
Abstract
Abstract
Background:
Studies in various fields have demonstrated that experts use specific gaze strategies to achieve better performance. Therefore, we hypothesized that mothers familiar with breastfeeding would use a specific gaze strategy to achieve better latching-on.
Methods:
A head-mounted eye tracker was used to record pupil positions from 14 breastfeeding mothers with 1-month-old infants. Eye gazes were analyzed during the latching-on and assessment phases.
Results:
During the latching-on phase, participants tended to fixate on their breast, the infant's lower face, an intermediate region between the infant's face and the breast, and the region of contact between the infant's mouth and the breast. Once the infant latched onto the breast, mothers typically assessed the latch by fixating on their breast or the region of contact between the infant's mouth and the breast. The gaze patterns were generally maintained without being influenced by the subtask properties of each phase.
Conclusion:
Similar to previous studies, we found that mothers fixated on specific locations that were relevant to the current breastfeeding subtask, suggesting that the gaze behavior contributes to the execution of latching-on. Therefore, it is important to consider that successful latching-on is influenced by maternal physical movements and efficient gazing behaviors.
Introduction
E
It is important for infants to successfully latch-on to the breast of their mothers because it prevents breastfeeding problems, early breastfeeding cessation, and loss of maternal confidence. 13 However, latching-on is a complex task that requires accurate physical movements and careful observation. Although previous studies have only typically evaluated breastfeeding from the perspective of external factors such as physical positioning, latching-on and breastfeeding can be influenced by other factors, including the mother's observation or concentration. Therefore, we hypothesized that mothers would exhibit a specific gaze strategy to successfully execute latching-on, similar to the strategies that are observed among other experts.
We used a portable eye tracker to monitor gazing behaviors for latching-on during natural breastfeeding. This task requires the sequential performance of various subtasks that require different physical movements and observations. Thus, we divided the process into two phases—the latching-on phase (Phase 1) and the assessment phase (Phase 2)—to compare mothers' gaze behaviors during these phases.
To facilitate this comparison, we adopted two assumptions. First, we assumed that the fixation proportions would differ between the two phases, as experts fixate on areas with relevant information for the current action.2–5 This assumption led us to predict that the mothers would fixate more often on the infant's lower face and their breast during Phase 1, and they would fixate more often on the contact region between the infant's mouth and their breast during Phase 2. Second, we assumed that the gaze pattern (the number of fixations per unit time and the mean duration per fixation) would vary during each subtask of the latching-on, as gaze pattern is influenced by task complexity. For example, Pelz et al. reported that each gaze pattern of the three subtasks during the model building task was different. 14 Therefore, we assumed that Phase 1 would involve a relatively large number of shorter fixations, and Phase 2 would require fewer and prolonged fixations.
Methods
Participants
We evaluated breastfeeding mothers and their infants 1 month after the delivery, to allow time for the mother to adjust to breastfeeding. All assessments were performed by female researchers between August 2012 and November 2014 at the Yamagata Prefectural University of Health Sciences (Japan). The preliminary inclusion criteria for the mothers were age (≥20 years), full-term vaginal delivery, started breastfeeding immediately after delivery, and sufficient visual acuity to obtain a driver's license and be trichromats. The preliminary inclusion criteria for the infants were good health, a full-term delivery (gestational age ≥37 weeks), birth weight ≥2,500 g, and no oral abnormalities.
We initially identified 74 mothers and their infants during their hospital stay; 71 mothers were recruited from a Japanese general hospital, and 3 mothers were recruited through an acquaintance. Among the 74 eligible mothers, 24 mothers provided informed consent to participate (participation rate: 32.4%). We subsequently lost five mothers before the 1-month follow-up: two mothers due to health problems and three due to unspecified reasons. We also excluded data from five mothers due to calibration difficulty or data unavailability. Overall, data from 14 mothers and their infants were included in the final analysis. This study's design was approved by the Ethics Committee of the Yamagata Prefectural University of Health Sciences (1207-05).
The mothers' and infants' average age was 33.2 years (standard deviation [SD]: 4.7 years) and 50.6 days (SD: 7.3 days), respectively. At 1 month, the infants' average weight was 4,992.9 g (SD: 641.1 g). Exclusive breastfeeding was performed by 64% of the mothers, and 36% of the mothers performed nearly exclusive breastfeeding. The mothers exhibited equal proportions of primipara and multipara status and had similar levels of breastfeeding skills during the 1-month study period.
