
Abstract
Abstract
Background:
Research has shown that women with low socioeconomic status and lack of breastfeeding support often breastfeed for shorter durations. Little research has been done on the effects of a breastfeeding peer support program for women from middle- to high-socioeconomic status.
Objective:
The objective of this project was to determine whether a breastfeeding peer support program would increase breastfeeding duration rates among middle- to high-socioeconomic status women.
Materials and Methods:
One hundred thirteen women were recruited from local OB/GYN offices to participate in a breastfeeding peer support program that included prenatal visits, phone calls, and anticipatory breastfeeding guidance throughout the infants' first year of life.
Results:
Factors associated with a significant increase (p < 0.05) in breastfeeding duration included marital status, mother's ethnicity, mother's medical history, and delivery type. Mothers who remained enrolled in the study had the following breastfeeding duration rates: 85% at 6 months and 65% at 12 months. These are all higher than current national goals and statewide rates.
Conclusion:
Results indicate that consistent breastfeeding support during the infants' first year of life may increase breastfeeding duration rates for women of higher socioeconomic status.
Introduction
B
Many studies have been conducted to determine the reasons for the wide variation in breastfeeding initiation and duration rates worldwide. A mother's socioeconomic status is one of the variables affecting breastfeeding that has been studied most often. Women whose income is at or below the poverty level are less likely to breastfeed than women of higher socioeconomic status. Approximately 59% of women who are below the poverty level breastfeed their infants, whereas almost 80% of women who are >350% of the poverty level breastfeed their infants. According to the 2002 National Immunization Survey, Special Supplemental Nutrition Program for Women, Infants, and Children participation was the factor most strongly associated with decreased breastfeeding initiation and exclusivity rates. 5 There is limited research investigating the effect of middle- to high-socioeconomic status on breastfeeding duration. Skouteris et al. conducted a systematic analysis of interventions designed to promote exclusive breastfeeding in high-income countries. The authors found that barriers to breastfeeding in high-income countries included high obesity rates, returning to work, inadequate family support, embarrassment about breastfeeding in public, and education level. The researchers also commented that “[breastfeeding] support-based programs that extend over a relatively long period and generally take place within the women's homes are effective at increasing exclusive breastfeeding initiation and duration.” 6
The purpose of this project was to determine whether a breastfeeding peer support program would increase breastfeeding duration rates as compared with the current state breastfeeding rates. This project was part of a larger, double-blind controlled clinical trial (Omega Smart Baby Project) that examined the relationship between maternal docosahexaenoic acid intake during pregnancy and lactation and neurocognitive development through the infant's first year of life.
Materials and Methods
This project was approved by Colorado State University's Institutional Review Board. Recruitment occurred at an OB/GYN office, which accepted private insurance. The target population was women with singleton pregnancies, ages 18–42 years, and who were willing to commit to exclusive breastfeeding for the first 6 months of their infants' lives. Participants did not receive compensation for their time in this project; however, they received the breastfeeding support program at no cost.
The breastfeeding peer support program that was used for this project was modeled after the North Carolina Cooperative Extension Service's In-Home Breastfeeding Support Program. Participants were assigned to a breastfeeding support coach. Breastfeeding support coaches were peers of the subjects and had personal breastfeeding experience but were not healthcare professionals and had no prior breastfeeding training. Coaches attended a 2-week training led by a lactation professional before the start of the project and had monthly meetings throughout the study. Topics in the training included History of Breastfeeding, Why Breastfeed?, Barriers to Breastfeeding, Anatomy and Physiology of Breastfeeding, Diet and Lifestyle when Breastfeeding, Initiation and Duration of Breastfeeding, and Anticipatory Breastfeeding Problem-Solving Guidance.
During the project, breastfeeding support coaches also had access to the lactation professional to ask questions and receive support. The breastfeeding peer support program included breastfeeding guidance before birth and throughout the program. Coaches provided in-person visits including a hospital visit, home visit after hospital discharge, and additional home visits at 2, 4, 6, and 10 months, and phone calls at 2 weeks, 1 month, 6 weeks, and 3, 5, 7, 8, 9, 11, and 12 months. Study participants could also contact breastfeeding coaches by cell phone or email at any point as desired. Thorough documentation occurred at each contact point. At the first prenatal visit (intake) and hospital visit, information such as mother's marital status, ethnicity, and medical history was gathered. At subsequent visits, the following information was collected: medication and herbal supplement use, number of children breastfed in the past and for how long, how long planned to breastfeed infant of current pregnancy, sources of support for breastfeeding, type of delivery, length of gestation, medications used during labor and delivery, infant weight and infant medical concerns, and whether mother saw a lactation specialist in the hospital. At each contact after the birth of the baby, the mother was asked whether she was still breastfeeding and, if not, the reason for cessation.
