
Abstract
Abstract
Background:
The literature on the iron requirements of exclusively breastfed infants contains conflicting data and contrary views.
Objective:
The purpose of this study was to summarize the evidence for both benefits and risks of daily oral iron supplementation with regard to hematologic, growth, cognitive parameters, and adverse effects in exclusively breastfed infants.
Materials and Methods:
Structured electronic searches were conducted using PubMed, Cochrane Library databases, and Google Scholar for randomized controlled trials (RCTs) involving daily iron supplementation in full-term healthy exclusively breastfed infants. Random- and fixed-effects models were used for calculating the pooled estimates.
Results:
Four RCTs with 511 infants were included in the meta-analysis. Iron interventions had no significant effect on iron deficiency or iron deficiency anemia, serum ferritin level, or hemoglobin level. Iron interventions did result in a significant increase in Bayley psychomotor developmental indices in later life (mean difference [MD] = 7.00, confidence interval [95% CI] 0.99–13.01) and mean corpuscular volume (MD = 2.17 fL; 95% CI 0.99–3.35 fL). Iron supplementation was associated with slower growth during the exclusive breastfeeding period, but the long-term effect is unclear.
Conclusions:
Limited available evidence suggests that daily iron supplementation has beneficial effects on hematologic parameters and cognitive development, but may delay physical growth in healthy exclusively breastfed infants. There was no evidence to suggest that iron supplementation could cause other adverse effects.
Introduction
M
Alternatively, concerns have been raised that iron deficiency (ID) is a common cause of anemia in infants which may affect their health and development. Some studies have suggested that early ID can lead to irreversible negative changes in long-term neurodevelopment.5–7 The American Academy of Pediatrics recommends that exclusively breastfed full-term infants receive 1 mg/kg of iron supplementation per day, beginning at 4 months of age. 8 This policy supports the concept that the small amount of iron in human milk may not be enough for the physical and neurological development of exclusively breastfed infants.
Although some studies have evaluated the health benefits and risks of iron-fortified food, it is important to determine whether these health effects and risks are associated with iron intake alone or are due to other nutrients.9,10 Evidence for the benefits and risks of daily oral iron supplementation in exclusively breastfed infants has not been specifically evaluated in a systematic review.
The aim of this systematic review and meta-analysis is to summarize the evidence of the health effects of daily iron supplementation with respect to exclusively breastfed infants before 6 months of age. Data provided could assist policy makers and clinicians to understand the benefits and safety of daily iron supplementation in exclusively breastfed infants.
Materials and Methods
Search strategy
This systematic review was registered with PROSPERO (registration number: CRD42015026031). PubMed, Cochrane Library databases, and Google Scholar were searched up to August 26, 2015. Reference lists from published review and meta-analysis were also reviewed. Search terms included: (iron or iron supplement or iron supplementation) and (infants or toddler or breast feeding or breastfed or breastfeeding). Studies were included if they fulfilled the following criteria: (1) randomized controlled trial (RCT); (2) assessing the effects of iron supplementation on health (iron status, physical growth, neurodevelopment, and morbidity due to infectious disease); and (3) with full-term healthy exclusively breastfed infants. Studies remained eligible when the infants were nearly exclusively breastfed (exclusive breastfeeding but were permitted to give small portions of foods). Studies were excluded if they included the infants that were low birth weight (<2,500 g), or preterm (<37 weeks), or not nearly exclusively breastfed during the intervention, or supplementation with solid foods or formula, or combined iron with other nutrients as the intervention.
Data extraction
The following information was extracted from the articles: the first author, published year, study design, study population characteristics (origin and age), feeding practice, iron form and dose, number of subjects, intervention time, and outcome measurements. One author entered data and a second author checked entries for accuracy. Discrepancies were resolved through discussion.
Assessment of risk of bias in included studies
Two authors (C.C. and M.G.) independently assessed the quality of included RCTs in seven domains (sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective outcome reporting) by the Cochrane risk of bias tool. 11 All the differences were resolved by discussion with the other two authors (J.F. and P.E.).
