
Abstract
Abstract
Background:
Breastfeeding education is known to be insufficient in pediatric (PEDS) training and is, in part, responsible for suboptimal rates of breastfeeding. No recent studies about the level of education provided to family medicine (FM) and obstetrics–gynecology (OB) residency trainees are available.
Objectives:
This study was conducted to investigate breastfeeding education and support services provided to FM and OB residents in the United States. The results were compared with a 2011 study of PEDS residents.
Methods:
A cross-sectional study was conducted using a web-based survey emailed to program directors (PDs) of FM and OB residency programs in the United States.
Results:
Eighteen percent of PDs (95 of 515) completed the survey. Of these, 88% answered questions regarding education and support services provided. A median of 23 hours of breastfeeding education is provided to OB residents (4-year program) and 8 hours provided to FM residents (3-year program). In comparison, PEDS programs reported a median of 9 hours. The most commonly used settings included lectures with faculty and lactation consultants, similar to the PEDS study. Approximately 75% of respondents cited barriers to educating residents, with limited resident time being the most common. Eighty-one percent of respondents identified breastfeeding rooms as the service most frequently provided to residents who breastfeed.
Conclusions:
FM and PEDS residents are provided similar amounts of breastfeeding education, while OB programs provide more education, but in different settings. Reported barriers to this education are similar in all specialties. Support services are more commonly provided in PEDS programs.
Introduction
T
Exclusive breastfeeding for the first 6 months of life is recommended by the AAP, American College of Obstetricians and Gynecologists (ACOG), and the American Academy of Family Physicians (AAFP) for almost all infants.1,3,4 Breastfeeding rates have continued to increase in the United States over the last few decades; however, the goals set by the U.S. Department of Health and Human Services through their Healthy People 2020 objectives have not been achieved. 5 Although 81.1% of infants have been breastfed at some point, only 22.3% are breastfed exclusively through 6 months of age, short of the goal of 25.5%. 4 Additionally, there is discord between racial populations as it relates to breastfeeding rates where black women have lower rates of initiation (66%) and continued exclusive breastfeeding at 6 months (15%) in comparison with white (84%, 27%) and Hispanic (83%, 19%) females. 6 These lower rates have been identified as contributing factors to the higher sudden infant death rate and other disease processes with high morbidity and mortality. 7 Similar low rates occur in mothers with lower level of education. 6 This relates to physicians in training as it is known that residents provide care to these high-risk populations.8,9
The movement to support the practice of breastfeeding is international as well as national. In 1991, the World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) started a global program entitled the Baby-Friendly Hospital Initiative (BFHI) to encourage and recognize hospitals and birthing centers that offer an optimal level of care for infant feeding and mother/baby bonding.10,11 Medical centers are now developing new ways of delivering care to new mothers and their infants. The BFHI assists hospitals in providing the skills, knowledge, and resources that improve initiation and continuation of breastfeeding. This includes educating healthcare providers in breastfeeding management as it has been shown that professional support increases breastfeeding rates. 12
It has been reported that prenatal breastfeeding education increases rates of exclusive breastfeeding through 6 months.13–16 The timing of the decision to breastfeed correlates with the duration of exclusive breastfeeding; antepartum decisions correlate with a higher likelihood that the mother will exclusively breastfeed until her infant is 6 months of age.17,18 Lack of physician knowledge about breastfeeding correlates with decreased initiation and continuation of breastfeeding by mothers. 19 Thus, adequate education of residents who will be caring for mothers in the antepartum, intrapartum, and postpartum periods is critical. A 2011 study of pediatric (PEDS) residents in the United States concluded that there is a universal lack of appropriate education for these pediatricians to competently counsel mothers on breastfeeding. 20 Previous studies that focused on physicians who provide care in both the antepartum and postpartum periods, family medicine (FM) and obstetrics-gynecology (OB) residents, concluded that there was an educational deficit.21–23 It is likely that this has not changed, as illustrated by a more recent study reporting that 40% of participating FM and OB residents believed formula and breast milk are comparable. 24 However, no recent study has been done measuring education given to FM and OB residents.