Apparatus
The mother's gazing behaviors were monitored during breastfeeding by using a head-mounted eye tracker (EMR9; NAC Image Technology, Tokyo, Japan), which allowed unrestricted head movement. The device weighed 75 g and included eye and field cameras, a wide-angle lens (92°), and a mirror on the glasses (Fig. 1). Participants who wore glasses or hard corrective lenses for near- or far sightedness were not suitable for this measurement. Pretesting evaluations in a different group of individuals revealed that the binocular cameras obstructed the mother's field of view during breastfeeding, which led us to use a monocular eye tracker in this study (without considering eye dominance). The monocular tracker recorded the right pupil's position at a sampling rate of 60 Hz, and the mother's field of view was recorded for every video frame (i.e., every 33.3 ms). The mother's pupil data were superimposed onto the video data from the field camera, which allowed us to track and analyze the eye's foveal location (i.e., gaze patterns and fixation locations). We also monitored the mother's body and head movements by using a video camera (HDR-CX370V; Sony, Tokyo, Japan) that was positioned ∼2 m to the mother's right side.
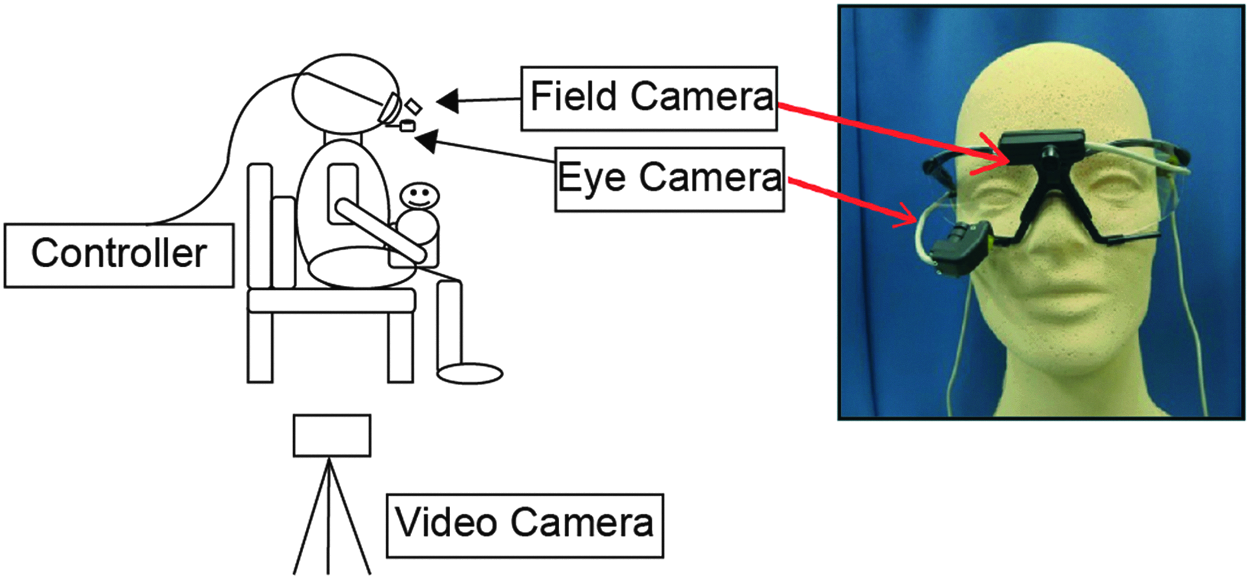
The measurement procedure.
Procedures
Each mother was briefed regarding the testing equipment and procedures and was then fitted with the tracker before the infant exhibited early signs of hunger. A nine-point calibration was performed for each mother. The mothers were then asked to begin breastfeeding on the left breast and to give a verbal signal when they determined that latching-on was successful. No time restrictions were set, which allowed the mothers to breastfeed normally until their infants were satiated.