Statistical analyses
The ID rate, diarrhea rate, weight gains, length gains, hemoglobin level, mean corpuscular volume (MCV), serum ferritin, mental development index, and visual acuity Z-score were compared between breastfed infants who received iron supplementation and breastfed infants who did not receive iron supplementation. The continuous data were extracted as mean ± standard deviation, whereas the dichotomous data were extracted as even/total number. If the study reported two subgroups, the combination formulae were used to combine them into a single group. 12 The continuous data were reported as weighted mean difference, whereas the dichotomous data were presented as risk ratios (RR) with confidence intervals (95% CIs). p < 0.050 was considered statistically significant. I2 was used to evaluate the heterogeneity. A random effects model was used if heterogeneity was detected (I2 > 50%); otherwise, a fixed effects model was used. All analyses were performed using Review Manager, Version 5.3 (Cochrane Collaboration, Oxford, United Kingdom).
Results
The initial search of the database mentioned above identified 8,456 publications, which included 37 relevant articles for full-article review (Fig. 1). An additional seven studies were identified from previous reviews and meta-analyses. After excluding the studies that investigated the iron supplementation with solid food or formula or multivitamin mixtures, or if the infants were not nearly exclusively breastfed during the intervention, there remained RCTs (five articles) that were included in this systematic review and meta-analysis. A total of 511 infants from Sweden, Honduras, Canada, Turkey, and China were included in these four RCTs.
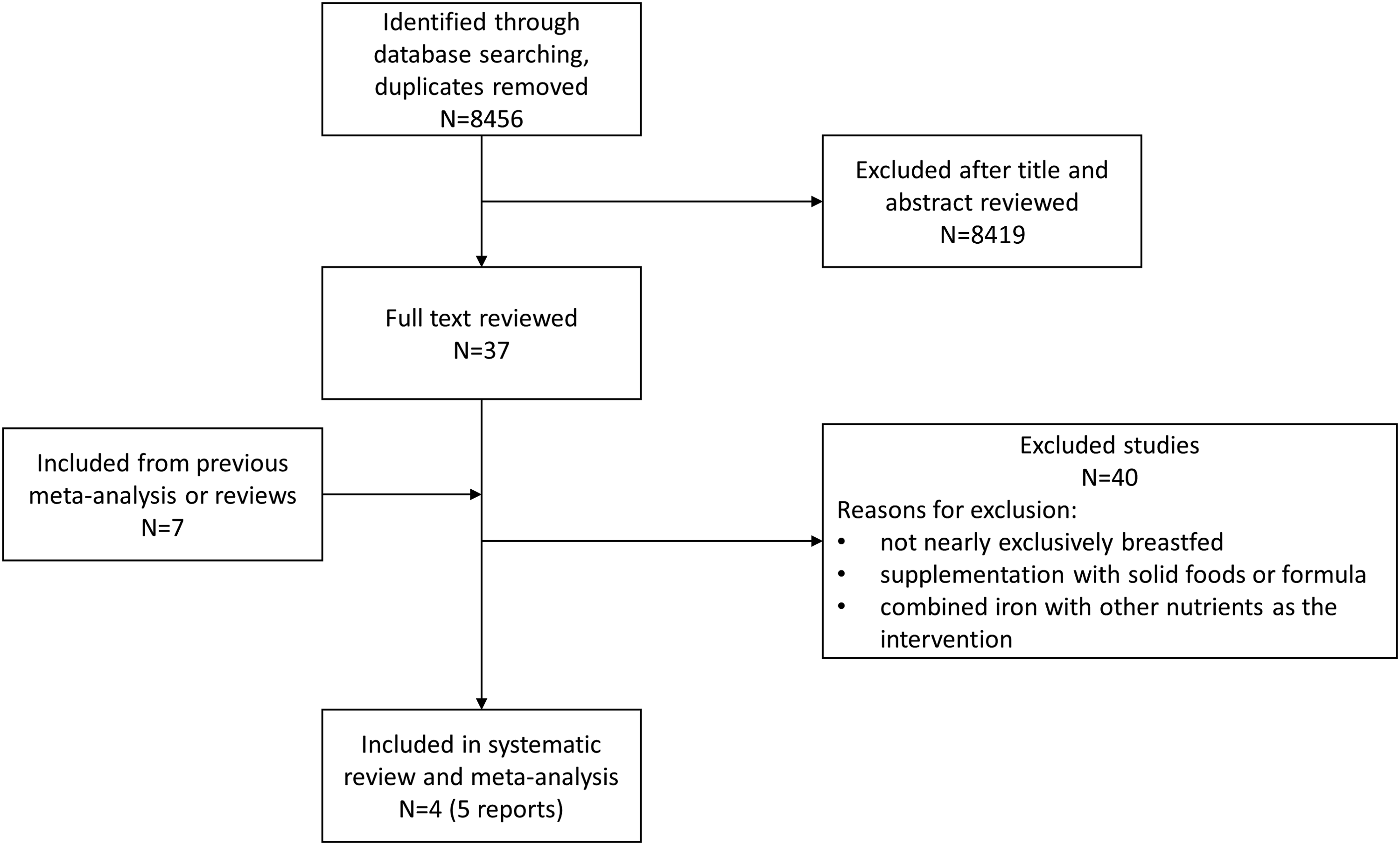
Flowchart of study selection.
