
Abstract
Abstract
The Baby-Friendly Hospital Initiative (BFHI) implemented through the “Ten Steps to Successful Breastfeeding” has been widely promoted as an intervention that improves breastfeeding rates. Step 2 requires the training of all healthcare staff in skills that are necessary to implement the policy. This systematic review provides evidence about the effect of training healthcare staff in hospitals and birth centers on breastfeeding outcomes. Randomized controlled trials (RCT), quasi-RCT, and controlled before and after (CBA) studies comparing training of healthcare staff on breastfeeding and supportive feeding practices with no training were included in this review. We searched CENTRAL PubMed, EMBASE, CINAHL, Web of Science, and the British Nursing Index for studies. Studies were screened against predetermined criteria, and risk of bias of included studies was assessed using the Risk of Bias Assessment tool for Non-Randomized Studies for non-RCT studies and the Cochrane Handbook for Systematic Reviews of Interventions for RCT studies. Of the six studies included in this review, three were RCT whereas three were CBA studies. The studies were conducted in 5 countries and involved 390 healthcare staff. Provision of educational interventions aimed at increasing knowledge and practice of BFHI and support was found to improve health worker's knowledge, attitude, and compliance with the BFHI practices. In one study, the rate of exclusive breastfeeding increased at the intervention site but no differences were found for breastfeeding initiation rates. All included studies had methodological limitations, and study designs and methodologies lacked comparability.
Introduction
S
A systematic review of the effect of BFHI worldwide found that adherence to the Ten Steps positively affected short-, medium-, and long-term breastfeeding outcomes, with the likelihood of improved outcomes, including initiation, exclusivity, and duration, increasing with the number of steps implemented. 4 There have been other studies of the effects of individual steps (including Steps 1, 4, 7, and 9). Step 1 is for facilities to have a written breastfeeding policy and to inform all healthcare staff about it. A systematic review and meta-analysis concluded that hospital interventions can benefit breastfeeding, particularly among first-time mothers. 5 Step 4 is interpreted as placing babies skin-to-skin with mothers immediately after birth and for at least 1 hour. 2 A systematic review and meta-analysis concluded that skin-to-skin contact immediately after birth improved breastfeeding outcomes along with other infant outcomes and had no negative effects. 6 Step 7 states that mothers and infants should “room in,” that is, remain together for 24 hours a day. A systematic review and meta-analysis concluded that there was little evidence to support rooming-in over mother-infant separation in terms of effects on breastfeeding duration. 7 Step 9 states that no artificial teats or pacifiers should be given to breastfeeding infants. A systematic review and meta-analysis of randomized, controlled trials involving pacifier use and breastfeeding outcomes concluded that pacifier use after birth or after lactation was established among healthy, term breastfeeding infants did not affect exclusive and partial breastfeeding up to 4 months. 8 All the recent reviews concluded that further studies were needed.
Step 2 is: “Train all healthcare staff in skills necessary to implement this policy,” 2 referring to the written breastfeeding policy of the facility providing maternity services and infant care, as noted in Step 1. The WHO concluded that the BFHI experience confirms that 18 hours can be considered an appropriate minimum length for the training, although longer courses (e.g., 6 full days) with daily clinical components would be desirable. 9 The WHO also stated that the training should be compulsory and combined with strong and specific facility policies to change facility practices. 9 A systematic review of the effect of education for health professionals and breastfeeding counselors concluded that the BFHI training course could influence breastfeeding duration. 10 However, there were methodological challenges to comparing interventions that train health staff due to differences in settings and contexts. 10
This study is an updated systematic review and synthesis of findings to inform the evidence base for Step 2. The purpose of this study is to provide evidence about the effect of training healthcare staff in hospitals and birth centers on breastfeeding outcomes.
Methods
The study was performed according to the protocol registered in the International Prospective Register of Systematic Reviews (PROSPERO 2016:CRD42016042035) and Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines 11 (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/bfm).