Although we collected data throughout the breastfeeding session, we only considered data obtained during Phases 1 and 2. The duration of each phase was recorded for each participant. Similar to the previous studies, we defined eye fixation as the eye having a stationary position for ≥100 ms (≥3 video frames). 15 Phase 1 started from the onset of breastfeeding and ended when the researchers identified successful latching-on. Phase 2 continued from the end of Phase 1 until the mother gave the verbal signal that she had identified successful latching-on. Successful latching-on was defined as the mother's breast completely filling the infant's mouth with the mouth wide open, lips flared, and chin in contact with the breast. The researchers evaluated latching-on by repeatedly analyzing the video data from the field camera.
Data analysis
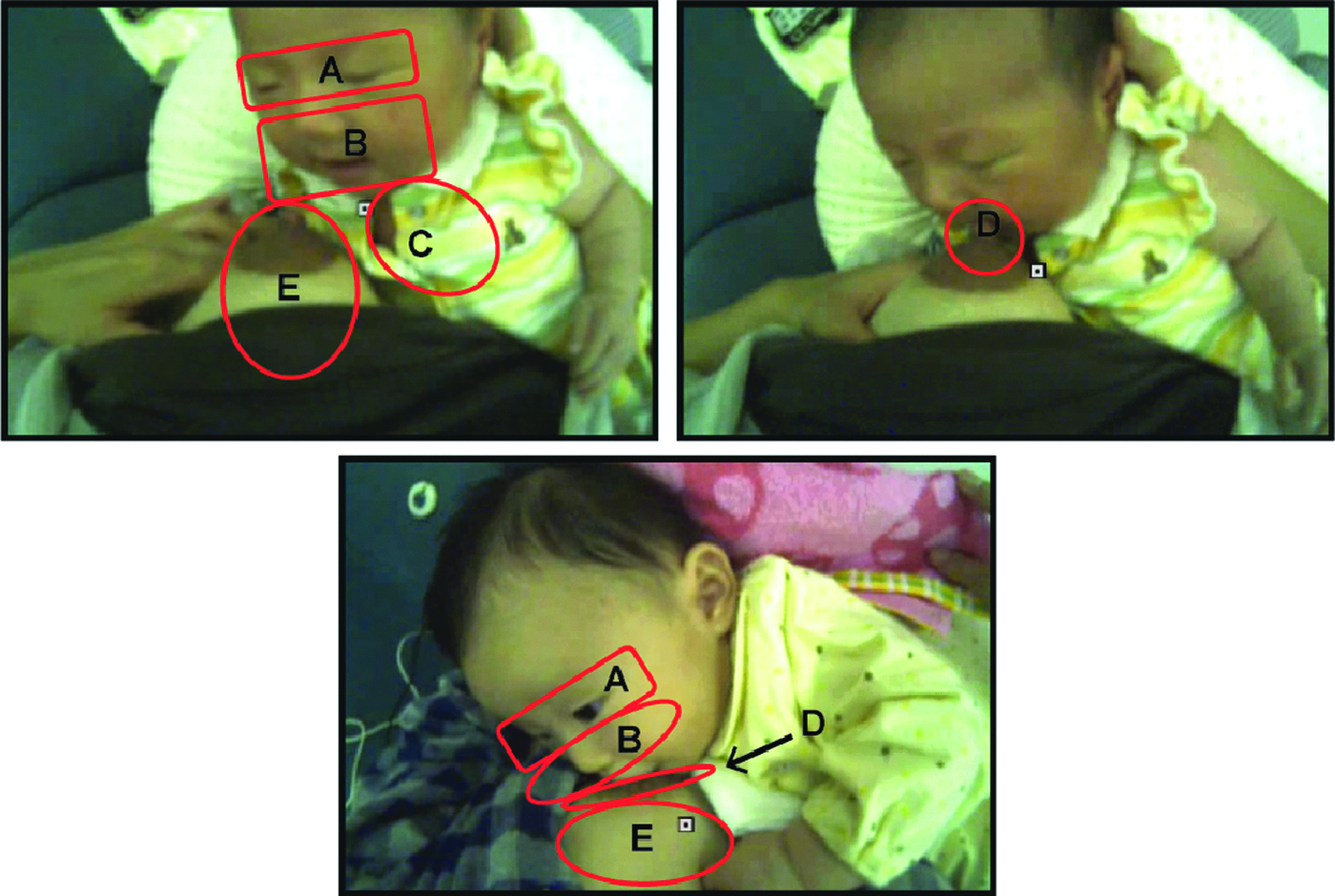
The eye gazing data were analyzed to identify fixations by using software (EMR d-Factory; NAC Image Technology), and they were subsequently coded for the location by using frame-by-frame analysis. Two researchers independently reviewed all the eye gazing data and coded the fixation locations by using an analysis template (Fig. 2). The kappa scores for inter-rater agreement ranged from 0.58 to 0.95, and disagreements were resolved through discussion. The coding template was developed during pretesting and included six fixation locations: the upper face, the lower face, the intermediate region between the infant's face and the breast, the region of contact between the infant's mouth and the breast, the breast, and other locations. The percentages of fixations for each location (number of fixations at one location/the total number of fixations) were calculated for each phase to identify specific visual information that was relevant to latching-on. We also calculated the number of fixations per second and the mean duration per fixation during each phase to examine the mothers' gazing patterns. Wilcoxon matched-pairs signed-ranks test was used to compare the percentages of fixations for each location, the number of fixations per second, and the mean duration per fixation during each phase. Differences were considered statistically significant at a p-value of <0.05. Data were reported as mean (SD).