The goals of this study were to investigate how much and in what settings FM and OB residents receive breastfeeding education, to evaluate what support services are being provided to residents who breastfeed, and to assess satisfaction of program directors (PDs) with the education and support services provided to their residents.
Methods
Design
A cross-sectional study implementing a web-based survey was conducted to investigate breastfeeding education and support services provided to FM and OB residents in the United States. Results were compared with a study published in 2011 in the Journal of Academic Pediatrics by Osband et al. describing breastfeeding education and support services provided to PEDS residents. 20 With the permission of Dr. Osband, our survey was designed to be similar to the Osband et al. study so that the results could be compared.
Subjects and data collection
All PDs of FM and OB residency programs (n = 539) in the United States were eligible to participate in the study. A list of all programs and their respective PDs for the 2014–2015 academic year was compiled from lists provided by the Accreditation Council of Graduate Medical Education (ACGME) website. 25 The survey was submitted to the Office of Research Subject Protection Institutional Review Board (IRB) at the University of Texas Medical Branch and deemed exempt from IRB review. After taking into account multiple programs with the same director, emails of PDs not listed, and email delivery errors, a total of 515 surveys were sent (331 FM and 184 OB).
Background information about the study and a hyperlink to the 17-question survey were sent by email. The survey was constructed using a web-based survey program and was available for completion from November 24, 2014, to January 24, 2015, with one reminder email during the 2-month time period. Completion of the survey implied consent to participate in the research. The demographic questions included program size, female representation within the program, geographic setting of the program, and baby-friendly hospital status as defined by WHO guidelines (Table 1). Questions about education included time spent in prenatal settings, hours spent on breastfeeding education in various settings, barriers to breastfeeding education, and overall satisfaction with the education given to residents. Finally, questions about support services provided to residents who breastfeed were also included.
Results
A total of 95 surveys were completed, 57 representing FM and 38 representing OB (response rate of 18.5%). Respondents reported a mean program size of 22 residents. FM programs were more likely to be located in suburban areas or rural areas than OB programs. Approximately 46% of the programs reported that their primary teaching hospital is classified as baby-friendly as defined by WHO guidelines, although verification of this status was not required. Both disciplines reported spending time in prenatal and postnatal settings, including prenatal clinic visits and newborn nursery rotations.
Breastfeeding education, barriers to education, and support services
Eighty-four of the 95 respondents provided information regarding resident breastfeeding education. A median of 23 total hours of breastfeeding education over the course of the residency program is provided to OB residents (range 0–70, SD 14.3), while 8 hours is provided to FM programs (range 0–94, SD 17.6). In comparison, PEDS programs reported providing a median of 9 hours (range 0.5–86). 20 The most commonly used settings for breastfeeding education in both FM and OB included lectures with faculty, and continuity clinic, consistent with the published PEDS study where programs utilized lectures with faculty, continuity clinic, and rounds with faculty (Fig. 1). 20 Other settings used were rounds with lactation consultants, observed structured clinical examination, attending a specialty clinic in breastfeeding medicine, and using web-based training. With respect to the number of education hours provided in each individual setting, FM and OB were similar in all settings except continuity clinic, where OB provided more breastfeeding education hours (Fig. 2). The PEDS study also reported continuity clinic as their main source of education, along with lectures with attending faculty, each with a median of two total hours over the course of the residency. 20

Breastfeeding education settings utilized by specialty. Settings utilized by specialty. Use of rounds with faculty, lectures with lactation consultants, and continuity clinic differed significantly among specialties (χ2 analysis). PEDS information extracted from the study by Osband et al. 20 FM, family medicine; OB, obstetrics–gynecology; PEDS, pediatric.

Total hours of breastfeeding education by setting. Hours of breastfeeding education dedicated to each setting by discipline using box-and-whisker plot. The full range of hours reported is denoted by each horizontal line with median, first quartile, and third quartile values illustrated. Similarities were noted in all settings with the exception of continuity clinic, used more heavily in OB residencies.
