In their article entitled “Teicoplanin Use During Breastfeeding,” Kaplan et al.1 describe the outcome of an infant who was breastfed during his mother's short-term intravenous teicoplanin treatment. The authors mention that the main limitation of their case was the lack of information on teicoplanin concentrations in the mother's milk and serum.
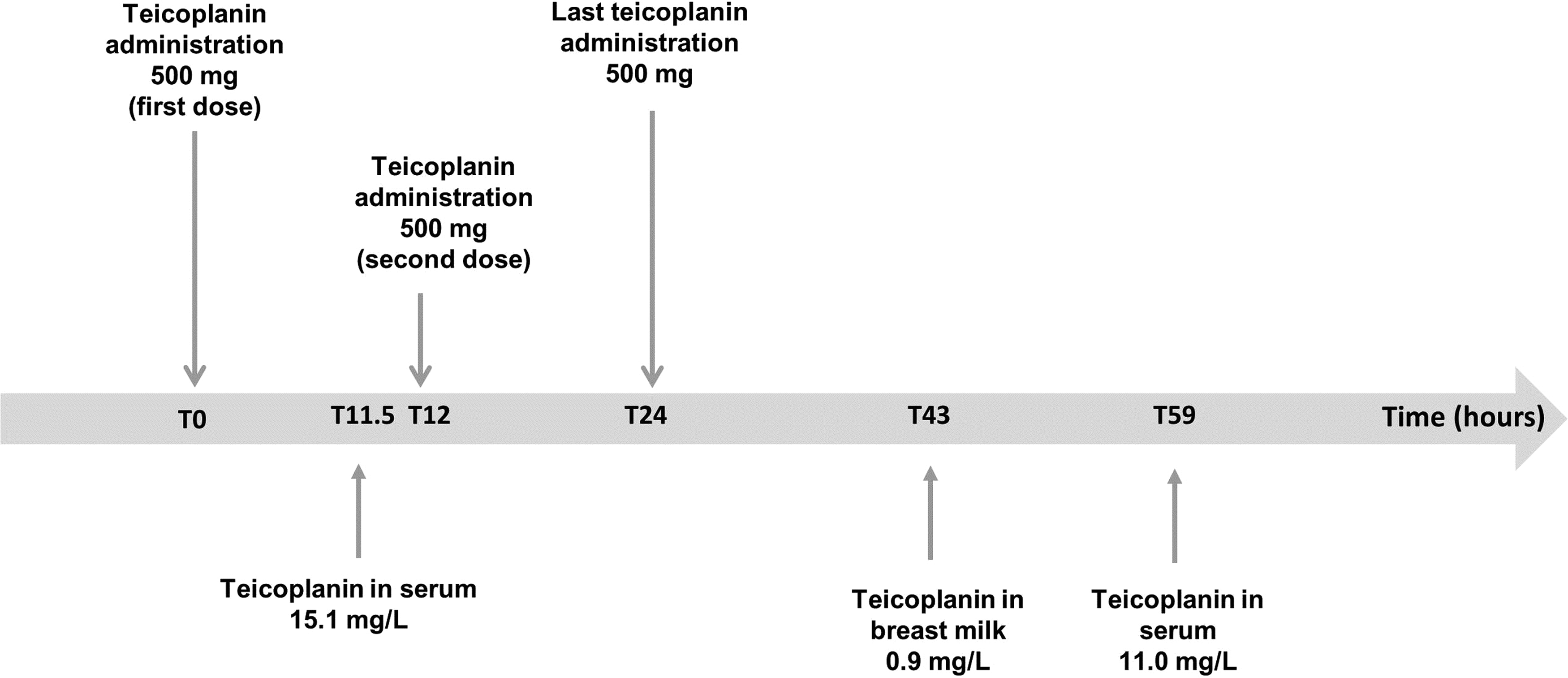
We report the case of a 32-year-old woman hospitalized in urology ward for pain at a left nephrostomy tube. She gave birth to a boy 2 months prior by cesarean section. She had an infected vesicocutaneous fistula. Cytobacteriological analysis showed methicillin-resistant Staphylococcus aureus sensitive to glycopeptides. She had been exclusively breastfeeding her child since birth. She was administered teicoplanin (Targocid®) at a dose of 500 mg twice daily (Fig. 1). Suspecting diffusion of teicoplanin into the breast milk, the clinicians (i) stopped (Fig. 1) administering the drug, (ii) switched to sulfamethoxazole + trimethoprim (Bactrim®), and (iii) measured the drug concentration in one milk sample from a full emptying of the breast (Fig. 1) 19 hours after the last administered dose. Clinicians checked maternal teicoplanin plasma concentration twice, before administration of the second dose and 35 hours after (Fig. 1).
Timing for drug administration, blood, and milk sampling.