Study characteristics
The characteristics of the included trials are summarized in Table 1. The source of iron included ferrous sulfate13–16 and iron amino acid chelate. 17 The iron supplement intervention during the exclusively breastfeeding period lasted between 2 and 2.5 months. One RCT started the intervention at 1 month of age, 14 whereas the other three RCTs started at 4 months of age.13,15–17
RCT, randomized controlled trial.
Assessment of bias risk
The quality of included RCTs was assessed by the Cochrane risk of bias tool. 11 All included trials had certain methodological limitations (Fig. 2). The major limitations were unclear allocation concealment, unclear blinding of outcome assessment, and high risk of bias in selective reporting.
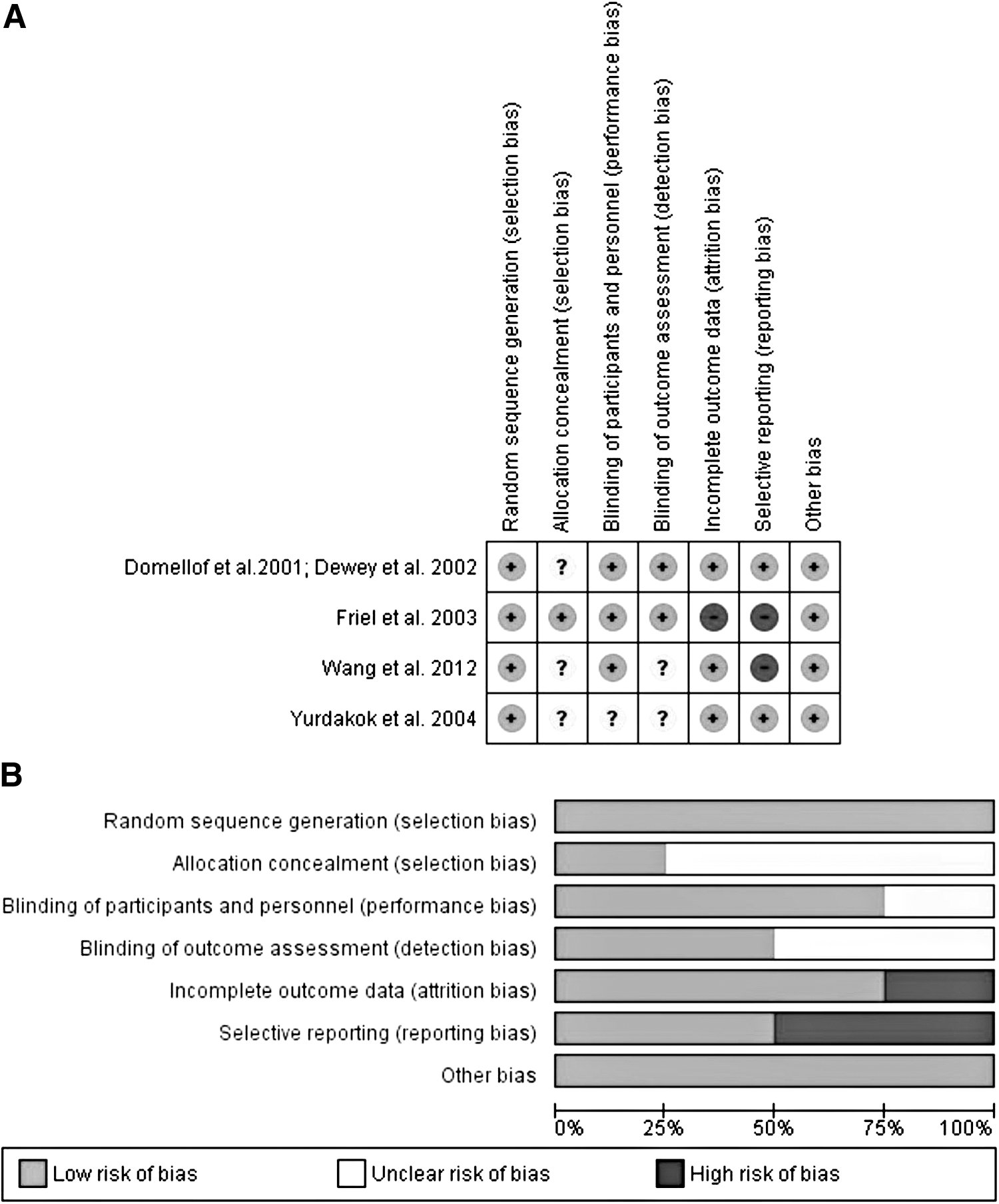