Barriers to breastfeeding education by programs were universally reported (Fig. 3). Limited resident time was the most common, reported by more than 60% of all programs. This was followed by limited faculty time and lack of faculty with significant knowledge about breastfeeding.
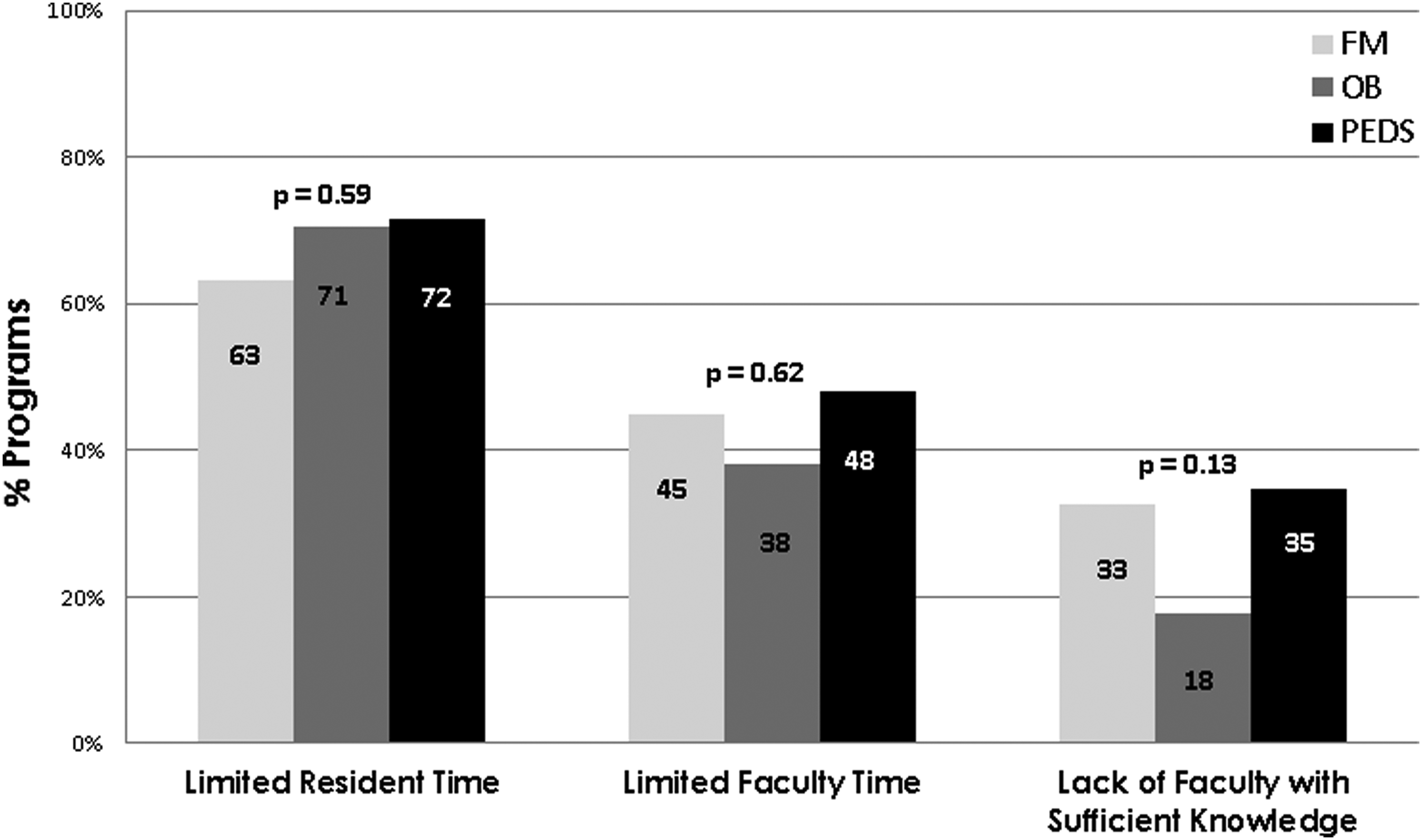
Barriers to breastfeeding education. Comparison of perceived barriers to resident breastfeeding education. There were no differences (χ2 analysis). PEDS results extracted from the study by Osband et al. 20
Support services for breastfeeding residents varied widely (Fig. 4). At primary institutions, the vast majority of programs provide breastfeeding rooms for mothers to pump. Most OB and PEDS programs provide breast pumps; FM programs were significantly less likely to do so. 20 This difference was also apparent in the designation of storage for breast milk.
