
Abstract
Abstract
Objective:
The study aims to assess effects of having preterm infants smell amniotic fluid, mother's milk, and mother's odor during heel stick procedure on pain, physiological parameters, and crying duration.
Materials and Methods:
The study was a randomized controlled experimental research. The population of the study was made up of preterm infants receiving treatment and care at a neonatal intensive care unit, where the study was conducted between January 2015 and March 2016. The study was performed with 85 preterm infants who met the selection criteria. Infants were randomized into four groups: amniotic fluid, mother's milk, mother's odor, and control group. Data obtained were analyzed by percentage distributions, means, standard deviation, chi-square test, Kruskal–Wallis, and Dunnett's test.
Results:
While no significant difference was found between the groups in terms of total preterm infant pain profile score before, during, and after the heel stick procedure (p > 0.05), a significant difference was found in terms of SO2 values (p < 0.05) and the difference was caused by the amniotic fluid group. Although no significant difference was found between the groups in terms of crying duration (p > 0.05), the amniotic fluid group had the lowest score, followed by the mother's milk group, the mother's odor group, and the control group.
Conclusions:
Amniotic fluid, mother's milk, and mother's odor were not effective in preterm infants during painful procedures.
Introduction
W
Some studies have focused on how to calm newborn infants during procedures causing pain. These calming methods for infants fall into two major groups: pharmaceutical and nonpharmaceutical methods. 3 The latter are frequently investigated by researchers because of the absence of biological harm. Many different methods have been discussed frequently in the literature, with regard to infants' sense of taste,4–6 sense of smell, 7 sense of hearing, 8 sense of touch, 9 and their vision. Previously published studies have shown that the sense of smell is the most mature of the senses at birth. Newborn infants can recognize the smell of their mother's nipples and are able to drink breast milk within their first few days of life. 10
The olfactory system is of special interest in this regard because, in comparison with the other senses, such as vision, it is already a notably developed system at the time of birth. Infants are not only able to tell the difference between the maternal and nonmaternal breast, milk, neck, and axillary odors the first few days after being born, but they also show a preference to orient toward their mother's amniotic fluid, which is an odor that they have come into contact with prenatally through the mother's diet11,12 and their mother's breast when it has been treated with her amniotic fluid. 13 This preference for odors related to the maternal environment has clear adaptive qualities in terms of ensuring efficiency in nursing. 14
The early sophistication of the olfactory sense as well as its significance for survival have led to the suggestion that maternal odors could have soothing qualities for early infants. A number of studies have observed that spontaneous crying is reduced when newborns are exposed to the odor of their mothers' amniotic fluid odor or different maternal odors15,16 In the second study referred to, it was found that infants became calmer when presented with the odor of their own mother's milk or even that of another mother. With regard to pain, Mellier et al. offered maternal milk or artificial milk odor to full-term newborns while drawing blood on the dorsum of the hand. Their finding was that during the recovery period breast-fed infants cried less when they were presented with the odor of their mother's milk odor than bottle-fed infants presented with their formula or to infants in the control group. 17
Several studies have recently investigated the pacifying effects of maternal odors on newly born infants.16,18 Rattaz et al. reported that infants' pain responses, such as head movements, decreased when they were exposed to odors from their mother's milk. Their report did not, however, examine the effects of odors from another mother's milk or formula milk. In the present study, we examined the effects of odors from mother's milk, other mother's milk, and vanillin on infants' behavioral responses to pain, including motor activity, crying, and grimacing to compare the relative effects of these odors. 18
When the mother is absent, sensory stimuli, including the mother's voice and her scent, have had demonstrable positive effects on preterm infants. Infants in the NICU can be exposed to a wide range of negative olfactory experiences. One study showed that preterm infants faced exposure on an average several thousand times to negative nosocomial odors (skin preps, alcohol pads, and adhesive remover) while staying in hospital. 19 The ability to detect and discriminate between odors develops between 28 and 29 weeks gestation and there is evidence that supports the conclusion that infants become familiar with and establish preferences for odors such as their amniotic fluid, their mother's breast milk, and her specific scent.20,21 Research has demonstrated that infants react to sensory stimulation with both positive and negative behaviors. The benefits from exposure to the odors which they prefer include better self-regulation, reduction in pain, and a decrease in cases of apnea.22–24 It is necessary for healthcare professionals providing care in the NICU to limit the number of noxious stimuli and to offer care that also utilizes positive sensory stimulation.