Search strategy
We performed an electronic search of the Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, EMBASE, CINAHL, Web of Science, and the British Nursing Index. Conference proceedings were also considered. The searches were a combination of four main themes: breastfeeding policy, breastfeeding support, health facility staff training, and breastfeeding outcomes. Particularly, we focused on knowledge and attitude on infant feeding, practice of the other steps to successful breastfeeding, adhering to the provisions of the International Code of Marketing of Breast-milk Substitutes, and breastfeeding outcomes.
Consistency in the theme was applied by taking into account the terminological and technical differences between the databases. Various synonyms and related terms for all subjects were used. No restrictions were applied to the searches in terms of publication year, language, country, or region. All six databases were searched from inception. The full search strategy is presented in Supplementary Table S2.
Types of studies
All randomized and quasi-randomized controlled trials (RCT) comparing training of healthcare staff on breastfeeding and supportive feeding practices with no training were included. Controlled before and after (CBA) studies were also included. Observational studies including cohort studies, cross-sectional, and case-control studies were excluded. The study PICO criteria are shown in Supplementary Table S3.
Participants
Included participants were healthcare professionals working within the health facility. We excluded studies where intervention targeted healthcare professionals who only worked at community level, traditional birth attendants, or other breastfeeding support groups.
Interventions
Studies were included if the intervention included provision of any training on breastfeeding and supportive feeding practices to healthcare facility staff.
Outcomes
The primary outcome measures were early initiation of breastfeeding, exclusive breastfeeding during the stay in the facility, and knowledge on infant feeding. Secondary outcomes were quality of skills of health facility staff in improving practices of mothers in optimal infant feeding, attitudes on infant feeding, adherence to the provisions of the International Code of Marketing of Breast-milk Substitutes, and duration of exclusive breastfeeding (months).
Study selection
First, O.B. and M.S. independently assessed all titles and abstracts. Second, we retrieved full text articles of studies potentially identified for inclusion from the title and abstract screening. O.B. and M.S. screened full texts and noted the reason for excluding studies. We resolved disagreements through discussion and, when required, consulted a third person. We created a study flow diagram to map out the number of records identified, included, and excluded (Fig. 1).
