
Abstract
Abstract
Background:
Studies on prevalence and effects of breastfeeding call for reliable and precise data collection to optimize infant nutrition, growth, and health. Data on breastfeeding and infant nutrition are at risk of, for example, recall bias or social desirability bias.
Objective:
The aim of the present analysis was to compare data on infant nutrition, that is, breastfeeding, use of infant formula, and introduction to complementary foods, obtained by four different methods. We assumed that weekly short message service (SMS) questions were the most reliable method, to which the other methods were compared.
Design:
The study population was part of the Odense Child Cohort. The four methods used were: (a) self-administered questionnaire 3 months postpartum, (b) self-administered questionnaire 18 months postpartum, (c) registrations from health visitors visiting the families several times within the first year of life, and (d) weekly SMS questions introduced shortly after birth.
Results:
In total, 639 singleton mothers with data from all four methods were included. The proportion of mothers initiating breastfeeding varied from 86% to 97%, the mean duration of exclusive breastfeeding from 12 to 19 weeks, and the mean age when introduced to complementary foods from 19 to 21 weeks. The mean duration of any breastfeeding was 33 weeks across methods.
Conclusions:
Compared with the weekly SMS questions, the self-administered questionnaires and the health visitors' reports resulted in a greater proportion of mothers with an unknown breastfeeding status, a longer duration of exclusive breastfeeding and later introduction to complementary foods, while the duration of any breastfeeding did not differ.
Introduction
S
Initiation and duration of breastfeeding and age of introduction to complementary foods have important effects on growth and development as well as current and long-term health.4–6 A limitation in many studies on this topic is that data on breastfeeding, use of infant formula, and introduction to complementary foods are inaccurate. In addition, observational studies in general are at risk of self-reporting bias (or social desirability bias), that is, respondents tend to underreport “inappropriate” behaviors, and at risk of recall bias since the memory recall might be inaccurate. 7 It is therefore important to evaluate and identify the most reliable methods to collect this type of data.
Over the past decade, the use of technology-based methods in nutritional epidemiological studies has been introduced.8–10 Some of the major advantages of this type of data collection are the reduced recall bias, the availability, and ease of use. Short message service (SMS) for other health-related purposes than data capture is widespread and well described. 10 A preliminary report of the SMS methodology as data collection method was published recently. 11
The aim of the present analysis was to compare measures of breastfeeding initiation, the use of infant formula within breastfeeding establishment, the duration of exclusive and any breastfeeding, and the timing of introduction to complementary foods among 639 singleton mothers with data from four different sources; self-administered questionnaires at 3 (termed Q3) and 18 (termed Q4) months postpartum, health visitors' written reports with intervals of ∼2 months within the first year postpartum, and weekly SMS questions since birth.
We assumed that the weekly SMS questions were the most reliable method due to the frequent distribution and the reduced recall bias, to which the three other methods were compared.
Subjects and Methods
Participants
The Odense Child Cohort is a prospective birth cohort consisting of children born in the municipality of Odense (∼190,000 inhabitants), Denmark from June 2010 to October 2013. The cohort is subjected to several questionnaires and physical examinations, including collection of biological material throughout pregnancy, infancy, and childhood, as well as access to medical hospital records, data from public health visitors, general practitioners, and national health databases, described in detail elsewhere. 12 Written information about the present study on infant feeding and early nutrition was sent to the participating mothers during pregnancy.
In total, 2,874 mothers were included in the cohort. 12 In the present analysis, we included only singleton mothers who had returned both Q3 and Q4, were seen at least once by a health visitor, and had received the SMS questions at least once (n = 639). An overview of the timing of the different data collection methods used in this study and the number of participating mothers within each group is shown in Table 1.
From June 2010 to November 2013 the visits were distributed as shown.
First time 3 days postpartum and preferably until the infant was both introduced to complementary foods and no longer being breastfed.
From June 2011, families with older siblings did no longer get the late visit.
Only within the first few hours/days after birth.
pp, postpartum; SMS, short message service.
Data on infant feeding from the questionnaires
Q3 contained 134 questions, of which 14 referred to breastfeeding and the use of infant formula, while Q4 contained 180 questions, of which 11 referred to breastfeeding and the use of infant formula. Neither questionnaires contained questions on the timing of introduction to complementary foods.
