
Abstract
Abstract
Purpose:
Breast milk stem cells are hypothesized to be involved in infant health and development. Our research team is the first known team to enroll mothers of hospitalized preterm infants during the first few weeks of lactation and compare stem cell phenotypes and gene expression to mothers of healthy full-term infants.
Settings:
Participants were recruited from a Level IV Neonatal Intensive Care Unit (preterm dyads) and the community (full-term dyads) in the northeastern United States.
Participants:
Mothers of hospitalized preterm infants (<37 weeks gestational age at birth) and mothers of healthy full-term infants (>39 weeks gestational age at birth).
Results:
Breast milk stem-like cell populations were identified in both preterm and full-term breast milk samples. The data suggest variability in the proportion of stem cell phenotypes present, as well as statistically significant differential expression (both over- and underexpression) of stem cell-specific genetic markers when comparing mothers' milk for preterm and full-term births.
Conclusions:
Our findings indicate that (1) stem cells are present in preterm breast milk; (2) differential expression of stem cell-specific markers can be detected in preterm and full-term breast milk samples; and (3) the percentage of cells expressing the various stem cell-specific markers differs when preterm and full-term breast milk samples are compared.
Introduction
P
Researchers have identified a number of different cell types within breast milk, including a population of cells that may contribute to the positive impact of a human breast milk diet on infant health and development. First identified in 2007, human breast milk stem cells are now known to be present in the breast milk of mothers with full-term infants. 12 Referred to as breast milk stem cells (BSCs), these stem cells have been found to have pluripotent characteristics, which means that they have the potential to differentiate into many cell types much like human embryonic stem cells.13,14 During pregnancy, an embryo contains human embryonic stem cells (hESCs), the most versatile stem cell type due to their ability to differentiate into all of the cells and tissues needed for fetal development. 15 After birth, the body uses adult stem cells for continued growth, and these stem cells repair injured cells and tissues. 15 Unlike hESCs, under normal conditions, adult stem cells are only able to differentiate into the type of cell or tissue of the organ from which the stem cell originated. 15 However, breast milk stem cells have been found to have pluripotent characteristics, which means that like hESCs, they have the potential to differentiate into a wide range of cells and tissues.13,16
On ingestion of breast milk, cells are able to cross into the systemic circulation of the infant, 17 and it is hypothesized that BSCs may follow the same pathway for disbursement throughout an infant's body.13,16 Recent findings suggest that in mouse models, breast milk stem cells are found in various organs of the mouse pup as differentiated and functioning cells. 18 Thus, it can be hypothesized that breast milk stem cells that are able to circulate in an infant's blood stream may be able to assist in tissue growth and repair. 16 The implications for the beneficial effects of BSCs in breast milk for preterm infants are astounding when the growth, repair, and neurodevelopmental possibilities are considered. 19
Given prior findings that the nutritional composition of breast milk has been shown to differ based on infant nutritional need,7–10 we hypothesize that the stem cell composition of breast milk may also be modifiable based on infant need. Despite new and emerging studies describing BSCs, no known study has specifically described differences between these populations of cells in breast milk from mothers of hospitalized preterm infants compared to healthy full-term infants. 6 In this study, we describe the phenotypes and differential expression of stem cell-specific genetic markers in breast milk between mothers of hospitalized preterm and healthy full-term infants. This is the first study to describe these differences.
Due to the potential therapeutic value of these cells within the preterm population, the first step is to identify the presence of BSCs in breast milk for preterm infants. Therefore, the purpose of this study was to take the first steps to determine if BSCs are present in the breast milk for preterm infants and begin comparison to full-term breast milk.