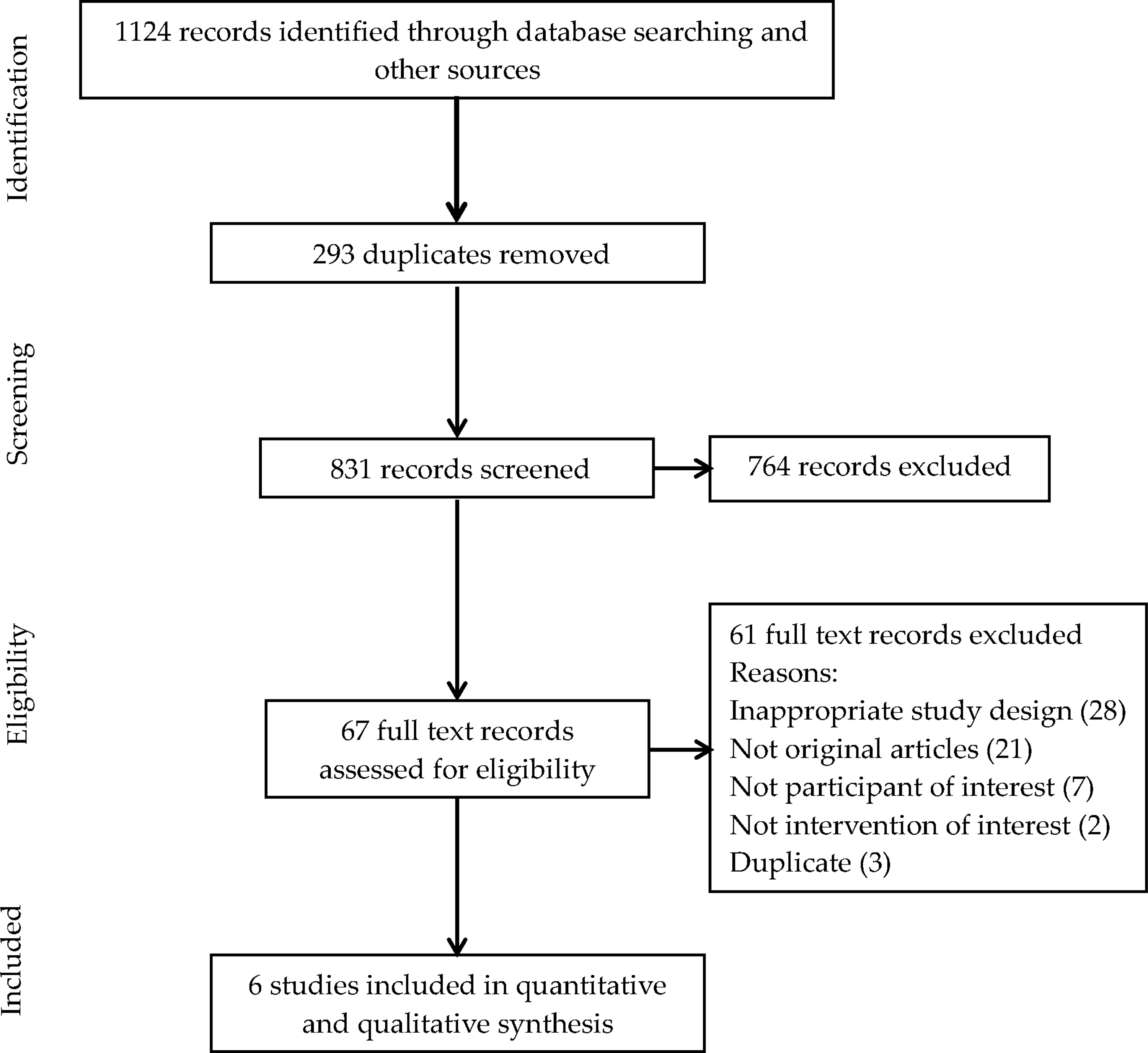
Flowchart showing identification of studies.
Data extraction and management
We independently (A.D., J.Y., and Y.T.) extracted data from the selected studies by using a predesigned and pilot tested data extraction form. Discrepancies were resolved through discussion. Information extracted from each study included (1) study characteristics (design, location, setting, trial period, and sample size of intervention and control), (2) characteristics of study participants (inclusion and exclusion criteria), (3) duration of intervention, and (4) outcome measure. We entered all data into the Review Manager Software 12 and checked for accuracy. When information regarding any of what has been just mentioned was unclear, we attempted to contact authors of the original reports to provide further details.
Assessment of risk of bias in included studies
A.D., J.Y., and Y.T. independently assessed the risk of bias for each included study. For RCTs, we assessed risk of bias by using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions 13 ; whereas for non-RCT studies, we used the Risk of Bias Assessment Tool for Non-randomized Studies (RoBANS) 14 . We resolved any disagreement through discussion with E.O. and O.B. For each domain, we assessed the methods as low risk, high risk, or unclear risk of bias.
Measures of treatment effect
For dichotomous data, we planned to present results as summary risk ratios or odds ratios with 95% confidence intervals. In case of continuous data, we planned to use the mean difference if outcomes were measured in the same way between trials or standardized mean difference to combine trials that measured the same outcome, but used different tools of assessment.
This review included studies using different study designs (RCTs and CBA studies). We had planned to analyze relevant data from both study designs separately. However, we were unable to meta-analyze any data in this review due to methodological variation in the CBA studies and unavailability of data for outcomes of interest in the cluster RCTs. We had also planned to conduct subgroup analyses based on length of training, frequency of training, amount of time spent on practical session, method of training, and type of trainer. However, no subgroup analysis was conducted due to the limited number of included studies.
Results
Results are presented in the following sections based on study design, as quantitative summary and textual narrative analysis. Key findings and conclusions of individual studies are summarized in Tables 1 and 2.
BFHI, Baby-Friendly Hospital Initiative; MD, mean difference; SLC, Santos Lactation Center.