The teicoplanin concentration was determined by liquid chromatography-tandem mass spectrometry (LC-MS/MS) method using an AB SCIEX API-4500 (Applied Biosystems/MDS Sciex, Foster City, CA) triple quadrupole tandem mass spectrometer. Our method used ristocetin as the internal standard and quantified only the major compound (teicoplanin A2-2) representing 50% of the whole of compounds (A2-1 to A2-5 and RS-1 to RS-42) found in plasma. Calibrators and quality controls contain the same repartition of teicoplanin compounds as in patients' plasma.
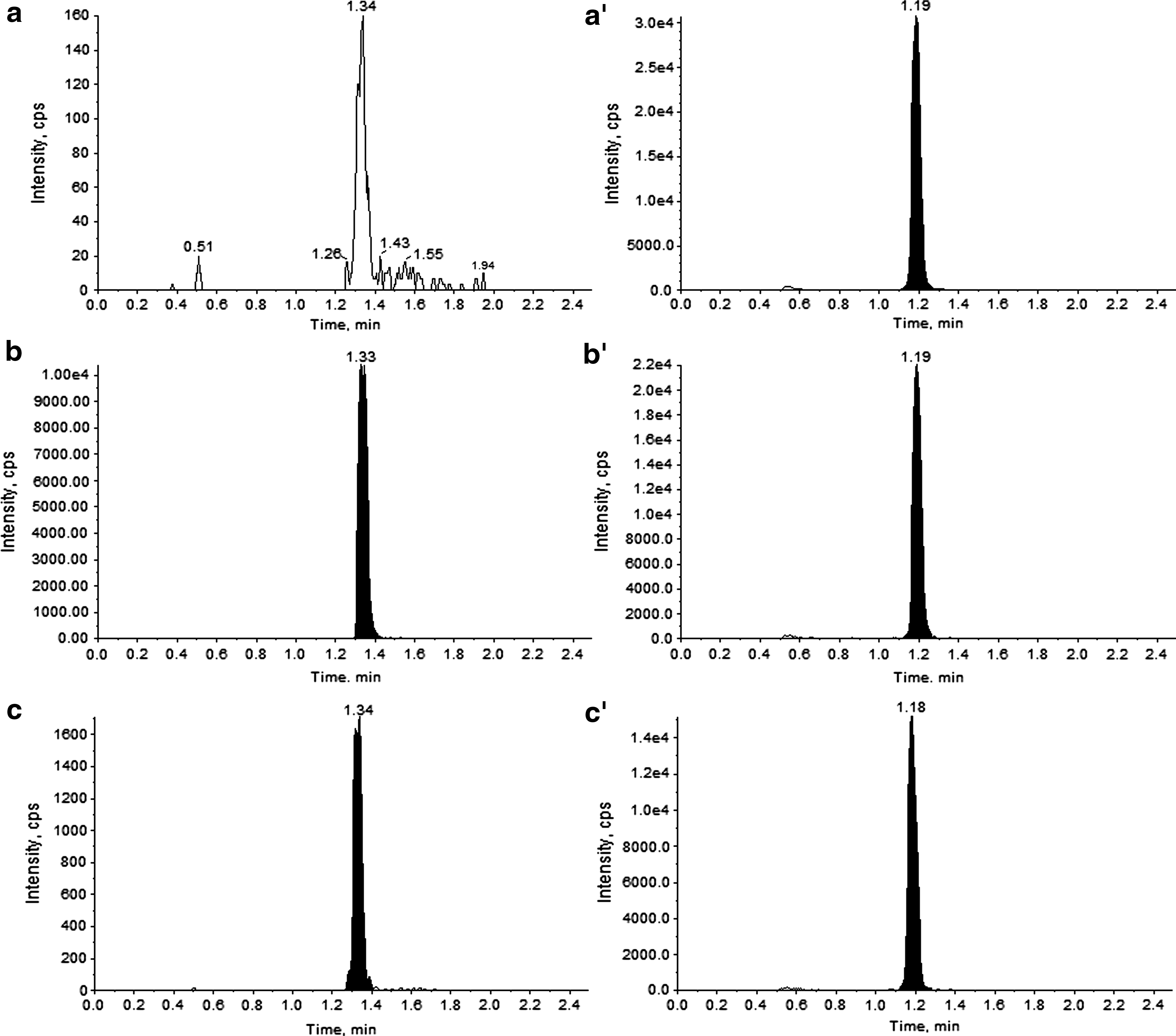
Teicoplanin (A2-2 form) concentrations were 15.1 and 11.0 mg/L for the first and second plasma samples (Fig. 1) and 0.94 mg/L in breast milk. Since our analytical method was initially validated for plasma samples, a blank (breast milk without teicoplanin but containing the internal standard; Fig. 2a, a′) and a quality control spiked with teicoplanin at a concentration of 4.0 mg/L (Fig. 2b, b′) were analyzed before determining the teicoplanin (A2-2 form) concentration in the sample of the mother's breast milk (Fig. 2c, c′). The blank and quality control ruled out any analytical interference.
