchopulmonary dysplasia and cardiac or congenital anomalies.

Mother-infant dyad interplays and the negative impact of prematurity and stress—schematic presenting the four interactive pathways (I, II, III, and IV) between mother and infant, be they beneficial or detrimental, and how stress may singly or together impact negatively the four elements of the mother-infant dyad.
The proposed four elements highlight four interactive pathways between and within mother and infant components that can challenge the breastfeeding performance of the dyad. It was mentioned earlier that the quality of these interplays are dependent upon the reciprocal feedbacks between mother and child as they can be positive/beneficial or negative/detrimental depending upon the partners' respective circumstances.
Pathway I relates to the interaction between maternal behavior and lactation. Indeed, the greater a mother's drive to breastfeed, the more likely her milk availability will increase, 85 increasing the probability of her infant being exclusively breastfed or receiving only mother's milk. In reverse, poor lactation may negatively feedback to mother, potentially leading to a decreased drive in breastfeeding and/or interest in expressing milk, 30 simultaneously increasing maternal stress. Pathway II shows the interactions between maternal behavior and infant non-nutritional growth/development that importantly relate to nurturing and bonding. If maternal behavior is inadequate, nurturing and caring/holding one's infant close would decrease affecting infant's growth/development. In return, if infant non-nutritional growth/development was delayed due to a shortened fetal development or infant postnatal fragility, mother-infant contact would be reduced along with increased maternal stress, overall leading to a decrease in maternal-infant interaction. Pathway III presents the interactions between an infant's non-nutritive and nutritive growth/development. With a delayed non-nutritive growth/development, an infant's neurophysiologic and neuromotor maturation would likely impact on his/her oral feeding skills and ability to breastfeed safely and competently. In return, such difficulty would reduce the nutritional and nurturing benefits that breastfeeding offers, further hindering the infant's overall growth/development. Pathway IV relates to the feedback between infant breastfeeding aptitude and lactation.
Safe and competent neonatal oral feeding is a complex dynamic system that relies on the coordination of multiple physiologic functions, behavioral state dynamics, and social interactions. 86 If an infant cannot latch on and remain latched onto the breast due to immature nutritive sucking skills and/or poor endurance, lactation over time will decrease and eventually cease. This may result from various causes, for example, the “supply and demand” principle mentioned earlier, as a decreased demand from the part of the infant will reduce milk supply; infant's inability to remain on the breast will likely increase maternal stress, leading to a decrease in milk production and/or maternal drive to breastfeeding; and with poor lactation, baby in turn will lose interest in breastfeeding and turn to bottle feeding.
Stress impact on the preterm mother-infant dyad
Figure 2 also illustrates how stress may differentially impact on the four elements of the mother-infant dyad depending on the nature of the stressor. Stress may be generated separately from within the individual, mother or child, or both partners of the dyad, or arise from external factors.
Stress and maternal behavioral care
The birth of an infant engenders a certain level of maternal stress. It is not only due to concern over the well-being and caring of the newborn but also due to the adjustments mothers need to make in their own life. A broad range of factors can affect the ease with which women settle into their new role as mothers, for example, maternal characteristics, coping skills, depression, anxiety, personal health, socioeconomic status, family/social support, life style, and/or work.13,14,17,60,87–90 All these factors potentially may hamper women's transition to motherhood. As such, it is understandable that maternal stress may worsen with the birth of a premature high-risk infant. It is now well recognized that mothers' inability to act as a parent in the stark and high-pressured environment of an NICU is a definite stressor.16,17,91
Animal studies have reported that a 4-hour separation between a dam and her pups increases the anxiety-generated c-fos activity in specific brain regions of postpartum rats. 92 In an earlier study, we observed that dams' corticosterone stress response to various stressors is dampened when compared to virgin rats, but is significantly heightened when the stressor threatens their young. 93 A number of studies conducted on breastfeeding women and animals are supportive of such an altered effect of stress during lactation, suggesting that involvement of oxytocin, prolactin, brain CRF-binding protein, and opiates, and activation of the hypothalamo-pituitary-adrenocortical axis are likely implicated.93–98
Over the last two decades, the recognition of oxytocin as a “social” hormone and its importance in the protection of the mother-infant dyad does not relate only to its lactogenic properties, but just as importantly to its social/behavioral impact on motherhood.31,51,54,99–106 The intimate relationship existing between a mother-infant dyad 106 is exemplified by a number of studies demonstrating that maternal well-being or lack thereof is echoed in her child. Maternal increase in circulating cortisol levels during stress has been associated with corresponding changes in their infant. 106 During times of “balanced” interplays, heart rhythms are coordinated between mother and infant. 107
Studies have reported 34% to 40% of mothers of very low birth weight infants were significantly depressed compared to 8–15% of mothers of healthy term infant.17,106,108–110 On the other hand, a meta-analysis study found that “parents of preterm-born children experience only slightly more stress than parents of term-born children, with small effect sizes”. 111 This may be explained by the resilience of mothers whose infants are in an NICU as they find themselves in a situation that they cannot control. 112 However, in an earlier study focused on mothers of infants born between 26 and 29 weeks gestation, we noted that mother's responses to self-reported questionnaires pertaining to depression and parental stress in the NICU were significantly correlated to the individual subjects' social desirability trait. Social desirability bias is one's tendency to overreport or underreport good or bad behaviors to be regarded more favorably by others. 17 Thus, interpretation of self-reported data needs to be more closely scrutinized to ensure the truthfulness of subjects' responses.