EBF, exclusive breastfeeding; N/A, not available.
Search results
A total of 1,124 records were identified through the searches. After duplicates were removed, 831 remained for title and abstract screening. Of these, 67 full text articles were reviewed; 61 of those were excluded due to inappropriate design, lack of population or intervention of interest, or absence of data (Supplementary Table S4). Six studies were included in the data synthesis of health facility staff training on breastfeeding and supporting feeding practices for improving breastfeeding outcomes (Fig. 1).
Study characteristics
Six studies15–20 involving 390 health professionals were included in the review. For Westphal et al., 19 only the number of participants from the intervention group was reported. Three hundred and seventeen participants (81%) from all included studies were nursing staff, whereas only one study 19 included both nurses and physicians. Breastfeeding training material and duration varied across the studies. In Ekstrom et al., 16 a process-oriented training program was implemented; whereas Westphal et al. 19 conducted a 24-hour training program on breastfeeding promotion for health providers modeled on the BFHI held over 18 days at the Santos Lactation Center (SLC). The intervention in Downie et al. 15 involved 12 two-hour sessions described as the Lactation Adviser Program designed to increase nurses' and midwives' knowledge, attitude, and confidence toward lactation management. The effectiveness of a breastfeeding education intervention consisting of a 1.5-hour mandated session with an optional self-paced tutorial was also evaluated 17 ; whereas Weddig 18 implemented an online course with an 8-hour, in-person practicum. Only one study 20 assessed the effectiveness of the WHO/UNICEF breastfeeding course.
Effects of interventions
All six studies were from different countries—four from high-income countries (Sweden, Australia, Canada, and the United States) and two were from Brazil—an upper middle-income country. Three of the included studies were RCTs—two being cluster RCTs,16,19 whereas the remaining three were CBA studies.15,17,18 None of the studies used a validated scale for assessing outcomes. Also, each of the included studies employed a different questionnaire or method for outcome assessment, thus precluding the possibility of combining the summary estimates from individual studies in a meta-analysis. We, therefore, present a narrative summary of the results categorized according to the study design.
Randomized controlled trials
One individually randomized 20 and two cluster RCTs conducted in Sweden 16 and Brazil 19 assessed the effect of breastfeeding training on knowledge skills, institutional changes, and attitudes of health facility staff to breastfeeding. The individually randomized study conducted in Brazil involving 60 health workers from different units assessed breastfeeding knowledge and skills pre-and post-intervention. 20 The training course was found to increase health workers' knowledge and clinical counseling skills for the support of breastfeeding. In another Brazilian study (12 healthcare providers), institutions exposed to the SLC course had a higher ranking in a 10-step score test than those in the control group 19 6 months after the intervention. In Sweden, attitude toward breastfeeding among 81 antenatal midwives and postnatal nurses exposed to a process-oriented breastfeeding training was evaluated in four dimensions: regulating, facilitating, disempowering, and breastfeeding-antipathy attitudes. The intervention group decreased their scores on the regulating scale and increased their scores on the facilitating scale over the first year after training, making both antenatal midwives and postnatal nurses better disposed to breastfeeding. Particularly, postnatal nurses in the intervention group were found to become less regulating, less disempowering, and more facilitating over time after the intervention.
