
Abstract
Abstract
Background:
Equity in breastfeeding could reduce excess morbidity and mortality among children and mothers of color. Few programs that support breastfeeding have been evaluated for their capacity to create equity. The aim of this study was to assess the extent to which a diverse set of national breastfeeding programs actively promoted equity.
Subjects and Methods:
Qualitative data collection was conducted between December 2012 and July 2013 by visits to 29 of 58 breastfeeding programs selected by the funder. Programs underwent a site visit with open-ended interviews of staff. Investigators used Atlas.ti software to code data and content analysis of qualitative evaluation data. Key categories and themes were identified to answer the questions: how do the programs conceptualize equity? and how do the organizations operationalize an approach to equity?
Results:
Programs had widely divergent and often limited conceptualizations of equity. Nine categories describe the equity approaches' programs used. The social, political, and environmental contexts in which programs operated varied in the degree of challenge they pose for implementing equity-focused breastfeeding methods. We found only a few programs that matched the social, cultural, and economic realities and context of women of color.
Conclusions:
Breastfeeding equity programs need to explicitly define and envision outcomes, and need to identify equity inhibiting policies and practices. Equity attainment is more likely to emerge from institutional transformational processes that collaborate with the populations at risk. These findings have implications for other programs addressing equity in health.
Introduction
B
The need for equity in breastfeeding has received worldwide attention.8–11 A major Foundation, which supports thriving children, working families, and equitable communities, recognized that high-quality breastfeeding support should be available to all women, and that high rates of breastfeeding intent, initiation, success, exclusivity, and duration should be the norm across all populations. The Foundation developed a portfolio of grantees who provide services, training, or policy development throughout the United States to reduce disparities in breastfeeding. These sites included local community organizations that directly support pregnant women and new mothers, hospitals working to achieve Baby Friendly status, nonprofit national organizations, academic centers, and social media outlets. A subset of grantees was designated as priority sites because of their location in three states and one urban area where the Foundation has made a long-term commitment, or because they were regional or national nonprofit entities committed to increasing breastfeeding rates.
Consistent with the Foundation's long-standing commitment to racial equity, diversity, and inclusion, in 2010, the Foundation committed to integrating racial equity into its national grant-making strategies and posted a document that included its definition of racial equity on the website. At that time, breastfeeding grantees were not explicitly told that achieving racial equity was important in the grant application, were not asked how their program would promote racial equity, and were not given guidance on how to achieve equity. However, in 2011, the Foundation decided to examine the grantee characteristics that contributed to increasing equity. This study assessed the extent to which grantees actively promoted equity, and documented how equity approaches were operationalized. Because achieving equity is a long-term outcome, we did not expect to focus on a program's impact on breastfeeding rates. 12 All of the researchers, except one, were women of color, representing academia (V.K.H., D.L.R., S.N.G.-N., R.B., and Y.T.), philanthropy (D.D. was the Foundation Program Officer at the time of the evaluation), and an independent evaluator (P.E.B.). The independent evaluator previously had worked as an evaluation officer in a foundation and at the time of the study provided consultant services to communities of color.
Methods
The evaluation was conducted among the 29 of 51 grantees identified as priority sites by the Foundation (Fig. 1).