Results
The mean duration of each phase
The mean duration of Phase 1 was 8.8 seconds (SD: 7.1 seconds), with a range of 1.2–26.5 seconds. The mean duration of Phase 2 was 7.2 seconds (SD: 3.8 seconds), with a range of 1.8–14.8 seconds.
Percentages of fixation for each location
Figure 3 shows the mean percentages of fixation for individual locations during the two phases. During Phases 1 and 2, we observed fixation on the upper face, lower face, the intermediate region between the infant's face and the breast, the region of contact between the infant's mouth and the breast, and the breast. However, during Phase 2, we did not observe fixation on the intermediate region between the infant's face and the breast. The participants exhibited more fixations on the lower face and breast during Phase 1, although no significant differences were seen between Phases 1 and 2. As predicted, a significant difference was found when we compared the percentage of fixation values for the region of contact between the infant's mouth and the breast (Phase 1: 9.0% ± 3.5%; Phase 2: 24.5% ± 5.4%, p = 0.013).
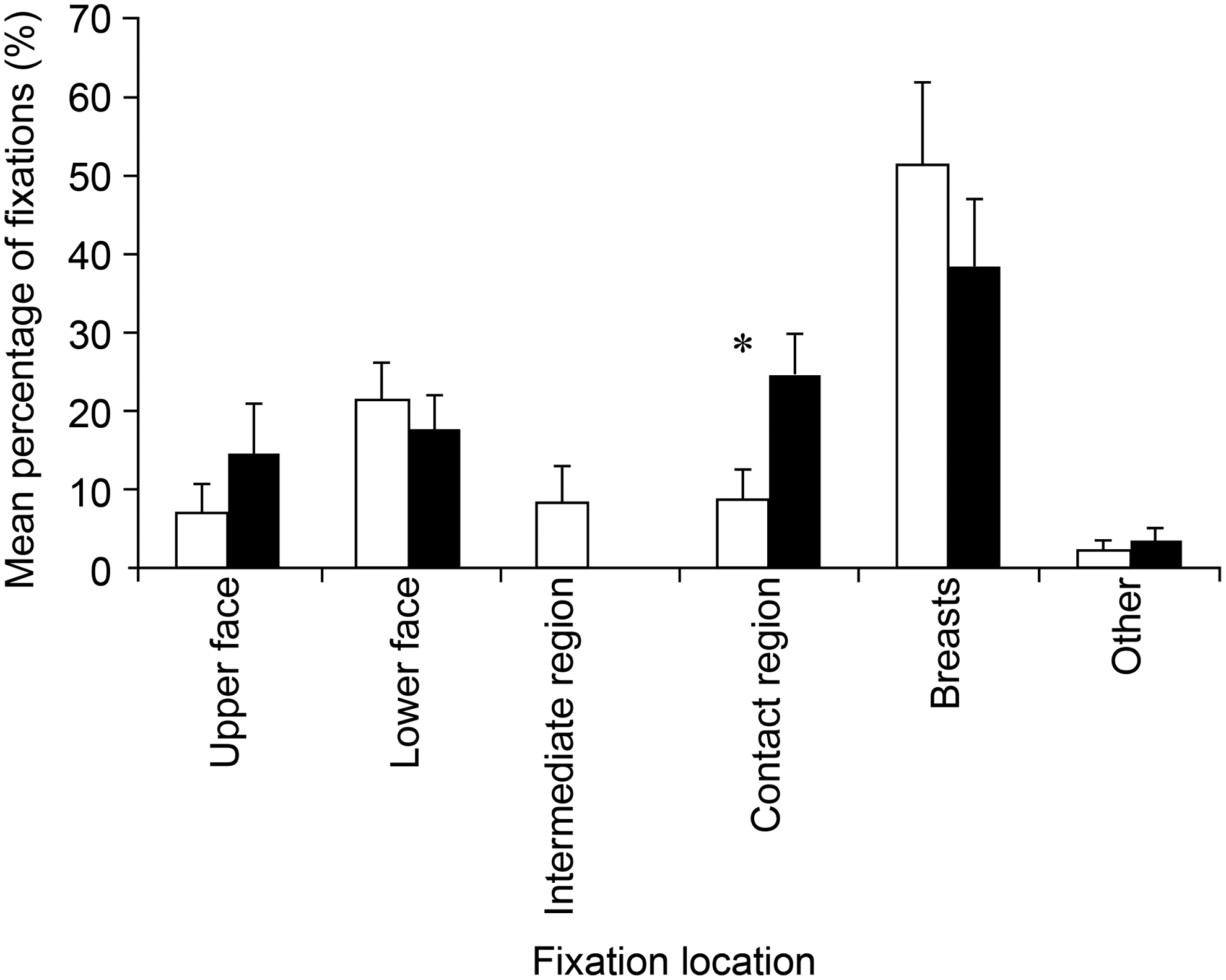
Percentage of fixations (mean ± standard deviation) for individual locations during the latching-on phase (□) and the assessment phase (▪). *A significant difference between the phases.
Gaze patterns
There were a larger number of fixations per second during Phase 1, compared with Phase 2 (3.1 ± 0.4 versus 2.7 ± 0.2). The mean duration per fixation tended to be shorter during Phase 1, compared with Phase 2 (380.9 ± 39.8 ms versus 455.4 ± 77.2 ms). Neither trend was statistically significant (Fig. 4). Contrary to our expectations, we did not observe any changes in the gaze patterns during the latching-on task.