The study aims to assess effects of having preterm infants smell amniotic fluid, mother's milk, and mother's odor during heel stick procedure on pain, physiological parameters, and crying duration.
Methods
Setting and sample
The study was a randomized controlled experimental research. The population of the study was made up of preterm infants receiving treatment and care at a NICU, where the study was conducted between January 2015 and March 2016. The sample initially consisted of 97 preterm infants who met the case selection criteria and the infants were assigned to groups randomly. However, the total number of infants decreased to 85 (amniotic fluid: 21, mother's milk: 22, mother's odor: 20, control group: 22) due to infants excluded from the study (Fig. 1). Randomization was performed using a computer program. Power analysis at the end of the study, it was found that the power was 0.91 for 123 preterm infants with β = 0.20 and α = 0.05 risk at 0.05 significance level.
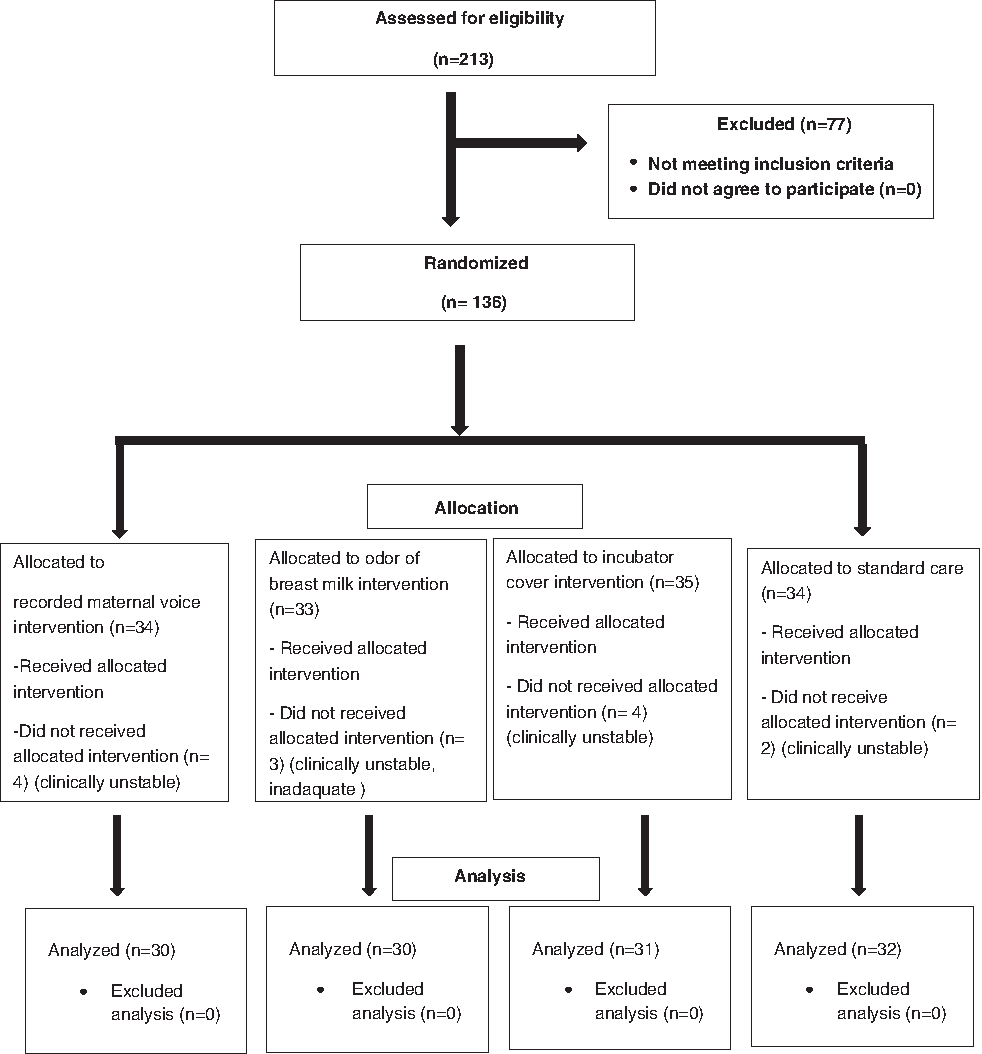
Diagram showing the flow of participants.