Maternal depression has been linked to decreased quality of mother-infant interaction and attachment, more specifically, decreased positive affective involvement and communication as well as breastfeeding performance.17,113,114 More severe and longer lasting psychological conditions such as posttraumatic stress situation have been reported in mothers of preterm infants.115–118 With a high-risk infant, this dyadic interaction may be further affected by maternal feelings of disappointment, guilt, insecurity, and choice not “to engage actively in mothering” for fear that one's infant may die.16,119–121 Therefore, the ability of a mother to compensate for her infant's difficulties through her behavior and traits, for example, resilience, ability to cope, and sensitivity to her infant's cues, is a strong determinant of their dyadic outcome.122–124 In a study conducted on physiotherapists' perceptions about the major obstacles to successful breastfeeding, three categories were identified: maternal obstacles, health professionals, and society. Maternal obstacles comprised lack of motivation, insufficient knowledge, anxiety, and work. Health professionals' obstacles included lack of support, inappropriate lactation management, lack of knowledge/conflicting advice, negative attitudes, and staff shortages. Societal obstacles consisted primarily of lack of social support and lifestyles. However, for these mothers, the most important methods of motivation to maintain breastfeeding pertained to increased information/education and contact with other breastfeeders, 87 an observation also supported by other studies.125–127
Stress and lactation
Based on human and animal studies, the suppressive effect of stress on lactation is generally well recognized. However, the research literature does not support such a consistent outcome. This is likely due to the wide variations in study designs, methodologies, as well as subjects' characteristics/traits, particularly as it relates to clinical studies.93,128,129 Nevertheless, such apparent inconsistencies only emphasize the importance of not “rushing” into generalizing that a particular stressor may be beneficial, detrimental, or have no effect insofar as maternal responses may also be influenced at the same time by the presence of additional environmental and physiologic factors, or their infant feedback to breastfeeding.
From animal research, we have a good physiologic understanding of how and why stress can inhibit lactation at the level of the CNS and peripherally on milk synthesis and ejection. Breastfeeding stimulates the release of the lactogenic hormones in the CNS, for example, prolactin from the anterior pituitary for milk synthesis and oxytocin from the posterior pituitary for milk ejection. There is anatomical evidence of interconnections between the neuroendocrine hypothalamus and the central autonomic system that can directly alter lactogenic hormones at the hypothalamic level or indirectly through catecholaminergic and peptidergic neural networks.130–133 Peripheral inhibition of milk synthesis and ejection may occur as stimulation of the central and/or peripheral autonomic systems can lead to vasoconstriction resulting in decreased hormonal delivery to the mammary alveoli and myoepithelium, respectively.60,134–136 The time delay between lactogenic hormone release and the resulting milk synthesized in the mammary alveoli would appear prolonged hours. 137 This contrasts with the release of milk stored in the mammary alveoli that occurs immediately in response to oxytocin. As such, depending upon the duration of a stressor, acute or prolonged, suppression of lactation may result from a decrease in milk synthesis and/or ejection. Consequently, when mother's milk availability decreases under stress, it becomes difficult to determine whether it is a result of a decrease in milk synthesis and/or milk release.