CBA studies
Providing educational interventions aimed at increasing knowledge and practice of BFHI and support among healthcare professionals, breastfeeding was found to increase nursing staffs' knowledge on breastfeeding. Nurses exposed to breastfeeding education had a significantly higher knowledge and attitude score than the control group 6 months after the intervention. 15 In a small rural Canadian hospital serving a predominantly native American population, nurses exposed to a 1.5-hour breastfeeding training with optional tutorial showed a significant increase in breastfeeding belief scores 7 months after the intervention, compared with nurses at the control site. In the same study, although there were no changes in bottle feeding beliefs or breastfeeding attitude scores, nurses who completed the tutorial had significantly higher breastfeeding attitude scores from pre- to post-test (45.2 versus 48.0, p = 0.003). 17 In another study done in the United States, registered nurses who took an online breastfeeding course with an 8-hour practicum demonstrated an increase in knowledge, changes in behavior related to breastfeeding initiation best practices, and appropriate use of formula supplementation. 18 Provision of breastfeeding education to healthcare staff significantly increased compliance with BFHI criteria at intervention sites especially for Steps 1, 5, 6, 9, and 10 of the Ten Steps. Also, hospital chart audit indicated an increase in exclusive breastfeeding rates at the intervention site but no differences were found in breastfeeding initiation rates or frequency of breastfeeds. 17
Risk of bias in included studies
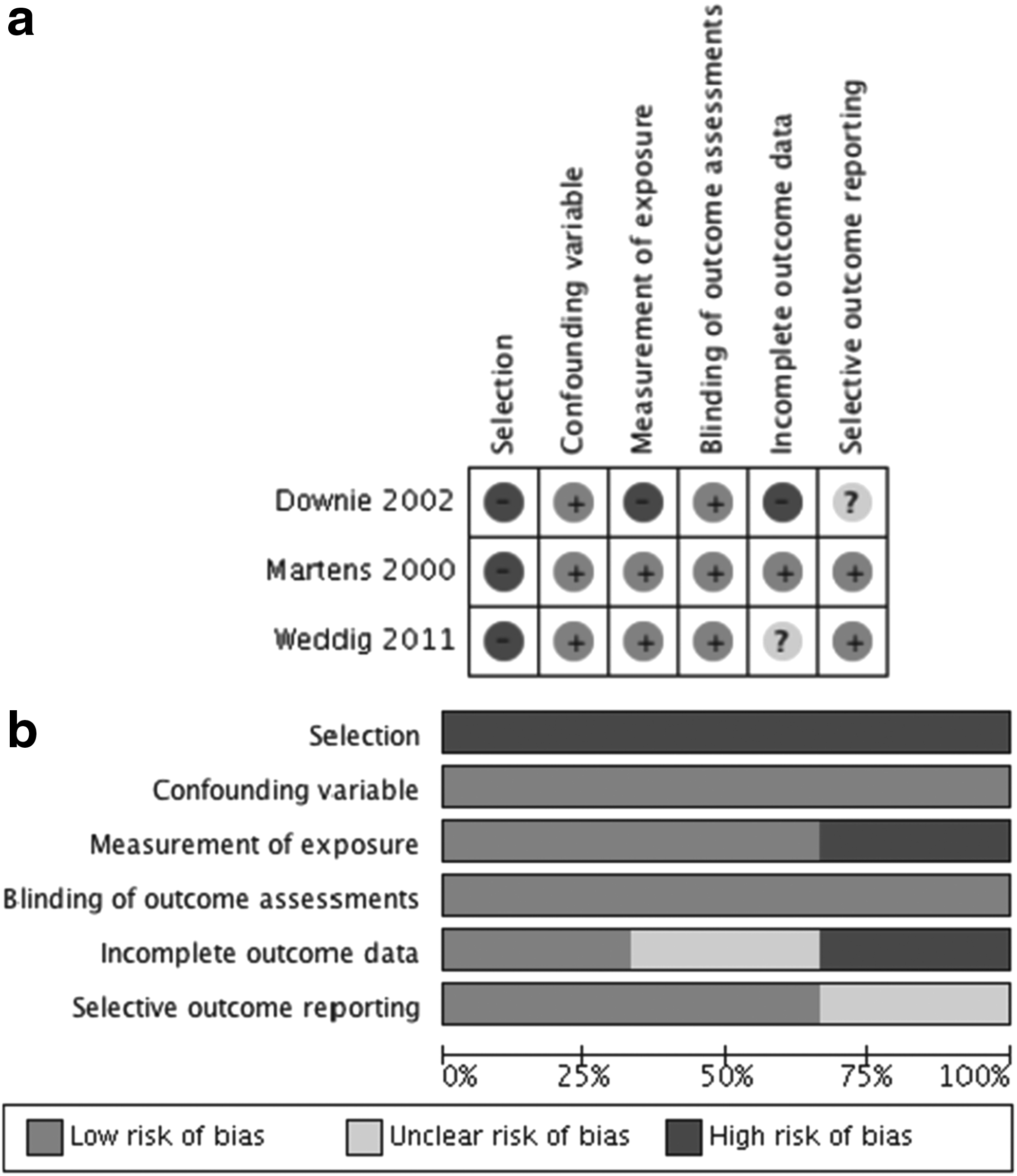
Overall, the included studies were of moderate to low quality (see Figs. 2 and 3). All studies had problems with various aspects of study quality.