Materials and Methods
Two groups of mothers were enrolled based on the gestational age at birth of their infant (preterm or full term—see Table 1). Mothers of preterm infants were recruited from a Level IV Neonatal Intensive Care Unit in New England (United States) and mothers of healthy full-term infants were recruited from the surrounding community. Mothers in the preterm group had to have an infant with gestational age <37 weeks at birth (inclusion was purposefully left with a large inclusion range, but enrolled infants ended up very similar in gestation—see Table 2). Mothers in the full-term group were eligible if their infants were ≥39 weeks gestational age at birth. The preterm mothers were also recruited for an interview portion of the study (results not included in this article), and therefore, all mothers must have been able to speak English. We enrolled 19 mother–infant dyads into our study, but the results of this article are based on the cohort where we began analyzing both flow cytometry and quantitative real-time polymerase chain reaction (qRT-PCR) data. After further consideration of the sample characteristics, we excluded one additional preterm infant who only had flow data and whose gestational age at birth was much different than the other infants (this did not change any of the result outcomes). The final sample was seven preterm infants and four full-term infants. Flow cytometry was completed on all 11 samples; however, qRT-PCR was only performed on 10 of the samples (missing 1 full term) as the other was excluded due to low RNA yield.
Protection of preterm infants receiving a human milk diet
To protect preterm infants and to preserve an all maternal breast milk diet, mothers were identified by the PI in collaboration with the lactation and/or medical team to evaluate for sufficient milk supply. Specifically, the following requirements must have been met for mothers to be enrolled in this study: infant was ≥5 days old, and the mother was expressing an average daily pumping volume that was at least 15 mL greater than the total daily volume required by the infant. The PI calculated this number (total daily volume required by infant) based on clinical care and the infant's feeding orders per standard care. These safeguards were calculated at recruitment and again on the day of collection. Mothers of full-term infants were all exclusively breastfeeding and their participation was based on maternal judgment of milk supply.
Design
Breast milk was collected on 1 day for each study participant. All preterm data were collected during Neonatal Intensive Care Unit (NICU) hospitalization through medical chart review and maternal interview. Full-term mother–infant dyad information was collected through maternal interview.
Breast milk collection procedures
Breast milk samples were collected after informed consent and approval through institutional review board (IRB#14-063). Approximately 15 mL of breast milk was obtained using a double electric breast pump from preterm and full-term mothers. On the day of breast milk collection, the PI met with the mothers and instructed them on study collection procedures. Mothers pumped per established routine and then the PI removed 15 mL immediately after the pumping session was completed. All breast milk was handled according to hospital policy and once the sample volume was removed, the remainder was given back to the mother. After collection, each sample was brought immediately to the laboratory on ice and protected from light, and processing began on arrival.
Isolation of cells from breast milk
Figure 1 summarizes the process of cell isolation and characterization of breast milk cells from full-term and preterm mothers. The breast milk sample was split into two parts: (one 5 mL sample and one 10 mL sample). Both samples were centrifuged at 300 g in a benchtop centrifuge (Eppendorf Hauppauge, NY) for 10 minutes. The supernatants were removed and the pellets washed once in 10 mL of sterile phosphate-buffered saline (PBS). After second centrifugation and supernatant removal, 350 μL of RLT buffer (Qiagen, Valencia, CA) was added to the 5 mL sample and frozen at −80°C for RNA isolation and qRT-PCR analysis. A cell count using equal parts of trypan blue (Thermo Fisher Scientific, Waltham, MA) and cell suspension was obtained from the 10 mL sample. This was counted with a hemocytometer and reported as a total number based on the known volume. Two tubes containing 100,000 cells each (from the 10 mL sample) were then processed for flow cytometry as described below.