The Statistical Package for the Social Sciences (SPSS) version 21 was used to perform data analyses. Paired samples t-tests and chi-square tests were used to determine significant differences. Descriptive statistics, including measures of distribution, central tendency, and variation, were computed.
Results
One hundred and thirteen mothers participated in the breastfeeding peer support program (Table 1). The majority of participants were white, married, and between the ages of 30–34 years. Twenty-nine percent of participants had a medical history that warranted additional prenatal care from an OB/GYN or primary care provider; three participants received diagnoses of gestational diabetes. Almost half of participants had previous breastfeeding experience. Fifty-five percent of participants planned to breastfeed for 1 year or more. Almost all participants had a support person available to them, and that primary support person was a significant other or other family member. Almost all participants took a prenatal supplement regularly, and >20% took herbal supplements as needed (e.g., ginger for nausea).
Birth experience data were missing for some mothers: ethnicity (n = 112), marital status (n = 111), support person available and type of support person available (n = 92), regular prenatal supplements (n = 108), herbal supplements as needed (n = 109).
Seventy-two percent of participants delivered vaginally and 77% used medications during labor. Seven percent of infants were born prematurely (33–37 weeks); 62% of the infants had no medical problems at birth. Jaundice was the most common medical condition reported. Almost one-fourth of infants received liquids other than breast milk in the hospital (e.g., glucose water and formula) (Table 2). Eighty-four percent of the participants met with a lactation specialist in the hospital.
Birth experience data were missing for some mothers: medications during labor (n = 110), infant medical problems at birth (n = 112), infant given liquid other than breast milk in hospital (n = 97), meeting with lactation specialist in hospital (n = 105).
Factors that were associated with a significant increase (p < 0.05) in breastfeeding duration included marital status (married), mother's ethnicity (white), mother's medical history requiring additional care (none), and delivery type (vaginal). Factors that were not significantly associated with an increase in breastfeeding duration included maternal supplement use, maternal herbal supplement use, number of children conceived, number of children breastfed, labor medication used, infant weight (e.g., low birth weight), infant medical history (e.g., preterm), and lactation consultant visit in hospital. The main reasons provided as to why a participant chose to cease breastfeeding included personal breastfeeding goal reached, perceived low milk supply, work or other scheduling difficulties, physical challenges, health concerns, baby self-weaning, and expecting another child (Fig. 1). A total of eight participants discontinued breastfeeding because of work or scheduling concerns, of this six discontinued before 6 months and two discontinued between 6 and 12 months. Breastfeeding duration rates of program participants exceeded Colorado statewide breastfeeding rates and national Healthy People 2020 goals (Table 3).7,8
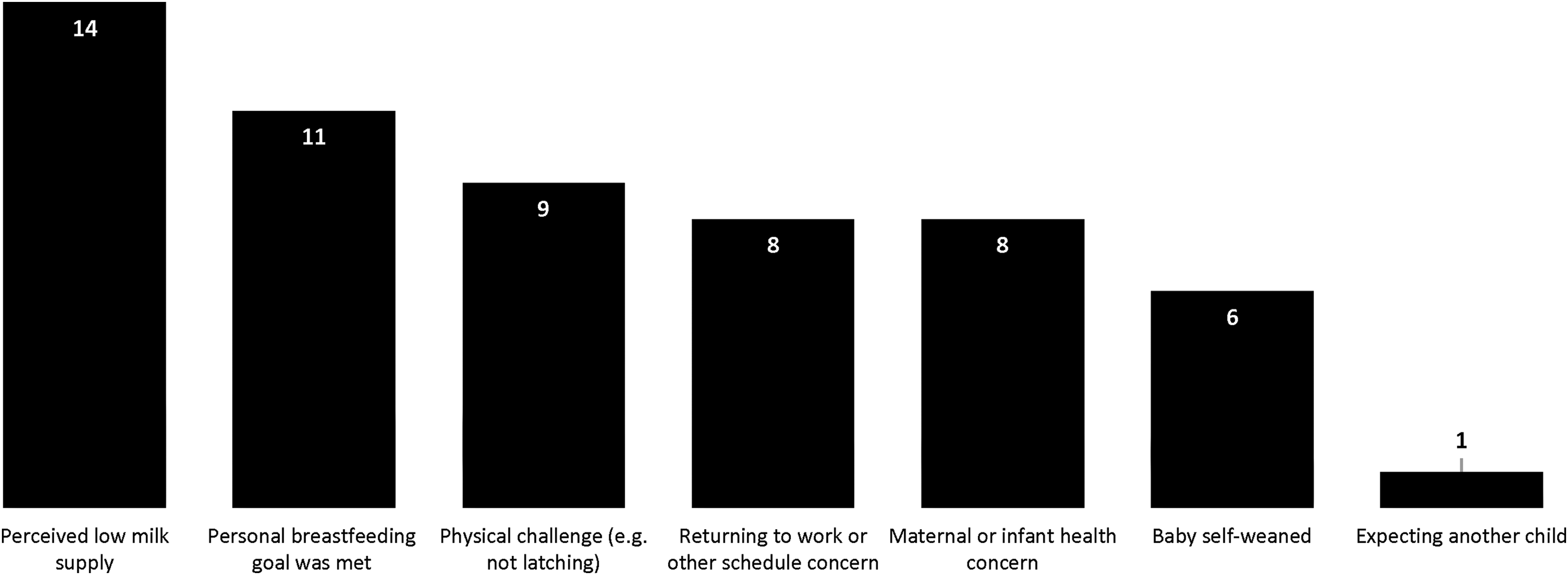
Reasons why participants (n = 46) chose to discontinue breastfeeding.
Contact was lost with 13 participants by month 6 (remaining n = 100).
Contact was lost with an additional one participant by month 12 (remaining n = 99).
Discussion