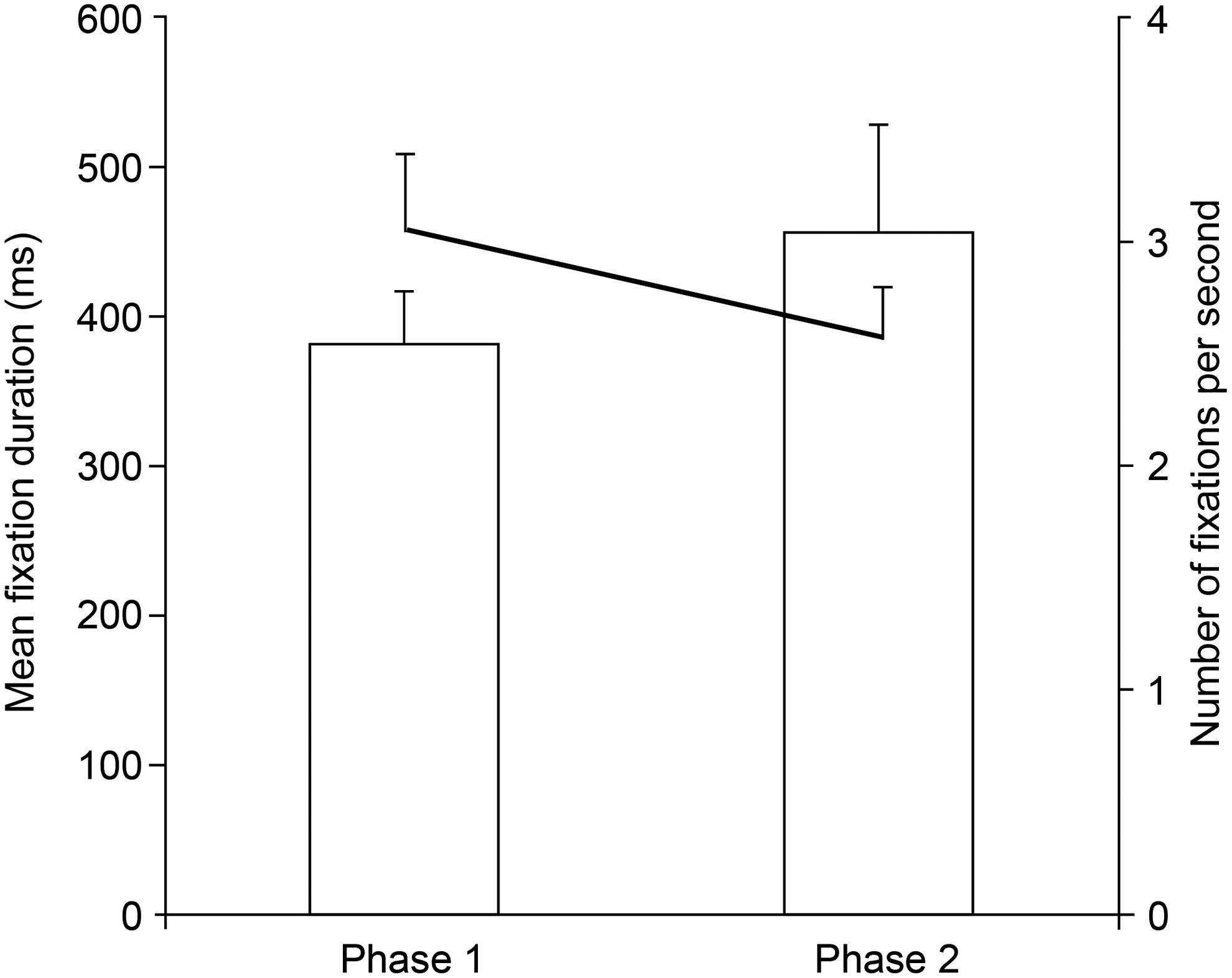
Gaze pattern: the number of fixations per second and the mean fixation duration per fixation (mean ± standard deviation). The bar chart shows the mean fixation duration per fixation. The thick line shows the number of fixations per second.
Discussion
The function of specific visual information for latching-on
We hypothesized that the proportion of fixations for specific locations would differ between the two phases as the overall motor task is completed by using a sequence of subtasks that require different physical movements and gaze patterns. Most fixations appeared to focus on the most relevant location for latching-on in Phase 1. It is also interesting that mothers fixated on the intermediate region between the infant's face and their breast only in this phase. Previous studies have confirmed that fixation near a key spatial location allows athletes to complete specific tasks by extracting a broad range of information through their parafovea or peripheral vision.3,8 Thus, fixation on the intermediate region between the infant's face and the breast would allow mothers to rapidly collect valuable visual information and perform physical actions in response to changing situations during the latching-on.