Preterm infants were eligible to participate in the study if they had been born between 28 and 36 weeks of gestation and were not eligible if they had congenital anomalies or genetic disorders and required surgery, or had an Apgar of less than six at 5 minutes.
Exclusion criteria (similar to those used in previous studies) were necrotizing enterocolitis, chromosomal anomalies, craniofacial malformation, respiratory distress syndrome, bronchopulmonary dysplasia, need for mechanical ventilation, neonatal seizures, intracranial hemorrhage, periventricular leukomalacia, or culture-positive sepsis or meningitis at study screening, and any pharmacological or nonpharmacological pain reliever 4 hours before the procedure.
Data collection
Preterm infant information form
Includes items on the newborn's gender, gestational age, birth weight, length, head circumference, and Apgar score.
Preterm infant follow-up form
This is the form in which the physiological measurements (heart rate and oxygen saturation) of infants are recorded.
Preterm infant pain profile
This scale was developed by Stevens et al. 25 and its Turkish validity study was conducted by Akcan and Yiğit. 26 In this form, the following seven indicators are scored to evaluate the infant's pain during the procedure: gestational age, behavioral state, maximum heart rate, minimum oxygen saturation, brow bulge, eye squeeze, and nasolabial furrow. Each item is scored between 0 and 3, from that which is the least affected to that which is the most affected by the procedure. Validity and reliability analyses were first performed in order that the form could be used. According to preterm infant pain profile (PIPP) guidelines, the gestational age must be between ≥28 and ≤36 weeks, and the behavioral state must be scored depending on criteria such as active–quiet, awake–sleep, eyes open–closed, and the display of facial movements. Moreover, an increase in the heart rate must be scored in the range of 0–25 beats/min, and a decrease in oxygen saturation is assessed between 2.4% and 7.5% per minute. The final total score is determined with regard to the aforementioned parameters to find the infant's pain level score; the highest score possible is 21 and lowest score is 0. The level of pain is judged mild if the total PIPP score is between 0 and 6 points, moderate if it is between 7 and 12 points, and severe if it is between 13 and 21 points.25,26
Duration of the crying
The researcher measured the duration of the heel stick, from the beginning of lancet insertion to the placement of the plaster in seconds. The amount of time spent crying (in seconds) was also measured. To this end, crying beginning from the onset of the lancet insertion until all crying had ceased, up to a maximum of 3 minutes, as some infants cried for longer than 3 minutes, was recorded on video and later evaluated by the same researcher. The total length of crying was defined as the total time during which the subject made audible vocalizations of distress during the 3-minute observation period. 27
Ookie mom-scent doll
The word Ookie means “little” or “tiny” in Dutch. Ookies have been used for newborns since 1997. An Ookie is a doll with satin edges, made of 100% cotton flannel, is 35 × 40 cm in size and comes in various colors. Because it is of a high quality it is easy to wash, dry, and sterilize the doll. The Ookie does not have any specific identifying characteristics such as a face, ascribed race, or gender. It is a useful tool for providing the mother's scent to babies who have been separated from their mother either at home, or who are undergoing care in a different environment, as well as infants in hospital. To transfer the mother's scent, the mother sleeps with the doll for one night after birth, and the doll is then put in position near to the baby.