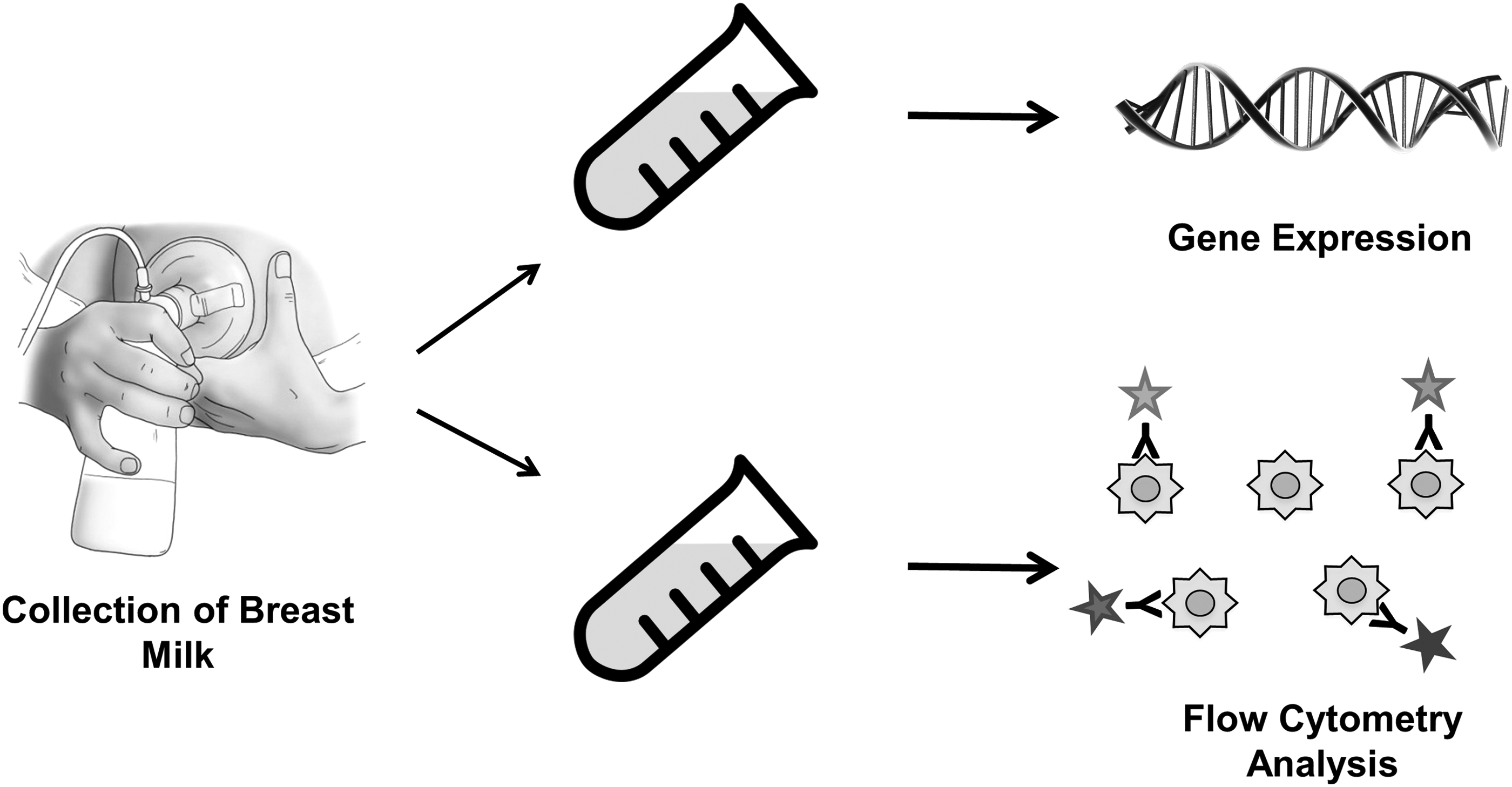
Isolation and characterization of breast milk cells from full-term and preterm mothers.
Quantitative real-time polymerase chain reaction
This test is used to determine gene expression in cells. RNA isolation was performed according to the manufacturer's protocol (Qiagen). RNA was quantified on a NanoDrop spectrophotometer (Thermo Fisher Scientific) and 200 ng of cDNA was generated using the iSCRIPT cDNA synthesis kit (Bio-Rad, Hercules, CA) according to the supplier's protocol. Quantitative real-time polymerase chain reaction (PCR) was performed on a Bio-Rad CFX PCR machine (Bio-Rad) using TaqMan PCR Master Mix (Thermo Fisher Scientific). Primers were purchased from Thermo Fisher Scientific and are summarized in Supplementary Table S1 (Supplementary Data are available online at www.liebertpub.com/bfm). Results were analyzed as described in the Statistics section.