(a, a′) Blank (breast milk sample without teicoplanin but containing internal standard), (b, b′) quality control with a concentration of 4.0 mg/L (breast milk sample containing teicoplanin and internal standard), (c, c′) patient (mother's breast milk sample with an unknown quantity of teicoplanin and internal standard).
The newborn's ingested dose was calculated using the following formula: \documentclass{aastex}\usepackage{amsbsy}\usepackage{amsfonts}\usepackage{amssymb}\usepackage{bm}\usepackage{mathrsfs}\usepackage{pifont}\usepackage{stmaryrd}\usepackage{textcomp}\usepackage{portland, xspace}\usepackage{amsmath, amsxtra}\usepackage{upgreek}\pagestyle{empty}\DeclareMathSizes{10}{9}{7}{6}\begin{document}
$${ \rm{Infant \ Dose}} = {{ \rm{C}}_{{ \rm{milk}}}} \times {{ \rm{V}}_{{ \rm{milk}}}}$$
\end{document}, where Cmilk is the drug milk concentration and \documentclass{aastex}\usepackage{amsbsy}\usepackage{amsfonts}\usepackage{amssymb}\usepackage{bm}\usepackage{mathrsfs}\usepackage{pifont}\usepackage{stmaryrd}\usepackage{textcomp}\usepackage{portland, xspace}\usepackage{amsmath, amsxtra}\usepackage{upgreek}\pagestyle{empty}\DeclareMathSizes{10}{9}{7}{6}\begin{document}
$${{ \rm{V}}_{{ \rm{milk}}}}$$
\end{document} is the milk volume ingested by the newborn. Because quantifying the volume of ingested milk is challenging, we used the standard assumption of 150 mL/kg/day of breast milk intake. The estimated infant dose was 141 μg/kg/day and was compared with the mother's intravenously administered dose (1,000 mg/day, i.e., 17 mg/kg/day for a bodyweight of 60 kg) using the formula of the relative infant dose \documentclass{aastex}\usepackage{amsbsy}\usepackage{amsfonts}\usepackage{amssymb}\usepackage{bm}\usepackage{mathrsfs}\usepackage{pifont}\usepackage{stmaryrd}\usepackage{textcomp}\usepackage{portland, xspace}\usepackage{amsmath, amsxtra}\usepackage{upgreek}\pagestyle{empty}\DeclareMathSizes{10}{9}{7}{6}\begin{document}
$$\left( { RID = { \frac { Estimated \ Infant \ Dose } { Maternal \ Dose } } } \right)$$
\end{document}. As teicoplanin is also administered intravenously for pediatric infections with a loading followed by a maintenance dose of 30 and 10 mg/kg/day,3 respectively, we applied the RID formula to the pediatric maintenance dose. The RID was 1.4%. Our results show, as suspected by Kaplan et al.,1 that teicoplanin is secreted in small amounts in breast milk and that the estimated infant dose is very low compared with the intravenously administered dose to adults or children. Moreover, teicoplanin is a large molecule with a molar mass ranging from 1,500 to 1,900 Da, so it cannot cross the intestinal wall.1 However, the absolute and relative infant doses could be somewhat greater because first, we only measured the A2-2 form of the drug, and second, we suppose that the teicoplanin secretion in breast milk leads to the same repartition of the different teicoplanin compounds as in plasma.
Teicoplanin targets gram-positive bacteria, including those from the microbiota which is structured during first months of life. Recently, disruptions of the microbiota are implicated in many diseases, such as inflammatory bowel disease, type I diabetes, and obesity.4 Consequently, with this in mind, the main concern is not about pharmacokinetics but rather about the microbiota: what are the medium- and long-term consequences of repeated low quantity of teicoplanin for a few days on the newborn's intestinal microbiota?
Footnotes
Disclosure Statement
No competing financial interests exist.
References
1.
KaplanYC, Keskin-ArslanE, AcarS, et al.Teicoplanin use during breastfeeding. Breastfeed Med, 2017; 12:124.
2.
BernareggiA, BorghiA, BorgonoviM, et al.Teicoplanin metabolism in humans. Antimicrob Agents Chemother, 1992; 36:1744–1749.
3.
WilsonAP. Clinical pharmacokinetics of teicoplanin. Clin Pharmacokinet, 2000; 39:167–183.
4.
SlatteryJ, MacFabeDF, FryeRE. The significance of the enteric microbiome on the development of childhood disease: A review of prebiotic therapies in disorders of childhood. Clin Med Insights Pediatr, 2016; 10:91–107.