Data on infant feeding from health visitors' reports
As part of the Danish public health program, a health visitor (i.e., an educated nurse with special training in neonatal and infant care) repeatedly visited the infant and the family in their home during the first year of life; did anthropometric measurements, assessed and gave advice on nutrition, development, and overall health. Beside the planned visits, families could contact their health visitor for extra visits, have telephone consultations, or see the health visitor in a public clinic. Each consultation was registered as a “contact” in an electronic filing system with the possibility of adding a corresponding “note,” for example, on current nutrition.
Data on infant feeding from SMS questions
Mothers giving birth from April 2012 until October 2013 received weekly SMS text messages with questions on infant feeding. The mothers received the same three to five SMS questions (Table 2) once a week, first time 3 days postpartum. The SMS tracking system was provided by SMS Track ApS (Esbjerg, Denmark).
Sent only if the response to the previous question was “Yes.”
Definition of different feeding types
The WHO defines exclusive breastfeeding as the infant receiving no other food or drink, not even water, than breast milk, which may be expressed from the mother herself or from a wet nurse. Oral rehydration salts, vitamins, minerals, and medicines in the form of drops or syrups are allowed. 2
Since the use of infant formula along with breastfeeding more than halved from the first to the second week after birth according to the SMS questions, we did two calculations on the duration of exclusive breastfeeding based on the SMS questions—one calculation accepting supplementation with infant formula in the first week (i.e., the first few days after birth), but not afterward, and one calculation not accepting any supplementation with infant formula at all. In Denmark, it is not common practice (nor recommended) to supplement breastfeeding with water, fruit juices, or teas.
Regarding the health visitors' registrations, the definition of exclusive breastfeeding is based on the recommendation from the Danish Health Authority, allowing up to one infant formula meal per week.
Partial breastfeeding was defined as breastfeeding along with supplements of infant formula and/or complementary foods. The duration of any breastfeeding would be the sum of the duration of exclusive and/or partial breastfeeding.
Complementary foods were defined as by the ESPGHAN Committee on Nutrition, that is, all solid and liquid foods other than breast milk or infant formula. 6
If a mother stated having never breastfed, she would be categorized as “truly never breastfeeding,” if she—according to the medical hospital records—had never initiated breastfeeding.
Definition of age
One month would equal 4.3 weeks or 30.4 days postpartum.
Ethics
The study was approved by the Danish Data Protection Agency (ref. 12/26892) and The Regional Committees on Health Research Ethics for Southern Denmark (ref. S-20090130, sub protocols 12, 18, and 37). The study complied with the Declaration of Helsinki II.
Analysis
Descriptive statistics were used to describe the participating mothers and their infants. Questionnaires and health visitors' reports were compared to SMS questions using Chi-square test for categorical variables and t-test for numerical variables. Survival curves of exclusive and any breastfeeding and introduction to complementary foods were made to visualize differences between the methods. Statistics were performed using STATA/IC 14.2 (Texas).
Results
Characteristics of the 639 mothers (and their infants) providing data from all four methods are shown in Table 3.
In terms of highest, completed education.
Lower and upper secondary school; vocational education and training.
Short-cycle higher education; medium-cycle higher education.
Long-cycle higher education (e.g., university).
Including smoking cessation during first trimester of pregnancy.
BMI, body mass index; BWZ, birth weight Z-score; SD, standard deviation.
Questionnaires
Mean age at date of completion of Q3 was 3.4 months (standard deviation [SD] 0.9, min–max 1.15–6.15). Mean age at date of completion of Q4 was 17.9 months (SD 0.8, min–max 16.6–25.6), with 4.5% (29) having no date of completion.
Health visitors' reports
A total of 7,373 contacts were registered with a mean of 7.9 contacts per mother (SD 6.5, min–max 1–63). Almost a fourth of the 7,373 contacts (23.2% [1,710]) had a note on current type of nutrition. Of the 639 mothers, 95.1% (608) had at least 1 note on nutrition in direct relationship to birth, while 3.0% (19) did not have a note on nutrition registered at any contact. An overview of the number of contacts, notes, and their distribution across individuals is listed in Supplementary Table S1 (Supplementary Data are available online at www.liebertpub.com/bfm).
