
Abstract
Abstract
Background:
Tongue tie or ankyloglossia articles are recorded in the Medline since 1949.
Objective:
To study trends in yearly number of tongue tie or ankyloglossia publications.
Methods:
Medline search engine was used to determine the yearly number of published consensus statements from 1949 to 2016. Keywords of tongue tie OR ankyloglossia OR frenotomy OR frenulotomy were used for the search. Articles were classified as case reports (or series), reviews, editorials (or opinions), cohort studies, clinical trials (nonrandomized), randomized controlled trials (RCT), and systematic reviews (SR). Linear or polynomial regression was used to determine trends. We also systematically summarized all RCTs published to date.
Results:
The total number of yearly published articles increased in a cubic fashion (r2 = 82.6%, p < 0.0001) over time (0–7 per year from 1949 to 1989, and up to 27–44 in the last 5 years). In terms of strength of evidence hierarchy, most articles belonged to low hierarchy categories (case reports 37.9%, reviews 15.4%, and editorials/opinions 13.4%), with only 8 RCTs and 10 SRs (all of them published during the last 10 years of the study period).
Conclusion:
The yearly number of tongue tie or ankyloglossia-related articles has increased dramatically in past few years. Most articles bring little evidence, but the past few years have witnessed publication of few RCTs and SRs. If this trend continues, much more solid evidence should accumulate about diagnosis and management of tongue tie, as it relates to breastfeeding and other outcomes.
Introduction
T
Materials and Methods
To perform this systematic study we used all Medline articles registered from January 1, 1948 and until December 31, 2016. We stopped the bibliographic study by the end of 2016, at the time the study was conducted (January 2017). Search terms (keywords) of tongue tie or ankyloglossia or frenotomy or frenulotomy were used for the search. The full text of all articles were retrieved, and each article was classified by two reviewers (ABN and FBM) as case reports (or series), reviews, editorials (or opinions), cohort studies, clinical trials ([CT], nonrandomized) randomized controlled trials (RCT), basic (or animal) studies, and systematic reviews (SR). We did not include any language limitation. Contrary to Medline's own classification of articles, we did not list RCTs as CTs. Also, articles based on a case report and a review of the literature were only listed as case reports. Thus, each article appears only once in our classification. We also examined the reference list of all retrieved articles to identify additional articles that the electronic search may have missed.
The Minitab version 16.0 (State College, PA) was used for statistical analyses. We used linear and polynomial regression to determine the effect of advancing year of publication upon the number of publications of each type. A p-value of <0.05 was considered significant.
Results
There were 514 articles retrieved by the search. The total number of yearly published articles increased in a cubic fashion (r2 = 82.6%, p < 0.0001) over time (0–7 per year from 1949 to 1989, and up to 27–53 in the last 4 years (Figure 1). Articles published in 2016 may not be completely recorded by Med-line. Case reports constituted 37.9% of the published articles, while 15.4% were reviews, 13.4% were editorials or opinions, 16.3% were cohort studies, 7.7% were basic or animal studies. Only 20 CTs (nonrandomized), 8 RCTs, and 10 SRs could be retrieved, all of them were published during the last 10 years of the study period.