Assessment of bias risk.
ID, IDA, and hematologic parameters
Three RCTs (n = 251) were included in the analysis (Fig. 3). There was no difference in the incidence of IDA or ID between both groups (RR 0.59; 95% CI 0.27–1.30; p = 0.19). Two RCTs reported extractable data on iron status parameters (Fig. 4). Although serum hemoglobin levels (mean difference [MD] = 1.78 g/L; 95% CI −1.00 to 4.57 g/L; p = 0.21) and ferritin levels (MD = −17.26 μg/L; 95% CI −40.96 to 75.47 μg/L; p = 0.56) were similar between both groups, MCV was significantly higher in the group supplemented with iron (MD = 2.17 fL; 95% CI 0.99–3.35 fL; p = 0.0003).
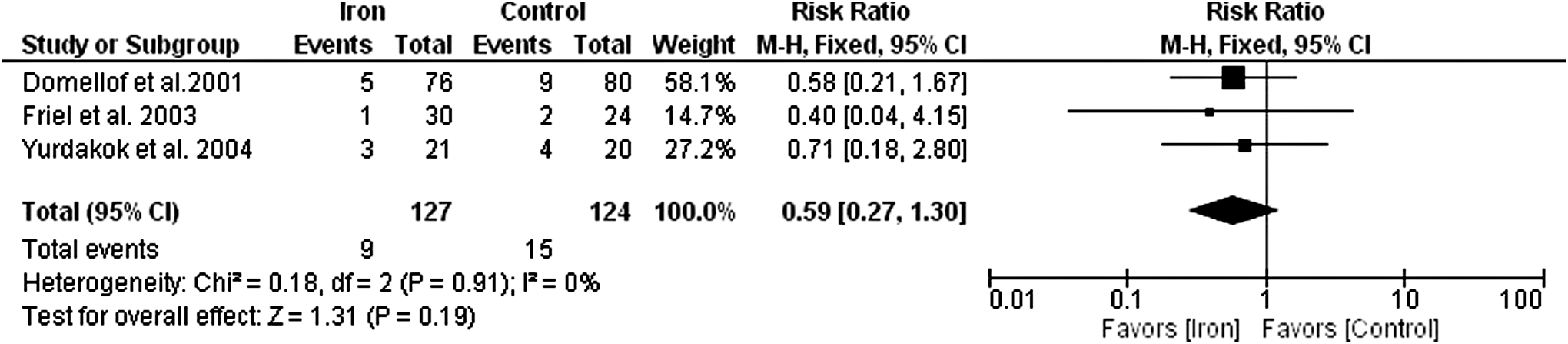
Effect of iron supplementation on IDA or iron deficiency in exclusively breastfed infants. IDA, iron deficiency anemia.
