
Abstract
Abstract
Introduction:
Under some circumstances human milk (HM) extraction and refrigerated storage may be necessary. Depending on the length and on the type of cold storage, milk may lose some important properties, but current advices on safe HM storage are discordant. Moreover until now no data in literature were present on the effect of prolonged cold storage on biologically active components of the HM such as adrenomedullin (AM). This important peptide is involved in response to hypoxia and inflammation, associated with neovascularization, in several tissues. The aim is to evaluate: (a) the presence of AM in preterm and term HM and (b) the concentration of AM in refrigerated milk at 4°C at 24-hour intervals, up to 96 hours of storage.
Materials and Methods:
The experiment was repeated four times. Immediately after collection, each HM sample deriving from each mother was divided into two parts as follows: “Pool” line and “Single Mother” line. One part (Pool line) was pooled and then divided into five aliquots. The other part (Single Mother line) was divided into five aliquots. From each line, one aliquot was analyzed within 3 hours, while the others were stored in the refrigerator for 24, 48, 72, and 96 hours, respectively, and then analyzed. AM levels were determined using a specific ELISA test.
Results:
AM was detectable in all samples. Its concentration was significantly higher in preterm milk with respect to term milk (p < 0.05). Significant differences were observed during the cold storage: the AM levels decreased steadily during the storage and the remaining concentration at 96 hours is ∼2%.
Discussion:
This study provides evidences regarding the presence of AM in HM, regardless of the gestational age. In particular, the refrigeration of fresh HM in controlled conditions significantly affected its bioactivity and nutritional quality related with AM, already at 24 hours.
Introduction
B
Adrenomedullin (AM) is a C-amidated peptide, involved in response to hypoxia and inflammation, which are associated also with neovascularization. Recent studies indicate that AM is synthesized also in the mammary gland and secreted in breast milk, 8 although the data are discordant on its concentration in milk of mothers having delivered at term of the gestational age. In contrast, the presence of AM in HM and the variation in its concentration between the different milk maturation degrees and between healthy and pathological mothers suggest that AM may have an important role in the regulation of growth and maturation of the neonatal gastrointestinal tract.9–11
To elucidate some of the uncertainties regarding AM in HM, we evaluated: (a) the presence of AM in term and also in preterm HM and (b) the effect on AM concentration in refrigerated milk at 4°C at 24-hour intervals, up to 96 hours of storage.
Materials and Methods
Sample collection
HM samples were collected at the NICU of the University of Turin, from healthy mothers having delivered preterm and at term of gestational age. Standard exclusion criteria for HM donation set forth by Association of Human Milk Donor Banks (AIBLUD) guidelines were also applied. 3 Mothers admitted into the study gave signed and informed consent. The study protocol was approved by the local Ethics Committee of the Italian AIBLUD. The experiment was repeated four times to ensure reproducibility of the results; we enrolled three mothers for each time (total donating healthy mothers: 12). Fresh milk samples were collected at the same time (9–10 a.m.) into sterile, disposable, high-density polyethylene sealed bottles (Flormed, Naples, Italy). Milk was collected with standard extraction methods by means of an electric breast pump (Medela Symphony, Baar, Switzerland). Immediately after collection, each HM sample derived from each mother was divided into two parts: “Pool” line and “Single Mother” line. The “Pool” line part was pooled in a sterile bottle with the other “Pool” line parts derived from the other two mothers (total volume: 50 mL) and then divided into five aliquots. The “Single Mother” line part was immediately divided into five aliquots. From each line, one aliquot (0 hour) was immediately frozen at −80°C until the analysis. The other aliquots (24, 48, 72, and 96 hours) were stored in the refrigerator at 4°C in the NICU, respectively, for 24, 48, 72, and 96 hours and then immediately frozen at −80°C until the analysis. The replicate pools were kept separated and analyzed independently. The temperature of the refrigerator was constantly monitored by two mini data loggers equipped with internal probes (Testo 174T, Lenzkirch, Germany) placed on the bottom and top shelves of the NICU fridge and programmed to record the temperature every 5 minutes.