Results indicate that having consistent breastfeeding support during an infant's first year of life may increase duration rates. Breastfeeding variation among socioeconomic statuses is one of the most thoroughly studied areas of breastfeeding research. Women in the lower socioeconomic statuses have the lowest rates of breastfeeding duration and initiation and also receive the majority of research focus. However, middle- and high-socioeconomic status women are also not meeting the recommendations. Despite this fact, little research has focused on the barriers faced by higher income women. Skouteris et al. reported that obesity, returning to work, inadequate family support, embarrassment about breastfeeding in public, and education level were barriers to women breastfeeding in high-income countries. 6 Returning to work and perceived low milk supply were the top two barriers among this project's participants.
The results of this project show that a breastfeeding peer support program with in-home visits and phone calls supported increased breastfeeding duration rates and attainment of mothers' personal breastfeeding goals. Tahir and Al-Sadat found that telephone lactation counseling increased exclusive breastfeeding rates at 1 month but not at 4 or 6 months. The authors recommended having mothers seek out counseling rather than having the session times directed by the counselor, having mothers meet counselors face-to-face before birth, and having more contact in general. 9 This study design provided many of the components recommended by these authors. Other researchers have found that breastfeeding peer support programs for low-socioeconomic status women were beneficial.10–12 Our data showed similar results for middle- to high-socioeconomic status women who were recruited through an OB/GYN clinic that accepted private insurance.
Limitations of this project include that this was a highly selective population and might not be generalizable to other populations or settings. In addition, education level and weight/height of participants were not gathered for this research project. Since low education level and obesity rates can be barriers to breastfeeding, these data should be collected in future studies. Colorado has one of the highest breastfeeding rates in the country. 8 As a result, there are likely other factors that may have led to the higher levels of breastfeeding. However, participants breastfed at higher rates than Colorado statewide breastfeeding rates at initiation, 6 months, and 12 months. The results of this project may not be generalizable to other states.
Conclusions
This research project demonstrates that women of middle- or high-socioeconomic status benefit from breastfeeding peer support programs. Overall, participant breastfeeding duration goals were met and exceeded both state rates and national breastfeeding goals. Participants within the project experienced barriers to breastfeeding, indicating that it is important for healthcare providers, lactation specialists, policy makers, and community health agencies to understand that, regardless of socioeconomic status, breastfeeding support is critical to maintain and increase breastfeeding initiation and duration rates.
Footnotes
Acknowledgments
The authors would like to thank Janice Gillespie and Annaliese Zeiler, breastfeeding coaches; Nicole Booker, project recruiter; and Jennifer Hunley and Lauren Rhoades, graduate students, for their assistance. Funding for this project was provided by USDA NIFA Grant (No. 00-52102-9633) and Colorado Agricultural Experiment Station Multistate Project (No. 001562410). Medela, Inc. provided the breast pumps for this project.
Disclosure Statement
No competing financial interests exist.