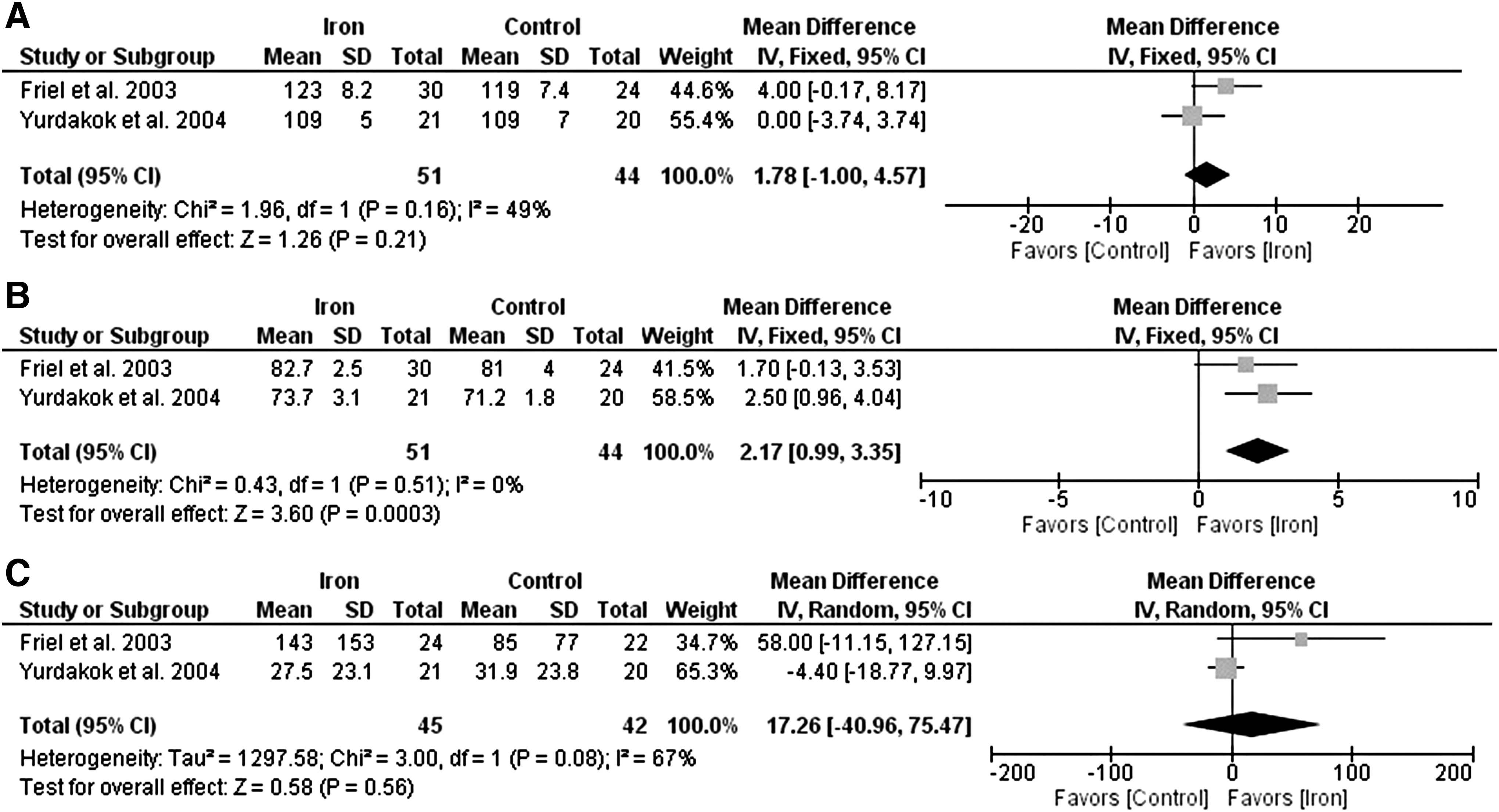
Effects of iron supplementation on
Growth
Three studies addressed the effect of iron supplementation on growth in exclusively breastfed infants (Fig. 5). Iron supplementation had no effect on length gain (MD = −0.01 cm; 95% CI −0.08 to 0.06 cm; p = 0.77), but had a significant negative effect on weight gain (MD = −0.04 kg; 95% CI −0.07 to −0.01 kg; p = 0.003) and head circumference gain (MD = −0.14 cm; 95% CI −0.18 to −0.09 cm; p < 0.00001).