SMS questions
Of the 639 mothers, 5.0% (32) dropped out while still breastfeeding. Another 7.4% (47) had one or more weeks with missing answers between their last week of reported breastfeeding and their first week of not breastfeeding. The mean duration of any breastfeeding did not differ when excluding this subgroup.
Comparison of the different data collection methods
The results on breastfeeding initiation and duration, the use of infant formula, and introduction to complementary foods based on Q3, Q4, health visitors' reports, and weekly SMS questions are shown in Table 4, and the corresponding survival curves are shown in Figure 1.
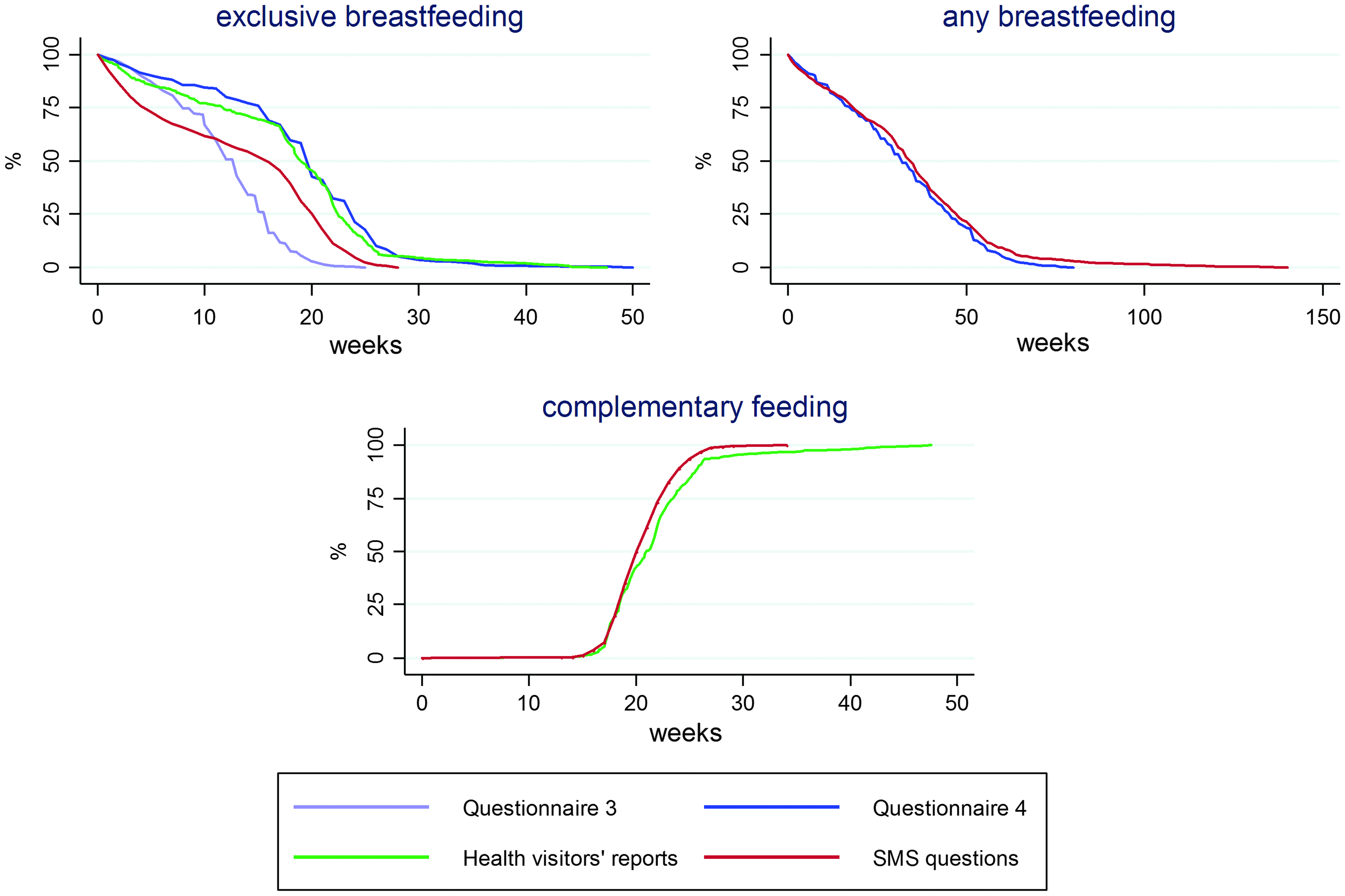
Time to breastfeeding cessation and introduction to complementary foods based on the different data collection methods. SMS, short message service. Color images available online at www.liebertpub.com/bfm
Numbers in bold specify a significant difference when compared to SMS data.