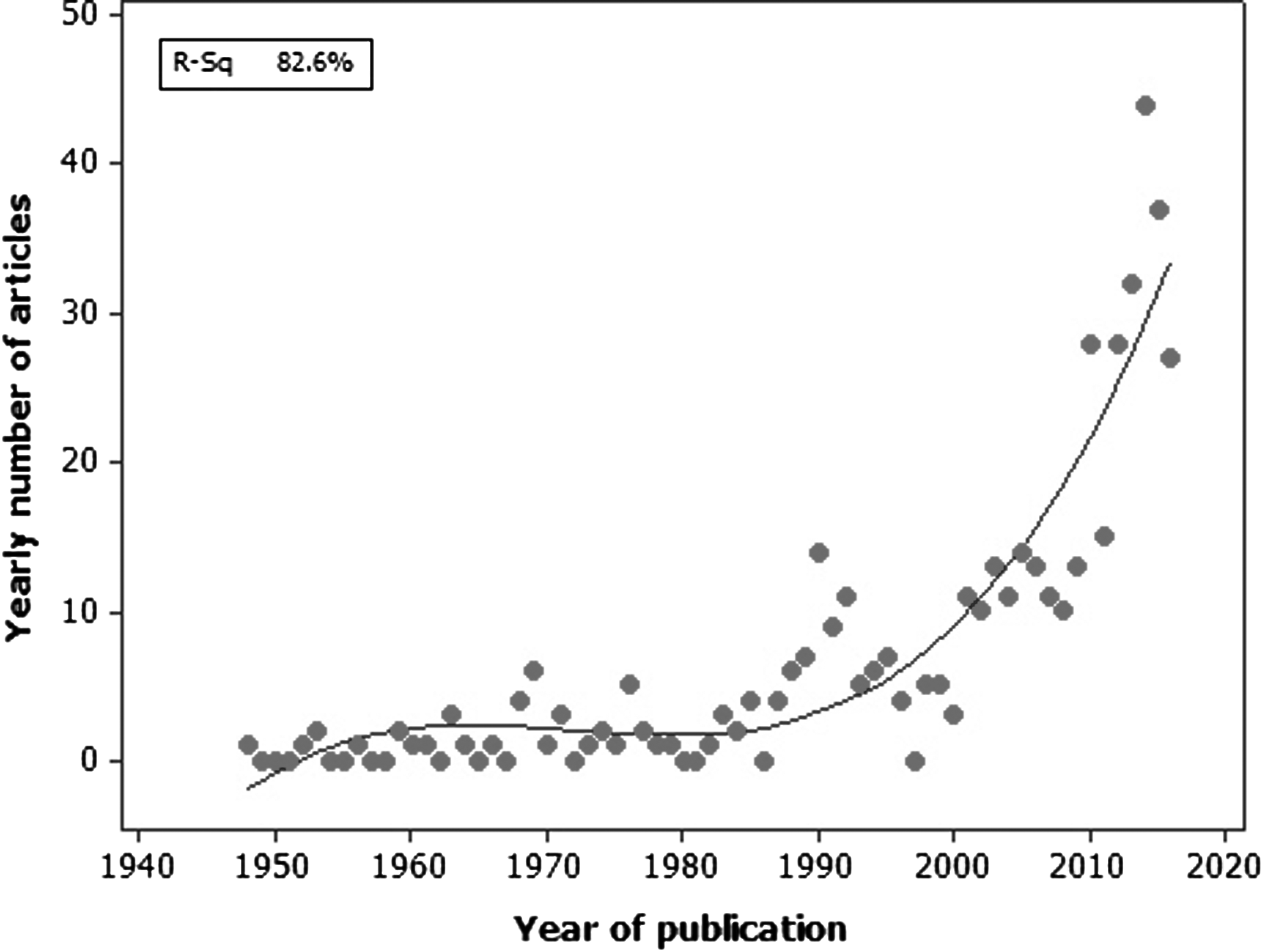
Yearly number of tongue tie-related articles (Y-axis) versus year of publication (X-axis).
Thus, up to January 1, 2017, there were only 8 RCTs that studied various outcomes and they were very heterogeneous in their inclusion criteria. Their main findings are as follows (Table 1):
NFCS, neonatal facial coding system.
The first one, by Hogan et al., 5 published in 2005 included 57 infants with a tongue tie of any grade with breastfeeding difficulties, which were randomized to either immediate frenotomy or frenotomy delayed by 48 hours. The study was not blinded both in terms of assessment by investigators and mothers were fully aware of the timing of the procedure. The authors of this article concluded that division of the tongue ties resulted in improved feeding in 54 out of 57 infants. The improvement was self-reported by the mothers. Importantly, only 40 out of 57 infants were breastfed, and 17 infants were bottle fed. Duration of breastfeeding was not assessed since the follow-up period was of 4 weeks only.