We observed fixations on the lower face and breast during Phases 1 and 2, although there were no significant differences, which contradicted our expectations. Interestingly, these fixations seemed to have a critical role during the subtasks in Phase 1. Similarly, Land et al. identified four functions of gaze fixation during ordinary tasks: locating, directing, guiding, and checking. 10 In our study, most fixations on the lower face and the breast during Phase 1 seemed to be a part of the guiding function, which implies one or multiple fixations between two distinct but related objects (e.g., a kettle and lid or a hammer and nail). This fixation allows for relatively continuous feedback that helps guide the completion of the intended activity and allows for orientation matching and adjustment for changing distances. During latching-on, the infant's mouth and the breast are distinct but related objects, and fixations on the infant's lower face and the mother's breast could provide visual information to ensure that latching-on is successful. However, during Phase 1, some fixations on the breast may also have a different function, such as the directing function that was proposed by Land et al. 10 In this context, directing fixations target an object or a location for immediate action and provide fovea-centered goal-position information to guide the arm. Thus, some fixations on the breast during Phase 1 might provide information regarding the breast's spatial position and allow the mother to guide her arm movements during latching-on. Moreover, during Phase 1, fixations on the region of contact between the infant's mouth and the breast may help achieve latching-on, as maintaining the fovea on the contact area improves hand–eye coordination and might allow the mother to complete latching-on under visual control.