Review authors' judgments about each risk of bias item
Review authors' judgments about each risk of bias item
Risk of bias for RCTs
In terms of methods used for random sequence generation, Ekstrom et al. 16 was assessed as having low risk of bias, whereas the randomization process was unclear for Rea et al. 20 and Westphal et al. 19 In all three studies, methods for allocating participants to comparisons were not described and were assessed as having unclear allocation concealment. All included RCTs included in this review lacked blinding of participants and personnel and were assessed as having high risk of bias. Performance blinding for this type of intervention is problematic as the healthcare staff receiving the interventions and the staff delivering them are likely to have been aware of group allocation. In the case of detection bias, outcome assessment was based on self-reports by using structured interviews in one study 16 ; whereas in another, 19 facilitator-led interviews and focus group discussions were held. Both trials were assessed as having low risk of bias due to the use of standardized data collection methods. One trial 16 had loss to follow-up of more than 20% and was assessed as having high risk of attrition bias. Although we did not have access to either trial registration or the study protocol, two RCTs were assessed as having low risk for reporting bias as they appear to have reported outcomes as described in the text.
Risk of bias in CBA studies
All three studies15,17,18 were assessed as having high risk of selection bias. In all three studies, comparison groups came from a different health service system. Participants included in one study 18 were also reported to have participated more, in breastfeeding education other than the intervention, thus increasing their level of interest in supporting lactation. Regardless of the inadequate selection of participants, all three studies were judged to have low risk of bias for confounding as the studies used statistical methods that controlled for major confounding factors in the analyses. Performance bias due to inadequate measurement of intervention was assessed as high risk in one study 15 due to data obtained through self-reports, whereas two studies17,18 had low risk of bias. Detection bias caused by inadequate blinding of outcome assessment was low in all three studies. Attrition bias was high in one study 15 due to large differences with respect to the number of participants that completed the post-test. In another study 17 with low risk of attrition bias, missing data were accounted for and a test showed no differences between pre- and post-completion rate. One study 18 had an unclear risk of bias due to lack of information regarding participants in the original sample that completed the post-test. Reporting bias was assessed to be unclear in one study 15 due to inadequate description of outcomes a priori, whereas two studies were judged to have low risk of bias.
Discussion
This review for health facility staff training on breastfeeding and supporting feeding practices aimed at providing evidence on the effect of training healthcare staff in hospitals and birth centers on breastfeeding outcomes. The six studies in this review included one individual and two cluster RCTs, and three CBA studies. Even though our review planned to assess a wide range of outcomes associated with healthcare staff training, most of the included studies reported on either of two outcomes: breastfeeding knowledge and attitude. Few included studies assessed other outcomes such as BFHI compliance—two studies17,19; exclusive breastfeeding rate—one study. 17
Five out of the six included studies reported breastfeeding knowledge and attitude. However, each study had assessed the outcomes by using a different scale, thus preventing the possibility of conducting meta-analysis. Included studies either did not assess the same set of outcomes or assessed the same outcome by using different methodologies or scales. Among the CBA studies, both Weddig 18 and Martens 17 assessed breastfeeding knowledge and attitude by using different scales—the Coventry University Breastfeeding Assessment Tool and the Breastfeeding and Bottle Feeding Beliefs Tool. In other cases, an inadequate description of study methodology limited our ability to combine results from individual studies. For example, there were no details about the questions used in the self-administered questionnaire in one study 15 to assess comparability to another study 17 reporting the same outcome.