AM analysis
AM levels were determined using a specific ELISA test (SL007HU- Human adrenomedullin -ADM- ELISA Kit) according to the manufacturer's instructions (SunLong Biotech Co. Ltd., China). Investigators who performed the laboratory tests were blind to storage modalities. The assay detection limit is 0.05 ng/L, and the assay range is 2–40 ng/L. The assay is specific for Human AM.
Statistical analysis
Demographic characteristics of maternal and neonatal outcomes are reported as mean ± standard deviation (SD). AM concentrations are expressed as mean ± SD. Statistical analysis was performed using two-tailed paired t test and by Mann–Whitney two-sided U-test when data did not follow a Gaussian distribution. Comparison between groups was performed using ANOVA one-way test for multiple comparisons. A p < 0.05 was considered significant.
Results
Demographic characteristics
The 12 donor mothers were healthy women having delivered, 6 at term (mean gestational age at birth: 39 ± 1 weeks; mean birth weight: 3,010 ± 220 g) and 6 preterm (mean gestational age at birth: 30 ± 1 weeks; mean birth weight: 1,650 ± 140 g). Eight mothers delivered by vaginal and four by cesarean section. Five newborns were males and seven females. The mean date of delivery was one month before the donations.
AM levels
AM was detectable in all HM samples.
Its concentration was higher in preterm milk (mean: 200.0 ng/L; SD ±189.9 ng/L) with respect to term milk (mean 18.1 ng/L; SD ±10.9 ng/L), and the differences in concentration were significant (p < 0.05). AM was detectable also in all refrigerated milk samples, Table 1. As shown in Figure 1, significant (p < 0.05) differences in AM levels were observed during the cold storage. The data show a significant reduction of 56% in concentrations in all samples at 24 hours. The AM levels decreased steadily during the storage and the remaining concentration at 96 hours is ∼2%. This trend of reduction is similar in the “Pool” line and in the “Single mother” line. Indeed, a significant difference (p < 0.05) was found also when AM concentrations in milk samples were corrected for gestational age.
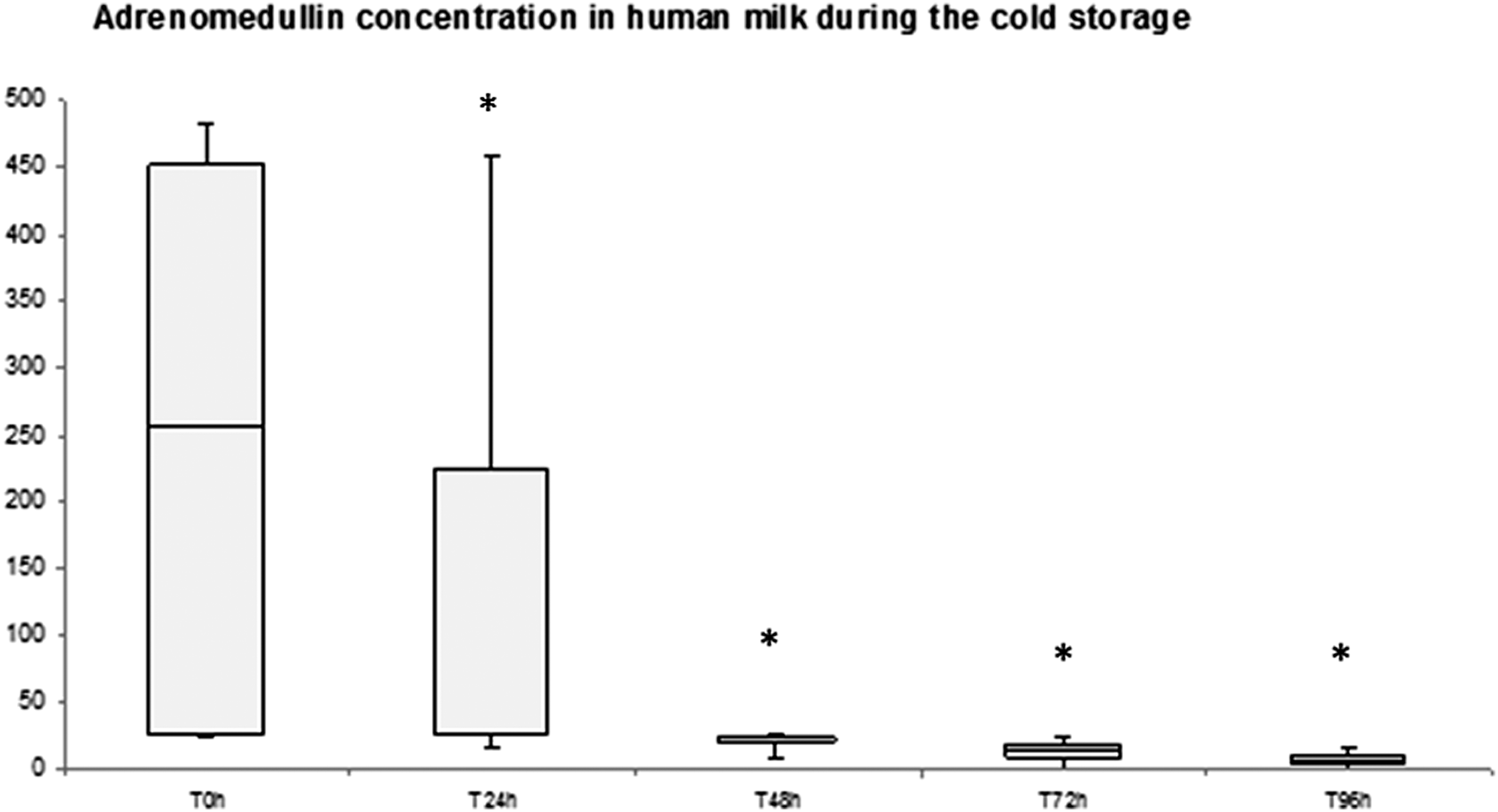