Proportion of self-reported “never breastfed” who were confirmed to have never breastfed by medical hospital records.
Including those still exclusively breastfeeding when fulfilling Q3, that is, duration = age at fulfillment (n = 12).
Infant formula supplementation in first week allowed.
Calculated from original mean ± SD (min–max) in days.
Based on the first week with a “Yes” to the question on complementary foods.
SD, standard deviation; SMS, short message service.
Noteworthy, the proportion of mothers with an unknown breastfeeding status was considerably higher based on Q4 (10.2%), health visitors' reports (2.0%), and Q3 (1.3%) compared with the SMS questions (0.2%). This resulted in a lower proportion of mothers reporting breastfeeding initiation based in Q4 and health visitors' reports compared with the SMS questions. Similar proportions were found in Q3 compared with the SMS questions.
The use of infant formula in the first week, that is, within breastfeeding establishment, varied from 10.1% (health visitors' reports) to 27.6% (SMS). Only the SMS questions revealed a decline in the second week to 12.9% (76/589), that is, 20.5% (92) of the 449 mothers exclusively breastfeeding in the second week had supplemented with infant formula in the first week. As specified in Definition of different feeding types, Subjects and Methods, we did two calculations on duration of exclusive breastfeeding—one accepting the supplementation with infant formula in the first week but not afterward and one not accepting any supplementation at all. In Table 4, we only present the duration of exclusive breastfeeding based on the SMS questions with allowance for infant formula in the first week.
Discussion
Compared to the weekly SMS questions, we found that the other methods revealed a higher number of mothers with an unknown breastfeeding status and, probably thereby, a lower number of mothers initiating breastfeeding, a less frequent use of infant formula within breastfeeding establishment (i.e., in the first week postpartum), a longer duration of exclusive breastfeeding, and a later introduction to complementary foods, while the duration of any breastfeeding did not differ. The number of mothers reporting to have never breastfed did not differ (from 2.2% to 4.5%), but when investigating the medical hospital records, we found that only 0.6% had truly never breastfed.
This kind of comparison of more traditional data collection methods to frequent SMS questions has—to our knowledge—not previously been performed in studies on infant nutrition.
Several other studies have compared more traditional data collection methods to each other, investigating differences on both short and long term. A small Croatian study published in 2012 (n = 157) found a significantly different rate of in-hospital exclusive breastfeeding, varying from 3% to 82% based on once-daily observations, every-feed observations, interview with the mother before discharge, and newborn examination form completed on discharge. An extensive supplemental use of infant formula (97%) was found only in the every-feed observations and the maternal reports. 13 In 2011, a comparison of two commonly used data sources for assessing breastfeeding rates in the United States, the National Immunization Survey (telephone survey, n = 2,337) and the California Newborn Screen (hospital staff collected data, n = 508,277) was published. These studies suggest that telephone surveys and staff collected data produced similar results regarding the prevalence of any breastfeeding few days after birth, while the prevalence of exclusive breastfeeding few days after birth significantly differed. 14
Questionnaires as data collection method
The questionnaires applied in this study were based on several other, previously validated, questionnaires. However, the questionnaires were not validated in their final form for this population. This was evident regarding the registration of date of completion and the registration of duration of exclusive and any breastfeeding, where the mothers were to add the duration in both months and corresponding days, which led to several misunderstandings. In addition, some recall bias occurred; this was obvious when investigating “any use of infant formula.” Of the 419 mothers confirming any use of infant formula in Q3, 4.8% (20) denied any previous use of infant formula when asked again in Q4. Finally, the questionnaires did not contain any questions on timing of introduction to complementary foods.