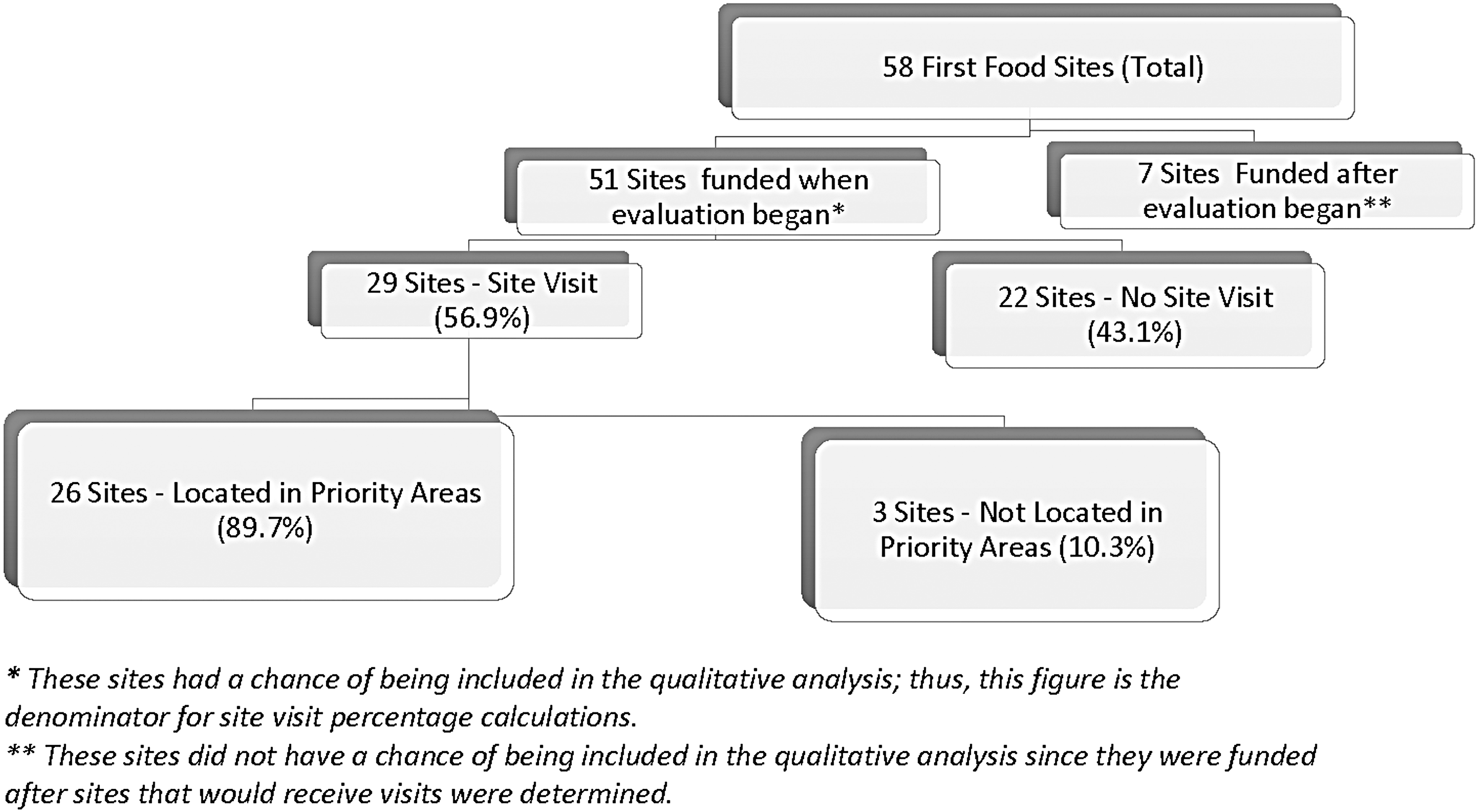
Distribution of programs included in qualitative analysis of equity in breastfeeding.
Participants were approached after the Foundation project officer sent a message to all grantees indicating that the evaluators would be contacting them. A site visit guide was used to document information about the grantees' environmental context, and an interview guide (Appendix 1) was used in face-to-face meetings with the program director and staff at their workplace (one director was not interviewed at her workplace). The interview guide was designed to document grantees' awareness, knowledge, conceptualization, and implementation of activities toward equity in breastfeeding, as well as to capture their self-reflection on the strengths and limitations to their ability to achieve equity. The Foundation's definition of racial equity formed the basis of development of the guide (Fig. 2). The race/ethnicity of each of the informants was not recorded; however, all informants from four of the community-funded grantees were people of color who resided or served their community.
Foundation definition of racial equity.