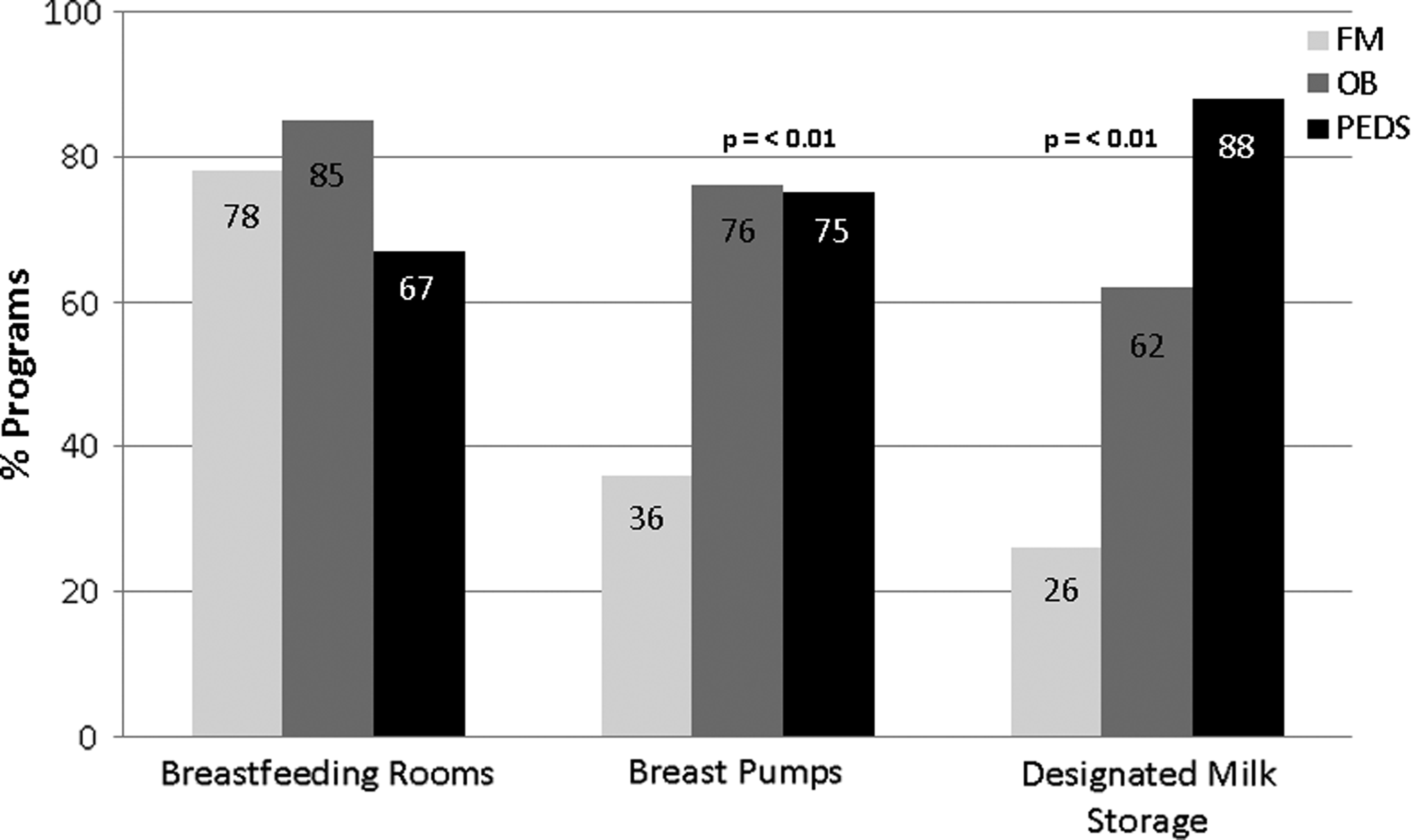
Support services for breastfeeding mothers. Services provided to resident breastfeeding mothers in respective specialties. Significant difference noted in providing breast pumps and designated milk storage where FM is far behind OB and PEDS (χ2 analysis). PEDS data extracted from the study by Osband et al. 20
Discussion
FM and PEDS programs provide similar numbers of breastfeeding education hours. 20 In comparison, OB programs provide more than double the hours, even when considering the difference in residency program length. The settings in which these educational opportunities take place are similar; however, we did not ask if the program included a dedicated breastfeeding curriculum, nor if the curriculum was followed if present. There are no uniform standards for breastfeeding education in residency training.
