
Abstract
Abstract
Aim:
As conjugated linoleic acid (CLA)is a potential growth promotor in newborns, the present pilot study aimed at measuring the effect of synbiotic supplementation on breast milk CLA level.
Materials and Methods:
Sixty lactating mothers were randomly allocated to take either synbiotic (n = 31) or placebo (n = 29) for 30 days. Maternal anthropometric indices were measured at the onset and end of the study by standard methods and body mass index was calculated. Information on food intake was collected by using a 24 hours 24-hour recall method for 2 days and food record questionnaire for 1 day. Breast milk lipids were extracted and CLA level was quantified by gas chromatography.
Results:
No significant differences were observed in the baseline mean breast milk concentrations of Fatty acids (FAs) between the synbiotic and placebo groups (p > 0.05). The CLA content of breast milk increased significantly by 58% (from 0.19 ± 0.15 to 0.30 ± 0.22 mmol/L) in the supplemented group, whereas it decrease decreased slightly but not significantly by 14% (from 0.22 ± 0.14 to 0.19 ± 0.10 mmol/L) in the placebo group. After adjustment for covariates, the CLA content of breast milk was significantly higher in the supplemented group compared with placebo group after the intervention (p = 0.03). The ratio of total n − 6:3 increased significantly over time in both groups, but was not different among groups (p < 0.05).
Conclusions:
This pilot study showed that supplementation of lactating women with synbiotic, resulted in increased breast milk CLA composition. Further research using different species of probiotic bacteria and analysis of maternal and infant plasma FAs would be beneficial.
Introduction
H
Materials and Methods
Sixty-three volunteer lactating women from urban areas of Tabriz city who exclusively breastfed their infants aged 90 days were selected for a double-blind, randomized, placebo-controlled trial parallel-group study.
All infants were full term with birth weights between 2,500 and 4,000 g and had been exclusively breastfed for 3 months. Mothers and infants were ineligible if they have had any clinical evidence of chronic illness or gastrointestinal disorders, or if they have received antibiotics, probiotic, or symbiotic supplementation in the month preceding the selection. The study protocol was approved by the Ethics Committee of Tabriz University of Medical Sciences and registered in the registration center for clinical trials in Iran (Code: IRCT201110181197 N12). All subjects were informed about the content of the study and an informed consent was obtained.
The participants were randomly allocated into two treatment groups to take either synbiotic supplements (n = 32) or placebo (n = 31). Assignment was done by computer-generated random number lists. Each synbiotic supplement (as documented by the manufacturer, Protexin; Probiotics International Ltd., Lopen Head, Somerset, United Kingdom) contained seven strains of friendly bacteria (Lactobacillus casei PXN 37, Lactobacillus rhamnosus PXN 54, Streptococcus thermophilus PXN 66, Bififidobacterium breve PXN 25, Lactobacillus acidophilus PXN 35, Bififidobacterium longum PXN 30, Lactobacillus bulgaricus PXN 39), (and prebiotic) (fructooligosaccharide) (as documented by the manufacturer).
The synbiotic group consumed a daily dose of a mixture of these strains (2.0 × 108 Colony Forming Unit) and fructooligosaccharide (394 mg), 30 minutes after meal during the intervention period of 30 days.
As a measure of agreement compliance, unused supplements were counted by an independent investigator. A computer-generated random sequence mentioned to the random allocation of subjects to study groups was kept in a remote secure situation and conducted by an independent third party, who was not involved with the clinical conduct of study until all study data were collected and certifified.
Lactating mothers and those involved in enrolling participants, administering interventions, evaluating outcomes, and analyzing data were blind to group assignments.
Demographic data (i.e., age), and clinical data (i.e., health status) were obtained through interview at the onset and end of the intervention. Maternal anthropometric indices were measured at the onset and end of the study. Body weight of each subject was measured to the nearest 0.1 kg using Seca as a weight scale; participants were weighed in light clothing without shoes. Height of subjects was measured with barefoot and using an amounted tape with the subject's arm hanging freely at their sides and recorded to the nearest 0.5 cm. Body mass index (BMI) was calculated as the weight in kilograms divided by the height in square meters (kg/m2). Information on food intake was collected by using a 24 hours 24-hour recall method for 2 days and food record questionnaire for 1 day before the supplementation and at the end of the study. Dietary intake of subjects was analyzed by nutritionist IV software program.
Breast milk samples were collected in sterile glass bottles by manual expression before nursing the baby in the morning, frozen immediately, and stored at −70°C until analysis. Milk was thawed, and fatty acid analysis performed on whole milk samples as previously described. Lipids were extracted with chloroform: methanol chloroform:methanol (2:1) using butylated hydroxyanisole as an antioxidant. Fatty acid methyl esters from milk lipid extracts were prepared by acid transmethylation using 1% H2SO4 in methanol. Breast milk CLA content was quantified by gas chromatography (GC).