Qualitative data collection took place between December 2012 and July 2013. Except for two sites, most interviews include at least two researchers, the grantee director, and one or more grantee staff persons. Interviews were completed over a range of 2–3 hours. Audio recordings of interviews were professionally transcribed, then coded by four researchers (V.K.H., S.N.G.-N., D.L.R., and P.E.B.) using inductive coding with ATLAS.ti 8 (Berlin, Germany). A general inductive approach for analyzing qualitative evaluation data, a form of content analysis, was used.13,14
Data analysis was guided by the evaluation questions. Researchers repeatedly reviewed transcripts to code and independently to identify categories. Then, as a group, researchers compared and discussed the categories until a common set of categories emerged. These categories were used to generate consensus on the most important themes that answered the questions: How do the informants conceptualize equity? How do the organizations operationalize an approach to equity?
The study received IRB approval from the University of North Carolina at Chapel Hill.
Results
Three themes emerged that are germane to the goal of achieving health equity: diverse programmatic conceptualizations of equity; how conceptualizations of equity are operationalized through programmatic and/or institutional actions; and programs operate in unequal and culturally diverse contexts.
Diverse programmatic conceptualizations of equity
We asked informants to describe what they thought equity means, what they thought equity looks like in their organization, and how they approach (or would approach) equity in their organization. The informants appeared to be open to considering equity when the topic was raised, but equity generally was not already consciously built into the fabric of the organizations or in their programs.
[INFORMANT]: There's not a common definition … I think … we haven't done anything in particular within the [informant organization] to ensure equity–but what is my definition? Making sure that people have the same access regardless of their race, their gender, their creed, their sexual orientation. Making sure that people are treated fairly and they're not given biased treatment because of all of those things, so I think that, having said that and thinking about that, we need to do more. I don't think intentionally anyone in the [organization] or the [organization] is set up to be inequitable, but I think that we need to be more conscious about it and we haven't been in the past. (Participant 3)
A subset of informants defined equity as “having equal access to services.” Other informants identified inequity through a data analysis process (e.g., “comparing black to white” rates), but had no articulated vision of what should be done to attain “equal rates” for populations of color.
[INFORMANT]: Well my definition of equity is access and the outcomes appropriate for everyone regardless of race, religion, geography, ethnicity. And when we look at data around breastfeeding, it's pretty clear that we have to address equity better. (Participant 4.1)
One informant expressed an understanding of equity that involved targeting a vulnerable group to “bring them up to the level of the rest of the population.” In this case, the end goal was for everyone to have an equal opportunity to breastfeed. One interviewee phrased this as “accelerating the pace” of a vulnerable group's improvement by specially targeting them with existing evidence-based practices or being “culturally appropriate.”
[INFORMANT]: Well we understand that equity is involved with every one of all shades, all colors, and all ethnicities getting equal treatment and getting access to the same opportunities …, we're dealing with the African American population so the way we see it, equity is when we allow the opportunities that most … breastfeeding moms get. We give those opportunities to the African American communities so we can boost those numbers so everyone gets access to the same opportunities. (Participant 5.1)
The informant noted that targeting one group can, however, be challenging because some people see this action as discriminatory.
Few informants articulated the broader dimensions referred to in the Foundation's definition of racial equity, that is, historic policies, racism, or structural factors. At one site, one informant appeared uncomfortable discussing issues of racism and deflected the conversation toward program aspects considered to be supportive of all women's efforts to breastfeed.
One informant had a priori thoughts about the organizations' equity vision, which incorporated more than just health outcomes.
[INFORMANT]: Our vision is to see every mother, baby and family thrive in a healthy community. That's the vision. (Participant 9.1)
Equity conceptualizations operationalized in programmatic action
We grouped informant organizations' current actions and approaches toward equity into nine general categories (Table 1). These illustrate the varying degrees to which informants translated an equity approach. The nine are based on informants' stated or implied awareness of equity. Any one program may show aspects of multiple categories. The nine categories do not have a linear progression: that is, one category is not to be considered “better,” “worse,” “more,” or “less” than another.