Flow cytometry
This test uses antibodies to identify specific cell populations of interest. Fresh samples were immediately processed for flow cytometry after being counted. Cells were stained with fixable viability dye e780 (Affymetrix, Santa Clara, CA) for 30 minutes according to the protocol. Cells were then centrifuged at 400 g for 4 minutes, supernatant was aspirated, and cells were fixed for 5 minutes with 4% paraformaldehyde. Cells were then centrifuged at 400 g for 4 minutes and resuspended in staining buffer (PBS containing 2% FBS). Surface marker antibodies were allowed to incubate for 30 minutes on ice and are outlined in Supplementary Table S2.
Cells were then centrifuged at 400 g for 4 minutes, supernatant was aspirated, and cells were resuspended in staining buffer containing 0.1% Tween for 20 minutes. After 20 minutes, intracellular marker antibodies were added and allowed to stain for another 20–30 minutes on ice. Those markers included Nestin Alexa 488 and OCT3/4 e660. Cells were then centrifuged at 400 g for 4 minutes, supernatant was aspirated and resuspended in staining buffer, and samples were run on a BD LSRII flow cytometer using BD FACSAria software (BD Bioscience, San Jose, CA). For analysis, only viable cells were included and percent positivity for each marker was calculated.
Statistics
Descriptive statistics were used to characterize the groups. Due to the small sample size, Mann–Whitney U tests were used to analyze differences in group characteristics, and descriptive statistics for these variables are reported as median with interquartile range due to the wide variability of values. For the PCR expression data, we fit a general linear model with a random subject effect to account for replicates of the dependent variable within individual participants and tested whether or not the intercept of that model (e.g., grand mean of logged expression values) was significantly different than zero. In addition, correlations were run for all variables to assess trends in gene phenotype and expression based on potentially contributing factors such as gestational age at birth, number of days postpartum when milk was collected, and infant birth weight. Two-tailed tests were used with significance set at p < 0.05.
Results
Our final sample size included seven mothers of preterm infants and four mothers of full-term infants. The preterm infants averaged 32 weeks gestational age at birth and the full-term infants averaged 40 weeks. All but one mother (in the preterm group) were first-time mothers and lactating for the first time. Gestational age and birth weight were significantly different between the two groups, which is expected (p ≤ 0.05). The mean maternal age (preterm = 29 years; full term = 30 years) did not differ significantly between groups and the number of days postpartum when the milk was collected did not exceed 50 days in either category (preterm mean = 22.3 days; full-term mean = 40.5 days). The difference in days the milk was collected is further addressed in the study limitations. There was variability between all mothers in total cell counts within a 10 mL sample of breast milk, but there was no statistically significant difference between the mean counts in either group (preterm = 1.9 ± 1.2 × 106; full term = 2.5 ± 2 × 106). A full summary of sample characteristics related to infant and maternal demographics is included in Table 2.
Flow cytometry analyses were done on all samples for the following markers: Nestin, SSEA4, TRA-1-60, OCT4, CD90, CD73, CD29, CD117, CD105, CD44, CD34, and CD 45. Data are presented by median percentage and interquartile range in Table 3. Values for preterm and full-term samples were not significantly different between groups.
IQR, interquartile range.
Preterm sample gene expression using qRT-PCR of stem and cell markers was compared/normalized to the full-term sample. Cell markers SOX2, Nanog, CD90, and CD105 were upregulated in the preterm sample. SOX2 had a fold change (FC) of 8.4 (p < 0.0001), Nanog had an FC of 9.2 (p < 0.0001), CD90 had an FC of 8.3 (p = 0.03), and CD105 had an FC of 1.6 (p = 0.001). Other markers (EpCAM and TJP1) were under regulated when normalized to full-term samples—EpCAM had an FC of 0.22 (p < 0.0001) and TJP1 had an FC of 0.56 (p = 0.007) (Fig. 2 and Supplementary Table S3). Details on how these tests were conducted are explained in the Materials and Methods section.