Health visitors' reports as data collection method
The visits from the health visitors were widely accepted by the families, and data from these visits were easily accessible for research purposes. On the contrary, visits might be registered differently between individual health visitors and some invalid registrations occurred, especially regarding dates, for example, some had a duration of exclusive breastfeeding of less than zero or more than 250 days in the present study. As stated in Definition of different feeding types, Subjects and Methods, section, the health visitors' registrations on exclusive breastfeeding includes up to one infant formula meal per week, challenging the comparison of methods. The duration of any breastfeeding could not be obtained from the health visitors' reports due to the absence of a breastfeeding cessation date in more than half of the registrations on partial breastfeeding. Finally, information bias may occur in registrations from mothers or families with certain challenges leading to more visits or contacts.
SMS questions as data collection method
A Scottish study published in 2012 (n = 329) did not compare SMS to other data collection methods but evaluated the reliability, validity, acceptability, and practicality of SMS as a data collection method. The approach used to test the reliability might be questioned, but the high level of acceptability reported by the participants and the practicality reported by the researchers are relevant. 10
One issue to consider is the risk of the weekly SMS questions being an “intervention in disguise,” that is, acting as a motivational tool. An Australian study published in 2014 (n = 334) tested if a weekly text message intervention for 8 weeks could increase the rates of any breastfeeding and improve breastfeeding self-efficacy and coping. The wording of the SMS was rather neutral, asking the mothers how breastfeeding was going or whether they had stopped. The mothers were supposed to answer using standard responses automatically leading to a second SMS with a more encouraging, helpful, or advisory wording, including a phone number to be used for further help. The data collection also included online surveys in weeks zero and nine. The study showed a smaller decrease in exclusive breastfeeding in the intervention group compared with the control group (6% versus 14%), and the intervention group demonstrated active coping of breastfeeding problems. 15 A Chinese study published in 2014 (n = 582) assessed the effect of an SMS intervention on the duration of exclusive breastfeeding. The intervention group had a longer median duration of exclusive breastfeeding, a higher rate of exclusive breastfeeding at 6 months of age, and a lower rate of introduction to complementary foods before 4 months of age. 16
In the present study, even if the SMS questions did actually improve the duration of breastfeeding, the effectiveness of the intervention does not explain the discrepancy between data obtained from questionnaires or health visitors' reports and SMS questions; also it does not make this discrepancy less important.
Overall, the weekly SMS questions give real-time data with a reduced recall bias, and in the present study, the SMS questions resulted in high response rates throughout the study period.
Conclusion
In conclusion, data from the self-administered questionnaires and the health visitors' reports indicated a lower use of infant formula within the breastfeeding establishment period, a longer duration of exclusive breastfeeding and a later introduction to complementary foods than indicated by data from the SMS questions. The duration of any breastfeeding based on data from the self-administered questionnaire at 18 months was similar to the one based on the SMS questions.
Our findings suggest that self-administered questionnaires and health staff registrations on a monthly or less frequent basis overestimate both the duration of exclusive breastfeeding and the timing of introduction to complementary foods. Surprisingly, the proportion of mothers not initiating breastfeeding was also overestimated, since mothers apparently tend to underreport their actual breastfeeding initiation, if the attempt fails within days or weeks postpartum.
Both the duration of exclusive breastfeeding and the timing of introduction to complementary foods are parameters used in many studies investigating the effects of breastfeeding and complementary foods on current and later health, development, and growth. Other studies use the duration of any breastfeeding that is not truncated at 6 months of age, as the exposure, which might be a more convenient approach. Based on our findings, the more traditional data collection methods might be sufficient to provide relevant data for such purposes.
Overall, our findings should further increase the awareness of the methods used in studies on infant nutrition. Concerning exclusive breastfeeding—either in-hospital or the overall duration—we recommend the use of a more frequent data collection method, for example, SMS questions with intervals of 1 or 2 weeks. When assessing the duration of any breastfeeding, more traditional and less frequent data collection methods are equivalent methods.
Footnotes
Acknowledgment
We want to thank all the participating children and their families, the employees at the Odense Child Cohort and our collaborators, including the coordinators and administration of the public health visitors in the municipality of Odense.
Disclosure Statement
As stated in the Affiliations, S.B. and L.N.J. are employees at Arla Foods Ingredients Group P/S, from where the present study is partially financed as an industrial PhD project. The other authors report no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.