The second study, by Dollberg et al., 1 published in 2006 included 25 infants aged 1–21 days, with tongue tie of infants with reported breastfeeding difficulties, which were randomized to either immediate frenotomy followed by sham procedure or sham procedure followed by frenotomy. The study was blinded both in terms of assessment by investigators: both LATCH and pain scores were calculated and recorded by investigators unaware of whether the infant was after frenotomy or after sham procedure. Mothers were also blinded. The authors of this article concluded that division of the tongue ties resulted in a significant decrease in maternally self-reported pain score compared to sham (p = 0.001) and a nearly significant improvement in latch (p = 0.06).
The third study, by Buryk et al., 6 published in 2011 included 58 infants aged 0–30 days old (mean age 6 days), with breastfeeding difficulties and significant ankyloglossia, according to the Hazelbaker Assessment Tool for Lingual Frenulum Function (HATLFF). Infants were randomized to either immediate frenotomy or sham procedure. The study was blinded both in terms of assessment by mothers (both nipple pain score by the Short-Form McGill Pain Questionnaire and the Infant Breastfeeding Assessment Tool), and in terms of assessment by the ENT surgeon and lactation consultants who performed HATLFF scores. The authors concluded that division of the tongue ties compared to sham resulted in a significant decrease in maternally self-reported pain score (p = 0.001) and a nearly significant improvement in LATCH score (p = 0.06).
The fourth study, by Berry et al., 7 published in 2012 included 60 infants less than 4 months old (mean 32 days old) with tongue tie of any grade with breastfeeding difficulties, that were randomized to either immediate frenotomy or sham procedure. The study was partially blinded for the mothers, who recorded a pain numeric score and the observer, who recorded LATCH scores and the Infant Breastfeeding Assessment Tool. After the first feeding post procedure, mothers were informed of procedure allocation, and infants who had the sham procedure underwent frenotomy. Mothers, who at this point were no longer blinded, recorded the pain score again. The authors concluded that division of the tongue ties resulted in improved feeding in 78% of the infants, compared to 47% in the infants in the sham procedure group. The improvement persisted a day after the procedure in 90% and after 3 months (mothers were not blinded at that time). Of note, only 51% of the infants were still breastfeeding at 3 months of age, although all underwent frenotomy.
The fifth study, by Emond et al., 8 published in 2014 was the largest and included 107 infants less than 2 weeks old, median 11 days, with more stringent inclusion criteria: HATLFF score of 6–12 (mild–moderate tongue tie) and LATCH score of ≤8. The infants were randomized to either immediate frenotomy or standard postnatal care. The researchers who performed LATCH score 5 days after the procedure, were blinded to infant group assignment. In contrast, mothers, who reported the maternal breastfeeding self-efficacy score, were not blinded. These authors reported that frenotomy did not improve LATCH scores. It, however, improved the tongue ie and increased maternally reported (nonblinded) breastfeeding self-efficacy: at 5 days, there was a 15.5% increase in bottle feeding in the comparison group compared with a 7.5% increase in the intervention group. After the 5-day assessment, 44 patients (out of 52) in the comparison group requested a frenotomy, which was performed; subsequently, by 8 weeks only six infants (12%) were breastfeeding without a frenotomy and two patients were lost from follow-up. At that time, there were no differences between groups in breastfeeding outcome measures or in infant weight, but at this stage the majority of the comparison group had undergone frenotomy.