Effects of iron supplementation on
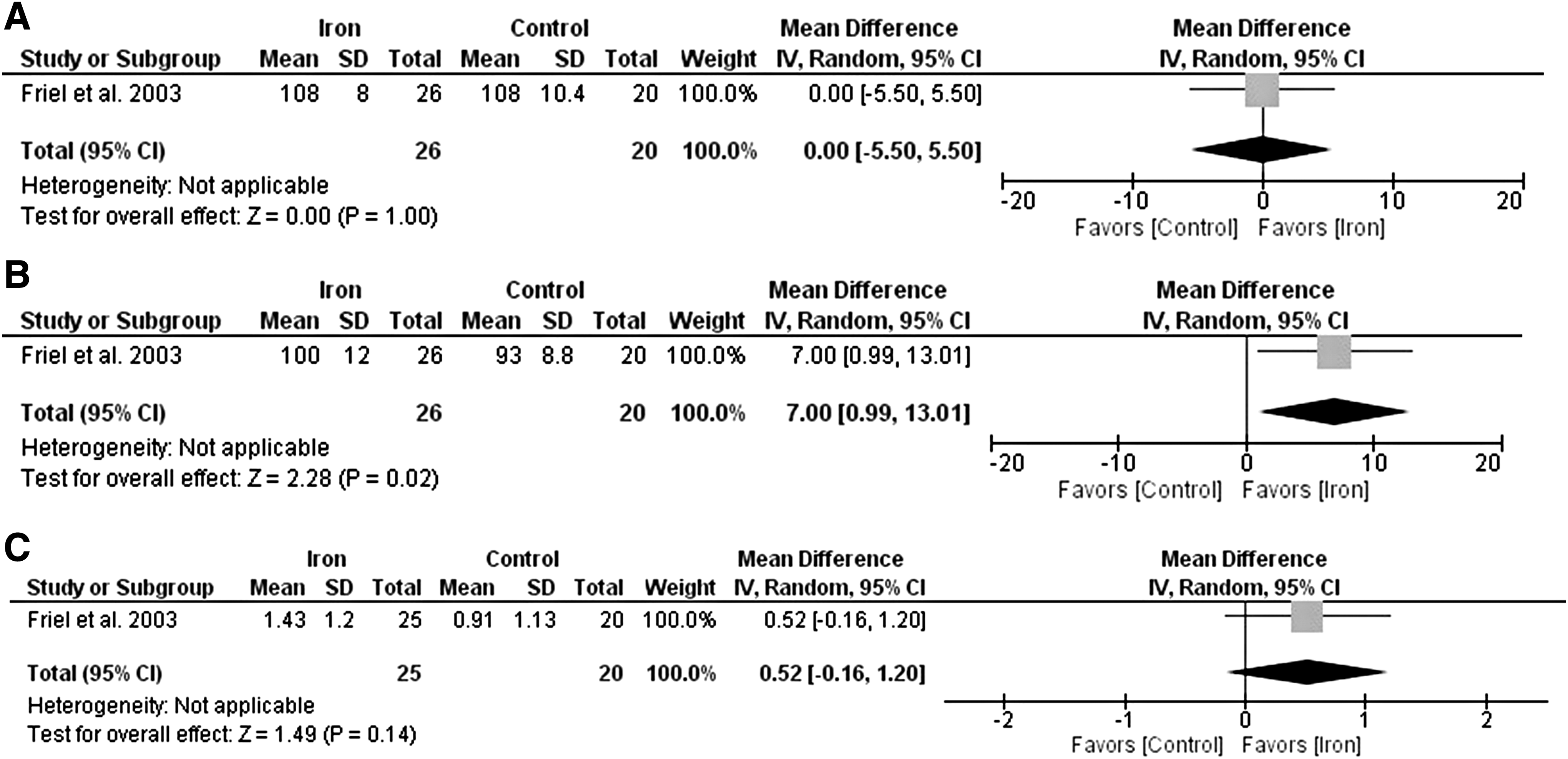
Mental and visual development
Mental and psychomotor developmental indices and visual acuity at 13 months of age were assessed using the Bayley Scales of Infant Development and the Teller visual acuity in the included RCT. Outcomes were analyzed by intention to treat. The Bayley psychomotor developmental index was significantly higher in the iron supplement group (MD 7.00, 95% CI 0.99–13.01; p = 0.02) (Fig. 6). There were no significant difference in Bayley's mental development index (MD 0.00, 95% CI −5.50 to 5.50; p = 1.00) and visual Z-scores (MD 0.52, 95% CI −0.16 to 1.20; p = 0.14) in infants receiving iron compared with control.