During Phase 2, most of the fixations appear to represent the intentional gaze behaviors of mothers based on their breastfeeding experience. As seen in Figure 3, fixations on the region of contact between the infant's mouth and the breast were significantly more common during Phase 2, compared with Phase 1. This difference may reflect a visual strategy to collect valuable information for assessing the success of the latching-on. In this context, the contact region is an efficient area for collecting critical visual information during the process of latching-on, as it is a location that includes the mother's areola and the infant's lip, nose, cheek, and lower jaw. Thus, information for this evaluation could easily be acquired by maintaining the fovea on the contact region. Moreover, fixations on the lower face and the breast during Phase 2 seemed to be similar to the function of fixations on the contact region. Therefore, it appears that maintaining the fovea on the lower face and breast may allow mothers to evaluate the success of latching-on and that the participants may have already identified this fact during their previous month of breastfeeding.
The upper region of the face includes the eyes, and fixation on this region would be expected to provide visual information regarding the infant's facial expressions. However, we found that the participants did not frequently fixate on the upper face during both phases. Thus, facial expressions may not be important during the performance or assessment of the latching-on task. Alternatively, it is possible that mothers could read their infant's facial expressions by using their parafovea or peripheral vision, rather than their central vision.
Gaze patterns for processing the visual information during latching-on
Our hypothesis for the present study was that the participants would exhibit different gaze patterns during the two phases, with more frequent and shorter fixations during Phase 1, and fewer but longer fixations during Phase 2. However, we did not detect significant differences in the gaze patterns during the two phases, which would indicate that the mother's gaze pattern is generally maintained without being influenced by the subtask properties during the two phases of latching-on. These results may be related to our participants' proficiency with breastfeeding as auditory or somatic senses (e.g., skin sensibility) might augment visual data for assessing latching-on success after 1 month of breastfeeding. If this speculation is correct, it would explain why we did not observe prolonged fixations during Phase 2 and might suggest that different results could have been observed if we included mothers with less breastfeeding experience.
In the present study, the mean fixation durations were 380.9 ms during Phase 1 and 455.4 ms during Phase 2. However, fixation duration is related to fixation frequency and depends critically on the time required to acquire the information that is needed for the current action.16,17 In addition, fixation duration could be prolonged in situations with a greater need for confirmation. Pelz and Canosa found that the mean fixation duration during a hand-washing task was 327 ms. 18 In another study, most subjects spent 100–200 ms while making a sandwich, although there were some variations between the subjects. 10 These results were obtained during tasks performed in a real-world environment similar to our study. Thus, as the fixation duration during Phase 1 of our study was similar to the duration for hand-washing tasks, it is possible that mothers who are familiar with breastfeeding could process visual information efficiently during Phase 1, similar to our familiarity with other activities of daily living (e.g., hand washing). However, the fixation durations in Phase 2 were slightly longer than the results for other tasks, which would indicate that greater confirmation is required during Phase 2, compared with other tasks. Thus, maintaining a relatively constant gazing pattern during latching-on is less stressful and more efficient for the mother.
The results of this study provide new information to understand the breastfeeding dynamics. However, we should consider the gaze behavior of mothers who are not successful breastfeeders in future studies. Recent studies in the field of sports have shown a positive result of gaze training in the improvement of motor skill performance.19,20 Clarifying the gaze behavior during breastfeeding may lead to the development of a new educational strategy that would aid more successful breastfeeding.
Conclusions
Our study examined gaze behaviors during latching-on in a natural environment and found that the fixations involved specific locations that were relevant to the ongoing subtask, which is similar to the findings of previous studies. These results indicate that the specific locations involved in successful latching-on are the infant's lower face, the mother's breast, the intermediate region between the infant's face and the mother's breast, and the region of contact between the infant's mouth and the mother's breast. It also appears that to assess the success of the latching-on, mothers fixated on the region of contact between the infant's mouth and their breast or their breast alone. Furthermore, we found that mothers generally maintained their gaze patterns, which were not influenced by the specific properties of each subtask.
Footnotes
Acknowledgments
The authors gratefully acknowledge the mothers and infants who participated in this study. They also acknowledge Dr. Hiromi Fujii for his helpful suggestions. This work was supported by JPSS KAKENHI grant number 23660069.
Disclosure Statement
No competing financial interests exist.