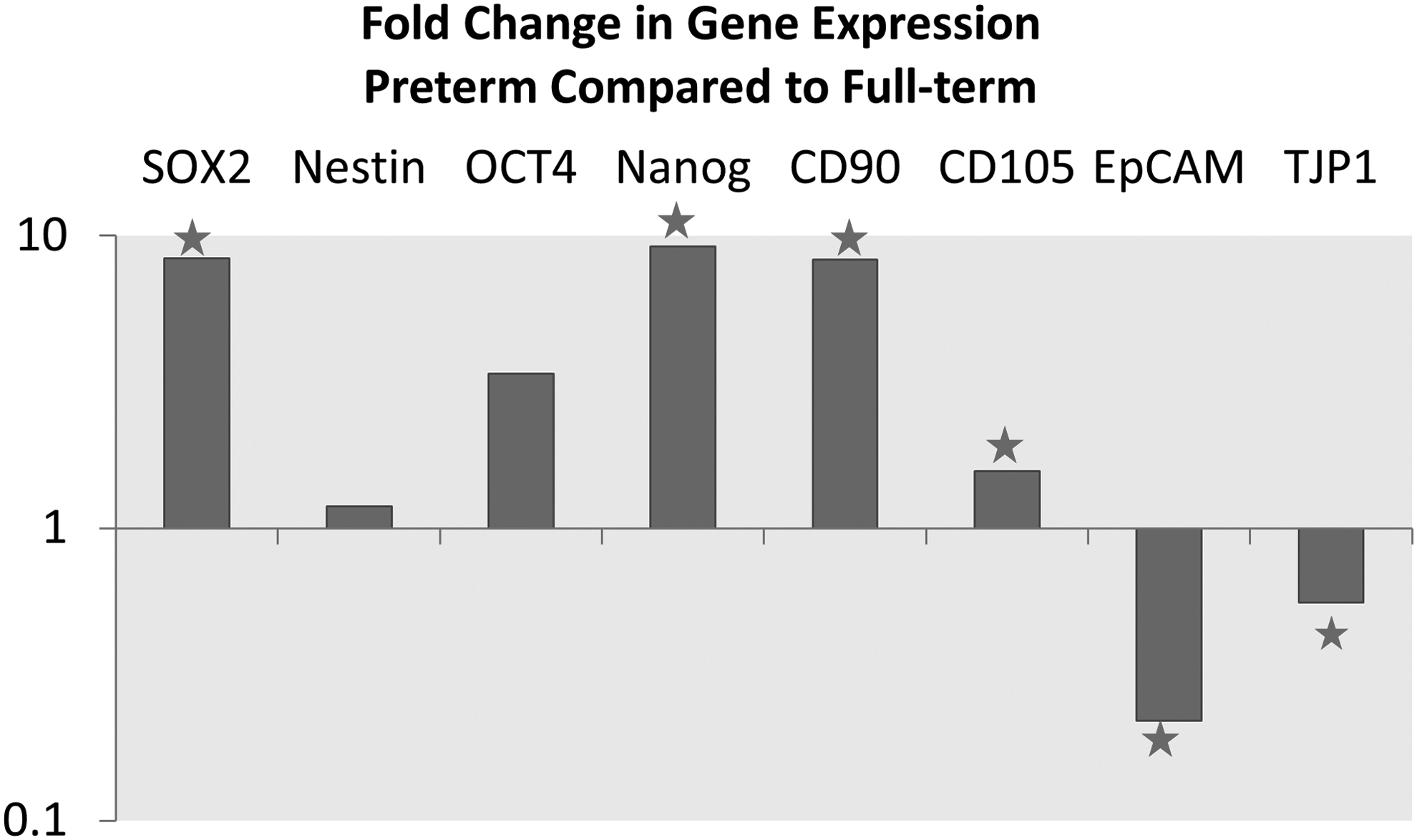
Fold change in gene expression of preterm breast milk compared to full term. Values greater than 1 are upregulated compared to the full-term sample, and those less than 1 are downregulated. ⋆p < 0.05.