PEDS programs in the previous study provide more services to residents who are breastfeeding than do either OB or FM, particularly with access to designated breast milk storage. 20 This is unexpected given the high rate of respondents being affiliated with baby-friendly institutions. While equipment services were quantified, time for use of these services was not queried. We inferred that time would be provided to residents if services are available.
We identified a few sources of bias in our study. While the response rate (∼20%) for our study parallels most survey-based studies, it was much smaller than the PEDS study (69.8%). 20 It is difficult to identify all contributing factors to this less than desirable response rate. The survey was sent to PDs directly, not through the Association of Pediatric Program Directors (APPD) listserv, which may have potentially lent to a lower response rate. Additionally, it is unknown whether participation was reduced due to lack of knowledge on the subject matter by PDs. There is a possibility that PDs are not fully aware of specifics regarding breastfeeding education. Results may have been more fruitful if the target audience had been neonatology faculty, hospitalist faculty, clinic faculty, and/or lactation consultants; however, this would not have allowed direct comparison with the PEDS study. 20 The response rate is adjusted for electronic mail delivery errors, but other electronic glitches such as direct entry into spam mail are also unknown.
Factors that could have influenced the data to represent more education and services were identified. A high percentage of respondents (46%) stated that their facility is baby-friendly, where only 340 baby-friendly (BF) institutions in the United States had this designation at the time of data acquisition. These facilities aim to foster exclusive breastfeeding and educating physicians in training is likely to be prioritized, especially in newborn rotations. Additionally, the vast majority of female respondents (95%) reported personal experience with breastfeeding, which may have contributed to the decision to participate in the study and positively affect results. In regard to satisfaction of education provided to residents, OB PDs were more satisfied than FM PDs (88% [30/34] of OB, in contrast to 37% [19/51] of FM). This may be due to the larger number of prenatal encounters that OB residents experience during the course of their training. Perceived satisfaction may lead to overestimation of time dedicated to education and may have also positively skewed data results.
Conclusions
Breast milk is the optimal source of nutrition for newborns and infants through age 6 months and continued for at least 1 year along with complementary foods. Although the AAP, ACOG, and AAFP have written policy statements supporting this, there appear to be deficiencies in the education and support services provided to residents to reinforce this. It is likely that this insufficient education limits residents' ability to educate mothers about breastfeeding initiation and duration and is contributing to national suboptimal rates of exclusive breastfeeding. Appropriate education of residents may increase these rates and address the public health issue. This study suggests the need for the establishment of a standard education model that can be implemented in all prenatal and perinatal specialties.
Footnotes
Acknowledgment
The authors would like to acknowledge Dr. David Rassin, PhD, Professor of Pediatrics at the University of Texas Medical Branch, for his help with the statistical analysis of this study.
Disclosure Statement
No competing financial interests exist.