The variation in the method of outcome assessment among studies may also be due to differences in the training provided to health facility staff. Breastfeeding training material and duration varied across all of the included studies, and only in one study 20 was staff training based on the WHO/UNICEF breastfeeding counseling course. The lack of comparability across studies with regards to training material and outcomes severely limited the possibility for quantitative analysis. Such variations in outcomes reported on a particular topic undermine consistency in the synthesis of evidence, 21 thus making it difficult to draw clinically relevant and policy-oriented conclusions. Therefore, core outcomes in breastfeeding research are required.
More than 80% of participants in the six studies included only nursing staff, with only one study 19 including both nurses and physicians. This finding is of significance and may reflect the overall conclusions regarding the rate of compliance to the Ten Steps, as Step 2 requires training all healthcare staff in skills that are necessary to implement the breastfeeding policy. Although physicians have a unique role in providing breastfeeding support, many physicians are not adequately trained in breastfeeding medicine. 22 In addition, practicing physicians may find it difficult to stay abreast of best breastfeeding support practices.22,23 Physicians play an important role in mothers' breastfeeding decisions,24,25 and breastfeeding support from physicians is a modifiable barrier to improved breastfeeding outcomes. Therefore, future research should aim at determining the perception and attitude of physicians toward breastfeeding, and it should seek ways to improve breastfeeding training among physicians.
In this review, expectedly, we found evidence to support the association between health facility staff training and improved knowledge and attitude toward breastfeeding among maternity staff. However, only one of the included studies reported on breastfeeding outcomes. 17 The WHO's “Ten Steps to Successful Breastfeeding” are important guidelines that outline the most fundamental needs for successful breastfeeding, and they address how hospital staff can optimize breastfeeding success. Further, evidence from observational studies and RCTs show an association between each of the steps and a positive breastfeeding outcome. 9 Our review focused on Step 2 of the Ten Steps. Step 2 requires maternity staff training for at least 18 hours plus 3 hours of supervised clinical experience, recommended at all levels to address the Ten Steps, breastfeeding, counseling, and the International Code of Marketing of Breast-milk Substitutes. However, the scarcity of studies demonstrating the impact of Step 2 on actual breastfeeding outcomes raises the question as to the relevance of provider training in the Ten Steps. Therefore, further research regarding the inclusion of Step 2 in the Ten Steps is needed wherein a core set of breastfeeding outcomes are measured.
The focus of our review is to inform evidence for updating breastfeeding policy and practice globally, and it is thus focused on interventions provided to facility-based healthcare workers only. To ensure relevance across different settings in both developed and developing countries, we included a wider search period with no restrictions on location or setting—unlike past reviews on this topic. 10
Although this review focused entirely on Step 2 of the BFHI's Ten Steps, intervention effects for this step and other steps may be more effective when administered in concert with other interventions included in the BFHI's Ten Steps. Findings from experimental studies evaluating the impact of other individual steps in the BFHI's Ten Steps for improving breastfeeding outcomes have been inconclusive. A Cochrane review that assessed the effectiveness of antenatal breastfeeding education on breastfeeding initiation and duration found no conclusive evidence that antenatal breastfeeding education of any sort could improve the initiation or duration of breastfeeding; or the proportion of women with any breastfeeding and exclusive breastfeeding at 3 or 6 months over the standard care. 26 Similarly, Jaafar et al. 7 found insufficient evidence to support the practice of rooming-in versus mother-infant separation. In yet another Cochrane review, Collins et al. 27 found limited evidence to show that avoidance of bottle feeds during establishment of breastfeeding was effective to increase the extent and duration of breast feeding in preterm infants. 27
In spite of the limited evidence on the effectiveness of Step 2 and other individual steps for improving breastfeeding practice and outcomes, there is more evidence to support the BFHI as an intervention to increase breastfeeding than there are studies that demonstrate no effect of the intervention. Two separate reviews that examined the impact of the BFHI package on breastfeeding outcomes provide global evidence showing that adherence to the BFHI's Ten Steps has a positive impact on breastfeeding outcomes across geographies.4,28 In another review of education and evidence-based practice interventions with health professionals and breastfeeding counselors on breastfeeding duration, Spiby et al. 10 found insufficient evidence on the overall benefit or harm of the interventions assessed, but they suggested the potential of the UNICEF/WHO BFHI training for improving breastfeeding duration.