Discussion
This study is the first to directly compare the stem cell populations in breast milk from mothers of preterm and full-term infants within the first 2 months postpartum. It is also the first to recruit and report on the specific stem cell content of breast milk from mothers of hospitalized preterm infants. The purpose of this study was to determine if breast milk stem cells are present in the breast milk for preterm infants and compare the samples to full-term breast milk. Our findings indicate that (1) stem cells are present in preterm breast milk; (2) differential expression of stem cell-specific markers can be detected in preterm and full-term breast milk samples; and (3) the percentage of cells expressing the various stem cell-specific markers differs when preterm and full-term breast milk samples are compared. We hypothesize that the findings of no difference in cell phenotypes, but differences in gene expression may indicate that the cells within breast milk of mothers with preterm and full-term infants are of similar structure, but that genetic expression is altered based on factors surrounding preterm birth. These factors may include the preterm infant itself, the stage of breast development/maturation, and/or the disrupted mother–infant coregulation that occurs with mother–infant separation in the NICU.
We are not the first to document the presence of stem cells in breast milk from mothers of preterm infants as another research team recently published that their samples included infants born preterm; however, it was unclear at what point in lactation these women were enrolled. 20 Their participants had breast milk collected on average when the infants were 214 days, compared to our study, where collection occurred on average between 22 (preterm cohort) and 40 days (full-term cohort) postpartum. In addition, our samples were all collected within a smaller amount of time from each other (days 14–50 postpartum), compared to a span of 177 weeks (1,239 days) in the other recently published study. 20 When considering a preterm cohort, the concept of when breast milk is analyzed may be essential as we already know that other aspects of preterm milk (e.g., nutrients) changes over time of lactation, with preterm milk becoming more similar to full-term milk around 10 weeks postpartum. 21 Much of the breast milk stem cell literature report that variability between mothers is common.13,20,22 Recent data support that some of the variability of genes is associated with infant's gestational age, 20 and these researchers propose that all studies of breast milk stem cells be done within a specified time. 20 We further propose due to the known changing dynamics of breast milk throughout lactation, within studies that evaluate breast milk cells, enrollment of mothers should be at similar time points of lactation and/or account for this variable in comparative analyses.
This is the first study to directly compare preterm hospitalized infants to full-term infants and confirm the presence of stem cells in breast milk for preterm infants in the beginning of lactation. These findings promise exciting future research directions that look to more closely analyze key differences in preterm and full-term milk. Furthermore, the differentiation capacity of preterm breast milk stem cells may be similar to the findings of full-term breast milk in their ability to differentiate into all three germ layers. 13 Therefore, the potential of these cells in future individualized stem cell therapy treatment and in regenerative medicine is infinite and additional research is needed to define their potential.
Limitations
This study had a relatively small sample size, however, the purpose of the study was to identify the presence of stem cells in breast milk for preterm infants during hospitalization and this was achieved. The study team aimed to collect milk from preterm and full-term mothers in a similar time period, but the final results yielded a difference in days postpartum the milk was collected. While this difference was adjusted for in our analysis, future studies should aim for a set time of collection for all participants. Additional studies are warranted to further characterize group differences between preterm and full-term milk, and should also focus on stratification by preterm gestational age, and additional maternal variables identified by Twigger and team. 20
Conclusions
Breast milk stem cells are relatively new in the scientific community. Breast milk provides many benefits of which the mechanisms are not fully known. The presence of stem cells in breast milk may help explain these mechanisms as scientific understanding advances. Additional research may be needed to evaluate specific differences in preterm and full-term breast milk. However, given the potential of breast milk stem cells, future analyses may be better suited to instead explore differences in individual expression over time. Since the discovery of breast milk stem cells is in its early stages, hypotheses have been generated about the implications of stem cells in breast milk, but no study to date has closely studied their impact. Future research will be important to obtain additional information on the role of breast milk stem cells in the growth and development of infants, as well as their potential in regenerative medicine.
Footnotes
Acknowledgments
This study was funded by grants from the National Association of Neonatal Nurses and the Foundation for Neonatal Research and Education.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.