Institutionalized-equity approach
These informants attempt to structure aspects of their operations, from Board composition to staffing to support equity-promoting actions. Developing an a priori culture of equity seems to result in fewer internal institutional roadblocks to improve the informant's ability to identify and address policy and sociostructural issues relevant to the community, thus facilitating the process of attaining equity. This was the least prevalent model.
Equity “add-on” approach
These organizations attach equity considerations as “add-ons.” They tend to maintain their existing institutional structures and processes, but attempt to add something they consider to be related to equity.
Cultural-matching approach
This approach characterizes many community-based programs run by people of color. This approach to equity focuses specifically on matching intervention approaches to the needs of women and families in the community. The cultural-matching approach tends to generate respectful, inclusive, and replicable models for addressing one component of equity—the effort to ensure that care is delivered in ways that respect the unique population context, history, culture, and needs. However, public policy and problems with institutional structures that may interfere with creating equity are not usually targeted.
Missionary approach
The missionary approach attempts to provide needed services in traditional mainstream ways. The design, programming, and implementation are usually delivered by people of a different ethnicity than the population served. The missionary approach fills basic needs for some services in underserved communities, but does not demonstrate cultural competency nor does it develop a pipeline to transition community members into the leadership of these programs.
Diversity approach
In this approach, the goal of achieving “minority representation” refers to diversity as their main equity intervention. In some cases, there is a limited understanding of the connection of the concept of diversity to power-sharing and incorporating alternative paradigms of action. These cases of diversity without power result in mere tokenism that does not transform toward equity. In other cases, the connection between diversity and power is understood and respected.
Equality “raise-all-boats” approach
The conflation of equality and equity is a common misunderstanding. Equality often focused on the service inputs—ensuring that they are delivered in the same way, equally to all population groups. Equality approaches may “raise all boats” equally, while still maintaining existing disparities. The “equal interventions” have been designed based on the needs of more privileged groups and, even if delivered equally, do not make up for the deficits in resources and opportunity experienced by historically and contemporarily oppressed and marginalized populations. In one instance, the Baby-Friendly Hospital Initiative, a “raising-all-boats” strategy, may work to improve outcomes by undoing some of the structural and cultural barriers to breastfeeding initiation, but does not address the posthospital discharge contextual inequities that affect long-term breastfeeding success.
Selective-equity approach
In this approach, informants may make a decision to limit the target of the intervention to one group or one dimension of equity. Organizations that use a selective-equity approach pick and choose which equity-promoting activities or population they will attempt to impact. For example, one academic center used bus advertisements to promote acceptance of breastfeeding in public place. This selective approach sometimes allows informants to avoid difficult discussions about racism.
Concerned non-action approach
Many informants know that inequities exist and report that they are truly concerned. However, for a variety of reasons, they may not initiate action because they need structured guidance on how to approach equity issues within their programs.
Low-awareness approach
A few informants do not consider equity attainment as part of their mandate.
Unequal and culturally diverse contexts
As noted in the Foundation's definition of racial equity, social, historical, economic, environmental, and institutional contexts contribute to the existence of inequities and ultimately influence the effectiveness of interventions. Conceptualizing, designing, and implementing culturally appropriate, historically and contemporary-responsive programming for the conditions of populations of color seemed to be areas of weakness for the 29 visited programs. Observed contextual issues that have the potential to interfere with a program's success or require more resources include the following:
• Inadequate transportation that makes it difficult for people to get to health or other services, or for service providers to get to clients. • Inadequate nutrition for families: An undernourished mother might question her ability to produce milk. People living in areas where the water and soil are known to be contaminated may question the safety of breastfeeding. • Shortages of basic resources that program personnel might assume are present and available in all communities: for example, access to fully stocked grocery stores versus a mini-mart or gas station as the source of people's diet. • Inhospitable circumstances, for example, having had prior bad experiences with agencies, including being disrespected. • Mainstream institutions work differently for different racial/cultural groups: for example, law enforcement, the judicial system, employment and income, and harmful environments. • Prior history of ill treatment and abuse (e.g., medical experimentations, sterilizations without consent, and taking indigenous peoples' lands) by the dominant society, resulting in some groups having low levels of trust. Those who have suffered have some kind of historical community memory and/or direct experience. • Extreme social burdens: for example, one informant described efforts to assist a woman who had several children and no income, and was homeless to address her immediate survival needs before breastfeeding could be a priority issue.