Effects of iron supplementation on
Adverse effects
Four studies presented adverse effects data, but only three presented extractable data. One RCT reported that there were no episodes of diarrhea related to iron supplementation, 15 whereas the other two RCTs reported no infections related to iron supplementation.14,17
Discussion
This study is the first systematic review and meta-analysis to analyze the effect of daily iron supplementation in healthy exclusively breastfed infants. Previous systematic reviews evaluated the effects of daily iron supplementation in low birth weight infants 18 and 2- to 5-year-old children. 19 However, the specific effects of daily iron supplementation on healthy exclusively breastfed infants have not been addressed in other studies. Our study extends the literature in this specific population, which could be used by policy makers and clinicians.
Control group participants of included studies were at high risk of developing ID/IDA (12% prevalence of ID and IDA at endpoint in the control groups of the meta-analysis). Daily supplementation of ferrous sulfate at a dose of 1 mg/kg/day or 7.5 mg/day did not significantly reduce the incidence of ID/IDA (7% prevalence of ID and IDA at the endpoint in the iron supplementation groups of the meta-analysis). However, a 42% reduction in the prevalence of ID/IDA should merit the attention of clinicians since it has been shown that infants with ID/IDA can be subjected to irreversible negative cognitive development and altered neurological functioning in adulthood.5–7,20
Although there were no significant differences in ferritin or hemoglobin levels in both groups, those infants with iron supplementation had higher MCV compared with infants in the control group. MCV is reduced in ID.21,22 Taken together with the ID/IDA results, iron supplementation did improve iron status of breastfed infants.
This meta-analysis found that daily iron supplementation resulted in slower weight gain and head circumference gain over the duration of treatment. There was no effect on length gain. It has been suggested that iron supplementation may impair the growth of infants by inhibiting the absorption of other essential nutrients. 23 Alternatively, while the connecting mechanism between growth deficit and iron is not entirely known, 24 some recent studies suggest an association between obesity and ID in children.25–27 Taken together, it is unknown whether decreased weight gain and head circumference gain in infancy will impair long-term growth of infants or is an indicator for developing obesity. These data reinforce the need for a long-term iron supplementation trial to address these questions.
There was a statistically significant positive effect of iron supplementation on the Bayley psychomotor developmental index. This finding supports the rationale that iron is needed for the rapidly growing brain in the first year of life as it is involved in the development of brain and neural pathways. 28
The greatest concern of any supplemental intervention is that it may increase morbidity; however, there is no convincing evidence that iron treatment results in an increase in infant morbidity from this meta-analysis or previous reports.19,23
Study limitations
Limitations of this meta-analysis are that the sample sizes of the studies analyzed are small and only four RCTs were eligible for the meta-analysis. Among the eligible studies, the reported outcomes of the long-term effect of iron supplementation on mental development of breastfed infants are limited, and could restrict the outcome assessment.
Conclusions
This systematic review confirms that for healthy exclusively breastfed infants, daily iron supplementation results in increased MCV levels and has a beneficial effect on cognitive development. However, iron supplementation can slow the physical growth of infants. There was no evidence to suggest that iron supplementation could cause other adverse effects.
Authors' Contributions
C.C., and F.J.K. designed research; C.C. and G.M. conducted research; C.C., G.M., E.P., and F.J.K. analyzed data; and C.C. wrote the article. F.J.K. had primary responsibility for the final content. All authors read and approved the final article.
Ethical Approval
This article does not contain any studies with human participants performed by any of the authors.
Footnotes
Disclosure Statement
No competing financial interests exist.