All data were expressed as group means mean and standard deviations. Normal distribution of data was analyzed with the Kolmogorov–Smirnov test. Between-group comparisons were made by independent t-test and χ2. Paired t-test was used to evaluate the difference between variables in each group before and after intervention. Difference between the means mean of breast milk fatty acid content in supplemented and placebo groups was analyzed using analysis of covariance while controlling for maternal BMI and energy, fat, and carbohydrate intakes. Data were analyzed using SPSS statistical package, version 16 (SPSS, Inc., Chicago, IL). A p-value <0.05 was considered as statistically significant.
Results
Sixty mothers (31 in supplemented group and 29 in placebo group) completed the study (Fig. 1)
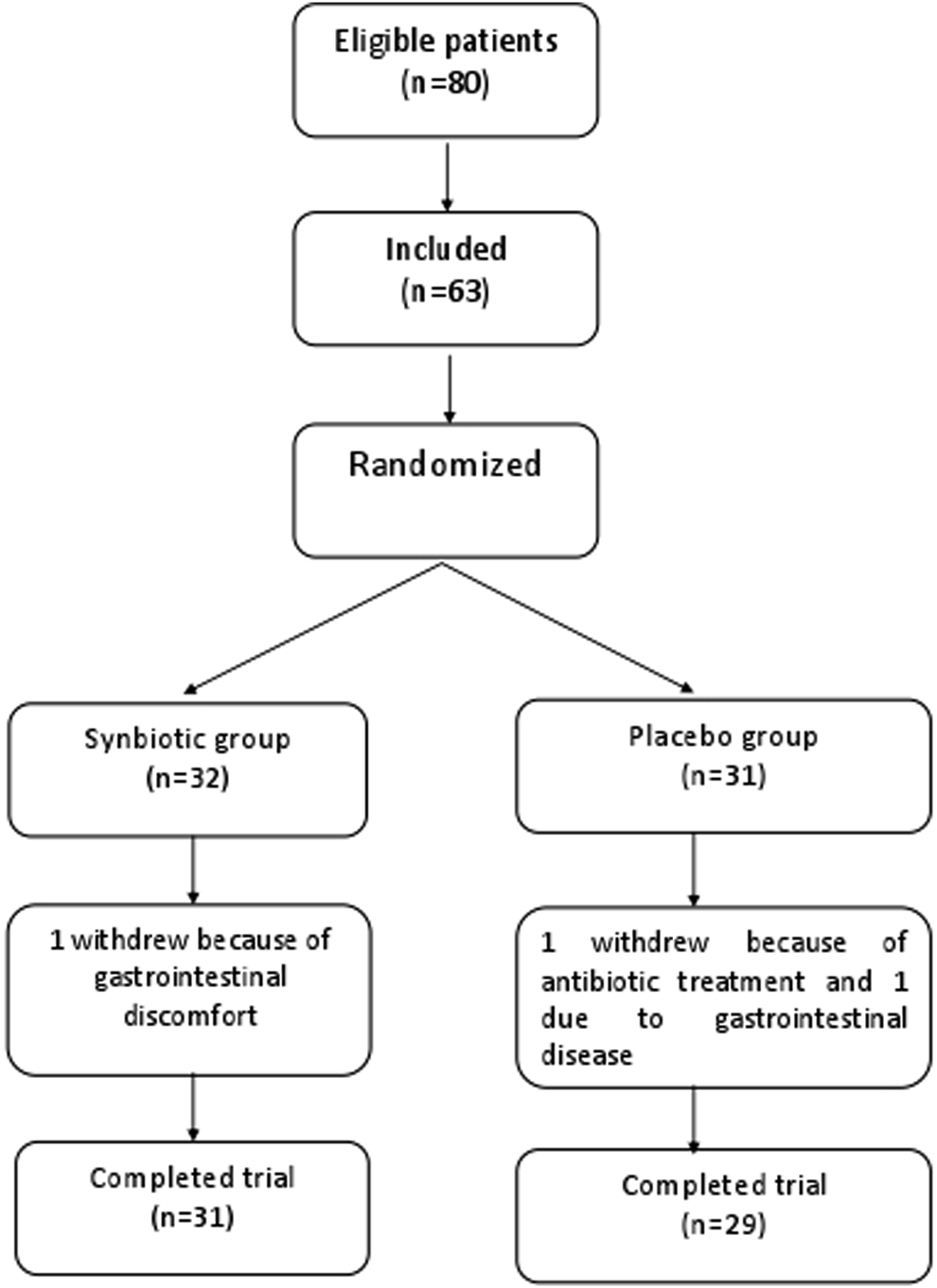
Flowchart for patient enrollment, randomization, and retention.