The studies included in the current review were judged to be of moderate to low quality, providing low-quality evidence due to study design and methodological limitations. In addition, there was considerable heterogeneity in definitions, methods of analysis, and outcomes across studies. A wide variety of educational interventions for health facility workers that differed in type and duration of training were identified that aimed at increasing knowledge and support for breastfeeding. In one trial, 20 the WHO/UNICEF 40-hour breastfeeding counseling course was provided to health workers; whereas all other studies provided training based on training materials either previously in use or developed specifically for the intervention. There was a general lack of a unifying model across the studies, and detailed contents of the interventions were unavailable to enable comparison across studies. Similar observations were also reported in other reviews of education for health professionals and breastfeeding counselors on duration of breastfeeding.10,28
In view of compelling evidence showing the many benefits of breastfeeding for both infant and women, UNICEF/WHO launched the BFHI as a quality improvement program to protect, promote, and support breastfeeding, by putting into practice the “Ten Steps to Successful Breastfeeding.” Training in breastfeeding and lactation management, thus, became a requirement for various types of maternity healthcare staff. However, it is important to consider the context of research undertaken on this topic. Although RCTs would provide the strongest evidence base for intervention effects, randomization of healthcare staff between breastfeeding training and no training would contradict the basic requirement of the BFHI practices. As a result, few RCTs could be found on this topic. Thus, we deemed it appropriate to include CBA studies in our review.
Our review has several limitations. The variation in the study methods and the types of study designs used in the included studies precluded the possibility of conducting meta-analyses. A meta-analysis involving well-designed studies would provide more robust evidence on the impact of healthcare staff training on breastfeeding outcomes. In spite of this shortcoming, valuable information could still be derived from included studies. Future reviews in this area may also follow the realist review approach 29 as such review methods will provide an understanding into problems regarding implementation and compliance with the BFHI guidelines at the facility and country level. Our review also included studies in which a wide variety of staff training materials was used. The variation in training materials may suggest difficulties associated with the adoption of a universal breastfeeding training curriculum. However, our review has been unable to provide insights regarding challenges faced by health facilities when implementing such BFHI-required staff training. An attempt was made to identify all research articles involving healthcare staff training, but our review may have missed important contributions by including only studies involving facility-based healthcare staff. We did not include studies involving nonhealth facility-based healthcare staff because this review was conceptualized to inform policy and practice as it relates to implementation of Step 2 at facility level. These limitations notwithstanding, our review provides important information regarding the effectiveness of Step 2 with implications for breastfeeding policy, and it identifies the limitations of the existing evidence base.
Conclusion
Adherence to Step 2 of the Ten Steps that form the basis of BFHI had a positive impact on the attitude of healthcare staff and improved their knowledge of recommendations for infant feeding in some settings. Health facility staff training on breastfeeding and supportive practices may help to improve the compliance with the BFHI. It is important to develop core outcomes in breastfeeding research to provide a more robust evidence base for Step 2 and other steps of the BFHI.
Footnotes
Acknowledgments
The authors would like to thank Miwako Segawa, Yuko Serizawa, and Chi Kataoka (NCCHD) for their help in developing the search strategy and conducting the electronic search. This review was partially developed during the World Health Organization (WHO)/Cochrane/Cornell University Summer Institute on Systematic Reviews in Nutrition for Global Policy Making hosted by the Division of Nutritional Sciences, Cornell University, Ithaca, NY, July 25–August 5, 2016. Source of funding: This research was supported (partially) by the Grant of National Center for Child Health and Development 27B-10, Japan, Japan Agency for Medical Research and Development, Japan and Department of Nutrition for Health and Development, WHO (Switzerland). The WHO acknowledges the Bill and Melinda Gates Foundation for supporting this work.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.