Stress and infant growth/development
Being born prematurely is a major stressor that infants encounter. Nevertheless, with immature neurophysiologic functions and underdeveloped organs, they must adapt to their ex-utero environment to survive. Consequently, during their time in the NICU, infants are faced with a variety of stressors that they have no control over. As safe oral feeding is one of the last milestones they need to attain before hospital discharge, some of these infants may not have reached the developmental stage that allows them to readily feed by mouth. Under such circumstances, breastfeeding and bottle feeding can become an additional daily struggle that we know can lead to unsafe and inefficient feeding along with long-term feeding aversion. 2 Although safe and competent oral feeding require mature skills, it is important to remember that oral feeding difficulties can also be of nonoral origins, for example, infant's clinical status at feeding time and during the feeding (e.g., cardiorespiratory status and fatigue), the NICU environment (e.g., light and noise level), infant's own behavioral states (e.g., sleepy, quiet alert, or crying), and/or organization (e.g., calm or agitated).138–140
The NICU Setting
The caring of preterm infants, due to their fragility, rests initially and understandably in the hands of the neonatal medical team in NICUs. Such setting drastically restricts opportunities for mother-infant direct contact. In addition, after overcoming the immediate life-threatening and damaging consequences of chronic conditions such as intraventricular hemorrhage and necrotizing enterocolitis, these infants' hospital discharge is often delayed by their inability to feed by mouth as attainment of independent oral feeding is one of the criteria recommended by the AAP for hospital discharge. 141 Consequently, the longer the transition from tube to independent oral feeding, the longer the hospitalization will be.142,143
Within a NICU, introduction and progression of oral feeding, be it breast or bottle, involve the input of the multidisciplinary medical team caring for the infant that includes, not only neonatologists, neonatal nurse practitioners, and neonatal nurses but often feeding specialists, for example, occupational therapists, speech pathologists, neonatal nutritionists, and lactation consultants when breastfeeding is concerned. Under such circumstances, mother and baby receive recommendations from all members of the team. If these messages are not consistent, confusion will likely arise with mothers uncertain about which feeding recommendation is best and infant needing to “adapt” to everyone's differing feeding approaches. This is a good example of an “uncontrollable” external factor mentioned earlier. Therefore, having one feeding plan agreed upon by all team members would be critical from the time a mother and her infant are introduced to oral feeding. Indeed, proper communication, relationship, and performance are important factors that will allow all players to work together effectively and successfully, just as it should be within a mother-infant dyad. At this time, this is unfortunately not common practice, but awareness that multidisciplinary interventions can be beneficial in the care of pediatric feeding disorders is growing. 144
Conclusion
Due to the intimate interactive exchanges existing between a mother and her infant(s) and the knowledge that stress may impact mother and infant differentially and at the same time, it is clear that studying mother and infant independently from one another, as customarily done, is not productive. Studies relating to maternal stress following a premature delivery primarily focus on mothers or infants separately without considering how importantly one partner can affect the other. Thus, to begin deciphering the mother-preterm infant “breastfeeding puzzle”, it would be more relevant to consider the mother-infant pair as one entity rather than two separate entities, that is, mother and infant.
The four elements defined in this model could be readily monitored. For instance, maternal behavioral care may be evaluated by the frequency of maternal NICU visits and skin-to-skin holding; lactation by the frequency of breastfeeding events and milk volume collected during milk expression; infants' non-nutritional growth/development by their overall medical status; and infants'nutritional growth/development by their daily weight gain and oral feeding performance.
As such, there is a unique opportunity to determine within a dyad at risk, the elements within each partner that may benefit from support. In addition, in evaluating the reciprocal effects of mother-infant interplays, this approach would ensure that any clinical management plan developed to assist one partner will, at the least, not be detrimental to the other. As such, our working model may be envisaged as a potential “diagnostic” tool. In summary, this working concept would not only facilitate the selection of relevant interventions that could be offered but also importantly determine whether any ensuing benefits to one partner have relevance for the other.
Footnotes
Acknowledgments
The author wishes to thank her many collaborators who have supported her work over the years and for support from the National Institutes of Health (R01-HD-28140; HD 044469; MO1RR000188). The contents of this publication are solely the responsibility of the author and do not necessarily represent the official views of the National Institute of Child Health and Human Development or the National Institutes of Health.
Disclosure Statement
The author had the sole responsibility for all parts of the article and has no conflict of interests to disclose.