The comparison of mothers' and infants' anthropometric and demographic measures in two groups is shown in Table 1, There was no significant difference in the baseline measures between the supplemented and placebo groups. Maternal weight and BMI increased in the supplemented group and decreased significantly in the placebo group at the end of the study (p < 0.01).
Independent t-test.
χ2 test.
BMI, body mass index.
As shown in Table 2 the mean intake of energy, carbohydrate, and protein decreased in the placebo group, and was significantly lower for energy and all macronutrients at the end of the intervention. These variables increased slightly in the synbiotic group. The changes in total energy and micronutrient intake were significantly different between two groups after the intervention (p < 0.05).
Paired t-test.
The mean breast milk concentrations of fatty acids before and after intervention in both study groups are compared in Table 3. No significant differences were observed in the baseline mean breast milk concentrations of FAs between the synbiotic and placebo groups (p > 0.05). The CLA content of breast milk increased significantly by 58% (from 0.19 ± 0.15 to 0.30 ± 0.22 mmol/L) in the supplemented group, whereas it decrease decreased slightly but not significantly by 14% (from 0.22 ± 0.14 to 0.19 ± 0.10 mmol/L) in the placebo group. After adjustment for covariates (maternal BMI and energy, fat, and carbohydrate intakes), the CLA content of breast milk was significantly higher in the supplemented group compared with placebo group after the intervention (p = 0.03). The ratio of total n − 6:3 increased significantly over time in both groups, but was not different among groups (p < 0.05). No remarkable changes were observed in the other FAs content of breast milk after intervention. There were no significant correlations between dietary intake of LA and breast milk CLA composition (data not shown).
Paired t-test analysis.
ANCOVA: adjusted for dietary before supplementation values and calorie, fat, and carbohydrate intakes and mother's BMI.
CLA, conjugated linoleic acid.
Discussion
Human breast milk as the ideal infant nutrition can be improved by maternal nutritional modification The results of the present pilot study demonstrated that supplementing the maternal diet of lactating women, with synbiotic for 30 days, heightened CLA content in human milk without any significant change on other FAs content Previous studies have reported that the fatty acid composition of breast milk clearly depend depends on dietary intake. 8 In this study, maternal diet was controlled as covariate factor, so it can be assumed that the positive changes are due to the synbiotic supplementation. Comparable with our results, Apas et al. reported that the probiotic treatment given to the lactating goats modified the lipid profile of the milk, with a significant increase in the CLA content (from 0.0093 to 0.232 g of FA/L of milk). 9
In this study, no significant correlations were found between dietary intake of CLA and breast milk CLA composition. Several studies concluded that diet is the main factors factor affecting the milk FA profile, including CLA isomer content, while whereas some others have reported that endogenous synthesis represents the major source of CLA in milk fat. 10 Piperova et al. have shown that the principal source of milk CLA would be the postabsorptive synthesis. 11
The bioproduction of CLA by various probiotic bacteria have has been reported in previous studies. Ogawa et al. reported the production of CLA from free linoleic acid by Lactobacillus acidophilus. 12 Raimondi et al. reported that the strain Bifidobacterium breveWC breve WC 0421 was the best CLA producer, converting LA into 68.8% 9cis, 11trans-CLA, and 25.1% 9trans, and 11 trans-CLA. 13 All of these findings suggest that CLA is synthesized as an intermediate via through biohydrogenation of LA to stearic acid by some anaerobic bacteria,; however, the mechanism of CLA formation and the precise structure of the CLA produced has not been elucidated in detail. In the present study, synbiotic supplements were used, which contain probiotic (fructoligosaccharides (FOS)) in addition to probiotic bactriabacteria. It has been demonstrated that prebiotics prebiotic fermentation resulted in a reduction in intestinal PH pH through promoting the production of SCFA. 14
This study has some limitations. The plasma fatty acids were not analyzed. In addition, various isomers of CLA were not estimated in breast milk. Randomly assigning women to either a synbiotic supplement or placebo and adjusting for maternal diet is some strength of this study.
In conclusion, this pilot study showed that after adjusting for dietary intake, supplementation of lactating women with a synbiotic, resulted in increased breast milk CLA composition. Further research using different species of probiotic bacteria and analysis of maternal and infant plasma FAs would be beneficial.
Footnotes
Disclosure Statement
No competing financial interests exist.