The sixth study, by Ovental et al., 9 was published in 2014 and included 21 infants recruited during the first 3 days of life. This study examined the analgesic effect of topical application of benzocaine before lingual frenotomy in infants with symptomatic tongue tie, as judged by maternal complaints and recommendations of both a lactation consultant and a neonatologist, using the Coryllos classification. The investigators reported that crying time was less than 1 minute in all subjects and that average crying time in the benzocaine group (21.6 ± 13.6 second) was counter-intuitively longer than that in the control group (13.1 ± 4.0 second) (p = 0.103). They concluded that benzocaine frenotomy is not recommended in infants who undergo frenotomy. The relevance of this particular study is rendered moot by an Food and Drug Administration warning that benzocaine gels should not routinely be used in neonates because of the risk of methemoglobinemia (www.fda.gov/ForConsumers/ConsumerUpdates/ucm306062.htm retrieved on: December 13, 2016)
The seventh study, by Yousefi et al., 10 published in 2015 included 50 pediatric patients less than 8 years old, with a mean age of 32 months, with significant ankyloglossia (Hazelbaker's appearance score <8), who were randomly assigned into two groups: simple release (frenulotomy) or Z-plasty (frenuloplasty). All procedures were done under general anesthesia. Ten percent (five patients) of the patients were diagnosed in the neonatal period, and 27 patients were still breastfeeding. The parents, who were blinded for the type of procedure, were interviewed by questionnaire 3 months later. Surgery, in general, had a significant effect on all variables measured in this study. Z-plasty had a greater effect on articulation, breast pain, tongue movement, and parent satisfaction than simple release (p < 0.05). Z-plasty and simple release had the same effect on breastfeeding, latching, and sucking. The conclusion of the authors is that Z-plasty is the preferred surgical method to address tongue tie due to a greater improvement in mother's breast pain, pronunciation and speech, tongue movement, and parental satisfaction.
The eighth study, by Shavit et al., 11 published in 2016 included 42 infants less than 3 months old, with a mean age of about 21 days, with type three or four tongue tie, which were referred to a pediatric craniofacial clinic of a tertiary medical center. The infants were randomized to two different analgesic agents: 2% Tetracaine oral gel or 20% Benzocaine oral gel. The surgeon and nurse who performed the procedure were blinded to infant group assignment and the analgesic agent was applied by the principal investigator. The primary outcome, pain score by the Neonatal Facial Coding System (NFCS) was determined by two trained NFCS raters who were blinded to the group allocation. No differences between groups were found in the NFCS scores before frenotomy and during frenotomy.
Discussion
We showed that the yearly number of tongue tie-related articles has increased dramatically in the past few years, demonstrating an obviously increasing interest in this controversial topic. We note, however, that most articles are case reports or series, reviews, or editorials, and opinions, and in terms of hierarchy of evidence, not very “strong”. Most, if not all, of these articles do not provide the level of evidence required to publish convincing guidelines, hence the continuing public debate on the topic. It is quite amazing that out of over 500 articles, only eight are RCTs: five are related to short-term breastfeeding outcomes1,5–8 and three discuss technical considerations regarding the procedure itself.9–11 In the double-blinded studies where a sham operation was performed,1,6,7 pain scores were consistently improved by frenotomy, while the effect on latch was at best nonsignificant. Unfortunately, since in these studies outcomes were measured by different means and scores, a meta-analysis was not feasible and therefore there is not sufficient information for clinical guidance.
In view of the controversy, we believe that RCTs are ethically justifiable and mandated in this field of medicine. Technically, a clear source of bias is that blinding is extraordinarily difficult to maintain for a long period of time, since sooner or later, caregivers or mothers will easily find out whether the procedure was performed or not. For instance, in Emond study 44 out of 52 mothers of infants randomized to “standard care” (control group, no frenotomy) on day 5 of the study had requested a frenotomy, while in the same study, early frenotomy did not result in an objective improvement in breastfeeding at 5 days. 5 Nevertheless, from this literature survey and from the 10 SR published to date, it is obvious that many questions remain unanswered. The following are among them: can we better define tongue ties that will benefit from frenotomy from those that frenotomy will not help relieve symptoms? If frenotomy is to be performed, what is the ideal timing for it? Can grade three and four tongue tie (“submucosal” tongue tie, or “posterior” tongue tie) benefit from frenotomy? Besides breastfeeding issues, are there other long-term outcomes (speech clarity, dental and gingival health, social issues, etc…) that might be improved by frenotomy? If the trend that we evidenced in the number and the quality of tongue tie-related publications continues, we speculate (and hope) that much more solid evidence should accumulate over the next few years about the diagnosis and management of tongue tie, putting an end to the controversy about this condition.
Footnotes
Disclosure Statement
No competing financial interests exist.