Procedure
All heel stick procedures were carried out during the day shift by the same nurse, who had 7 years of NICU experience. No pharmacological or nonpharmacological pain relief was given to infants under heel stick in the NICU where the study was conducted. All factors that could affect the level of pain of preterm infants in intervention and control groups during the study were standardized. This included ensuring that the procedure was performed while the preterm infant was not crying, and if he/she was crying, then a waiting period of 2 minutes was applied. Before the procedure, the area was cleaned from the center to heel using 70% alcohol as a skin antiseptic in all preterm infants. The procedure was performed after at least 90 seconds had elapsed. The heel stick procedure was applied for metabolic screening on the second day following the admission of preterm infants to the unit. Lancet was used for all infants during the heel stick procedure.
The video recording was made by the researcher and was begun 1 minute before the procedure, during the procedure, and lasted for 5 minutes after the procedure for both groups. Physiological parameters were measured through continuous monitoring. Heart beat and SO2 were recorded from the monitor.
Intervention
The preterm infants, in conformity with the selection criteria of the study, were all considered stable. Interviews were conducted with the families of infants, who had been stabilized during the first 24 hours, and they were informed about the study. The written permission of the families who had agreed to participate was obtained, and their infants were included in the study. Families were informed that the data would be kept confidential and only be used for this study. Before the study, NICU nurses and mothers were informed about the study and the interventions to be conducted. The interventions, which were applied to the preterm infants who made up the control group and experimental groups of the study, were as follows:
Preterm infants in the control group
Preterm infants in this group received routine nursing care from the clinic. Routine nursing care includes such caregiving procedures as assessing vital signs, temperature checks, feedings, girth measurements, and diaper changes. However, no intervention was made during the heel stick procedure for the infants in the control group. Video was recorded of the baby before, during, and after the procedure.
Preterm infants in the mother-odor group
An Ookie doll was given to the mother of each premature infant in this group and the mother was asked to keep the doll on her chest for one night (∼8 hours), in such a way to make it touch their naked skin. Ookie absorbed the mother's scent owing to its smell-absorbing nature and then was placed near the infant during the heel stick the next morning. In this way, infants in this group were exposed to their mother's scent. The Ookie dolls employed for each discharged preterm infant were sterilized in the sterilization unit of the hospital (at 121°C in autoclave for 1 hour) inside disposable sterilization bags. The doll was positioned 5 cm away18,28 from the infant 15 minutes before the procedure, in order that the infant could begin to smell it. The infant continued to smell it during the procedure and for 15 minutes after the procedure. Video was recorded of the baby before, during, and after the procedure.
Preterm infants in the breast milk odor group
The breast milk of the mothers of each preterm infant in this group was taken using a breast pump when the mother became stable. About 5 cc of the milk sample was poured into a sterile sponge 15 minutes before the procedure, placed 5 cm away18,28 from the infant, in order for the infant to begin to smell it. The baby was given a side position during the procedure and the odor material was placed on that side by another nurse. If the baby turned his head, the nurse carried the material to the side she was turned. The infant continued to smell it during the procedure and for 15 minutes after the procedure. Video was recorded of the baby before, during, and after the procedure.
Preterm infants in the amniotic fluid group
The preterm infants in the amniotic fluid group were exposed to the smell of their own mothers' amniotic fluid. About 8–10 cc of amniotic fluids were taken by the doctor into a 20-mL injector during cesarean section and kept at 8°C in the refrigerator until cannulation administration. In the preterm infants hospitalized in the NICU, amniotic fluid was fixed 5 cm away18,28 from the infants' noses by pouring it onto a big piece of sterilized gauze sponge 15 minutes before heel stick. The infants were exposed to the smell of amniotic fluid during the procedure and for up to 15 minutes after the procedure. Video was recorded of the baby before, during, and after the procedure.
Statistical analysis
Video recordings for both the experimental and control groups were viewed after the procedure by one NICU nurse and the researcher to evaluate levels of comfort. The researcher's observations were used in the data analysis, as there was no statistically significant difference based on the results of the inter-observer agreement for the assessment of pain levels. The assessment of pain was performed before, during, and after the heel stick.