Program decisions can exacerbate contextual constraints, often creating more disadvantages. For example, one program faced loss of funding for salaries of peer counselors and had to scale back its programmatic activities. Program leaders decided to place the peer counselors in locations where a lactation consultant also existed to leverage resources. However, few lactation consultants operate in communities of color. A seemingly reasonable decision resulted in underresourced communities being further disadvantaged.
Discussion
Observations relevant to programmatic efforts to achieve equity emerged from the analysis of data collected during visits to the programs. We found that grantees have widely divergent, and in some cases, limited conceptualizations of how to achieve equity, with some more sustainable than others. We described nine ways that grantees operationalize their approach to equity. With the exception of Baby Friendly hospital grantees, equity approaches mainly targeted changing individual-level behaviors, including grantees that used the cultural matching approach. Approaches to equity that encourage changing institutional structures have more strength and sustainability compared to those that do not address and change systemic practices. The few efforts at higher level policy intervention tended to consider issues that may be common to all women, but not issues unique or more prevalent in the circumstances of women of color and low income.
The social, political, and environmental contexts in which the various programs operate vary greatly in the degree of challenge they pose for program implementation, or for women's ability to access or use the services provided. Traditional evidence-based programs and strategies often need to be altered or redesigned to accommodate contextual realities. Except for a few community-based, culturally matched programs, we found little evidence of program implementation strategies that matched the social and cultural realities of women of color. Grantees that serve communities with transportation issues, food deserts, and inhospitable physical or built environments have a difficult task; however, Foundation resource allocation was unlikely designed or implemented with consideration of these contextual conditions of the communities served by grantees.
This is one of the first times that understandings and intentional practices around equity have been the focus of exploration and evaluation of a U.S.-based national breastfeeding program. This study was intended to be an initial examination of how the breastfeeding program grantees included racial equity into their work. We were able to characterize major differences in program approaches to equity. The findings suggest that grantees need to receive direct information about the Foundation's commitment to racial equity. We recommend that the Foundation explicitly informs grant applicants of the Foundation's decision to incorporate racial equity into grant-making strategies, provide tools to support equity planning, and evaluate instructions for monitoring progress toward equity. It is possible that some applicants might change their operational approach if this information is provided.
Implications of findings
The Foundation's national breastfeeding initiative broke important ground by encouraging organizations to promote equity. Once the Foundation successfully ties together the promotion of breastfeeding and the promotion of equity, there is the potential for developing extraordinary models for promoting progress on multiple levels and in multiple contexts toward national equity goals.
Inequities arise from historical, cultural, social contextual, and institutional factors. Achieving equity requires transformative actions that include changes to governance, policy, and social and cultural norms. 15 All grant recipients should be encouraged to participate in changing governance policy and norms. An inability to envision what equity looks like, and to see it both as process and outcome, may put organizations in a position to inadvertently reproduce or maintain the existing inequities. 16 Without a coherent roadmap for navigating these underlying challenges, programs will be limited in their ability to achieve substantial and sustainable change. Equity attainment in breastfeeding or in any health outcome is a long-term process that requires intentional processes in all policies, decisions, and actions. Equity is more likely to emerge from institutional transformational processes that collaborate with the populations at risk.
Footnotes
Acknowledgment
This work was supported by the W.K. Kellogg Foundation.
Disclosure Statement
No competing financial interests exist.