The researcher viewed the video recordings after the procedures to evaluate the pain levels. Data were analyzed using the Statistical Package for Social Sciences (SPSS) 18.0 statistical analysis software packages. Percentage distribution, mean value, standard deviation, chi-square value, Kruskal–Wallis, and Dunnett's test comparison between groups was used for the statistical analysis of the data.
Ethical considerations
The written permission of the hospital and ethical consent from the Ethics Committee were obtained to conduct the study. The parents of the infants were informed of the aim and protocol of the research (why the babies were being video recorded, and for what purpose these recordings were going to be used), and both their written and oral consent were received. In the study, the related ethical principles of “Informed Consent Policy,” “Volunteer Policy,” and “Privacy Protection Policy” have been fulfilled since the use of human subjects requires the protection of individual rights.
Results
In the study, no statistically significant difference was found between the preterm infants in the control and experimental groups in terms of gender, gestational age, birth weight, birth height, birth head circumference, diet, the Apgar score at the 5th minute, and diagnosis (p > 0.05; Table 1). These results indicate that the intervention and control groups were similar in terms of variables.
χ2 = Fisher's exact test for categorical variables.
Kruskal–Wallis test.
Pain levels of the babies in the breast milk smell group during the procedure were determined to be lower than the infants in the control and the other groups, however this difference was not significant (p > 0.05; Table 2).
Kruskal–Wallis test.
PIPP, preterm infant pain profile.
It was found that there were no significant differences between the groups in the duration of crying during and after the procedure on the infants (p > 0.05). The amniotic fluid group was found to have the shortest crying duration after the procedure (Table 3).
Kruskal–Wallis test.
No significant difference was found between the heart rates of the infants in the experimental and control groups before, during, and after the heel stick (p > 0.05; Table 4).
Kruskal–Wallis test.
The oxygen saturation during the procedure was found to be 90.22 ± 7.54 for the preterm infants in the mother's milk group, 88.25 ± 5.30 for the preterm infants in the mother's odor group, 93.19 ± 5.02 for the preterm infants in the amniotic fluid group, and 89.00 ± 8.17 for the preterm infants in the control group. It was found that there is a significant difference among the SO2 levels during the procedure of the infants between the groups (p < 0.05). The significant difference between the groups in terms of SO2 values was found to be caused by the amniotic fluid group according to the results of the post hoc analysis (p < 0.05; Table 5).
Kruskal–Wallis test.
Advanced analysis result (Dunnett's tests).
Discussion
Babies are liable to encounter many negative olfactory stimuli in NICU. These may include strong perfumes or scented aftershave, alcohol, cleaning chemicals, alcohol-based hand rubs, and oral medications. These odors should be reduced and fragrances with a positive stimulus such as substances associated with breastfeeding or those which smell of the parents should be used as a counterweight.29–31 In this way negative physiological reactions in infants will be decreased, and they will develop a sense of security, making the development of the bond between babies and parents easier. In addition, they will be less likely to experience negative feelings. For example, if a baby experiences constant smell of alcohol during the process of collecting blood, he/she will come to expect pain when encountering the smell of alcohol and may begin to cry.30,32
The fetus inhales the odor of amniotic fluid during the intrauterine period and this is a chemical stimulus for him/her. It has been seen that this smell can help the baby to become calmer and adapt to new and different environments in the period after birth. 15 In the literature it has been stated that smells related to mothers are associated with trust and that they decrease pain and stress in newborns.10,16,18,33,34
In the studies conducted using the heel lance it was determined that newborns smelling their own mothers' breast milk felt significantly less pain and had fewer symptoms of uneasiness/agitation.10,18 In Akcan and Polat's study it was also stated that after the heel lance procedure, pain was less in the newborns in the breast milk and amniotic fluid group compared with the lavender and control groups 28 These studies support the results of the present study. Badiee et al. studied the effect of the odor of breast milk on preterm infants' reaction to pain. They used PIPP to measure pain. The main result of their study was a PIPP reduction as a result of smelling breast milk. 35 All the studies have concentrated on the calming effects of the smell of breast milk, and did not discuss variations in vital signs in a detailed way. It could thus be maintained that smells of mother, a figure with whom newborns feel safe, are effective when used in practices which cause stress and pain. Marlier et al. reported that olfactory stimulation with vanillin was effective on respiration rate of preterm infants and reduced apnea frequency and severity. 22 In our study, no significant difference was found between mother's milk, amniotic fluid and mother's odor during the heel stick procedure. However, the mother's milk group had the lowest PIPP score during the procedure. The reason for this, the number of infants in each group was low. Additionally, all of our smells belonged to the mothers, therefore, the PIPP scores of the infants in the experimental group were similar but lower than the control group. The fact that the lowest pain scores are in mother's milk odor group remembered what his mother's milk for babies is so effective and important.
In their study, Varendi et al. 15 found that newborns smelling amniotic fluid cried for shorter period of time than those in breast milk smell and control groups. Another study investigating the effect of smells on pain determined that if crying infants were made to smell an cloth belonging to their mothers, a cloth from another mother, and a cloth that had never been used, their responses were more positive with regard to the smell of their own mothers. 16 In Goubet et al.'s study, 33 it was stated that the newborns who were made to smell familiar scents during the heel lance cried 32% less than those in the control group and the group which was made to smell vanilla. Rattaz and coworkers 18 determined that smelling breast milk and vanilla during the heel lance decreased the number of grimaces newborns made and that only the smell of breast milk had the effect of decreasing neonatal stress after heel lance. In their study, Goubet and coworkers, 36 concluded that, as a result of presenting the smell of vanilla to newborns during the heel lance and venous blood-letting, presenting them with a perfumed scent for the first time and presenting them with no scent, newborns given a familiar scent grimaced and cried less. This and previous studies suggest that making newborns smell the scent of their mothers is an effective method for relieving the pain that newborns feel during procedures.
In this study, no significant difference was found between the heart rates of the infants in the experimental and control groups before, during, and after the heel stick. In Akcan and Polat's 28 study it was also stated that the smells of lavender and breast milk prevent increased heart rates and falling oxygen saturation during invasive procedures on newborns more than the smell of amniotic fluid or no smell. Örs et al. 37 studied the pain of newborns and found that the changes in the heart rates of the newborns given sucrose were lower than those who were given breast milk. Aoyama et al. 38 determined that the smell of breast milk increased blood flow oxygenation in the orbitofrontal region more than other smells. Yılmaz and Arıkan 39 found that the heart rates and oxygen saturation levels of newborns given sucrose during heel lancing was higher than those of newborns who were given breast milk and pacifiers.
Limitations
The most important limitation of the study is that amniotic fluid could only be obtained from infants born by cesarean section and obtaining this fluid is difficult. Another limitation is that there was no blinding because the evaluation of pain was made by viewing the videos that had been made. Since the Ookie doll and gauze sponge were positioned near to the noses of infants during evaluation of PIPP and could be seen from videos, it was easily understood which group they belonged to. However, the video recordings of both groups were viewed independently by one NICU nurse not involved in the research, and the principal researcher (D.K.A.) after the procedure to evaluate the pain, and the researcher's observations were subsequently used for data analysis as there was no statistically significant difference in the result of the interobserver agreement test carried out by both for the pain.
Conclusion
This study was conducted to determine the effects of having preterm infants smell amniotic fluid, mother's milk, and mother's odor during heel stick procedure on pain, physiological parameters, and crying duration. Amniotic fluid, mother's milk, and mother's odor were not effective in preterm infants during painful procedures. Nurses could train mothers how to pump their breast milk in order for it to be used as an odor stimulus as well as being used to nourish their infants.
Health professionals working with neonates should be able to assess pain status of neonates using scales developed for this purpose, follow heart rate and oxygen saturation, and follow the pain status of neonates regularly and constantly as the 5th vital sign. The health staff should support the neonatal and the family for effective pain management and use nonpharmacological pain relief methods efficiently before, during, and after the heel stick procedure.
Footnotes
Acknowledgments
The authors thank the parents of the infants who participated in the study and nurses employed at the NICU.
Disclosure Statement
No competing financial interests exist.