Adrenomedullin concentrations (ng/L) in total human milk samples during the cold storage at 4°C for 96 hours. The lower and upper bars represent the 5th and 95th centiles, respectively; interquartile range is indicated by the box, and median value is represented by the horizontal line in the box. *Significant differences between T0 hour and the other time points (p < 0.05).
Data are expressed as mean and SD.
SD, standard deviation.
Discussion
The biologically active components found in HM participate in multiple physiological processes, including modulation of gastrointestinal functions, microbial growth control, and immunoregulation. 12 Cold storage of HM is a common practice both in hospitals and at home, but the effect on these components is already unclear. The maximum refrigeration time for HM ranges between 24 hours and 8 days, according to current advices. Such variability reflects the heterogeneity of the scientific sources, which can be attributed to differences in the study design and in the methodological approaches. 5 Recent studies concluded that HM can be stored for 96 hours at 4°C without affecting the overall milk integrity, but several important biological compounds were not considered at all.6,7
Our study shows that prolonged refrigeration of HM at 4°C affects its original content of AM. This protein is not thermostable at 4°C: AM is significantly reduced (56%) at 24 hours and is nearly undetectable at 96 hours. We performed our analysis not only in HM pool but also in HM samples derived from the single mothers to compare the results on two different modalities of storage (HM banks and home, respectively). Our data show that the model of AM decrease is similar in both lines. Moreover we related the decreased content of the AM only at prolonged refrigerated storage because the protein stability, under different conditions such as freezing and thawing procedures, is certain. In this respect, Lev et al. 13 showed that the total protein amount remains unchanged during the storage at −80°C, data confirmed by Ahrabi et al. regarding the freezer storage, at −20°C, of HM for up to 9 months for refrigerated milk. 14 The thawing procedures were investigated recently by Handa et al., 15 and no changes in protein were observed between processing methods of thawing and warming of HM.
We detected AM in all HM samples collected, and these data are in agreement with the literature. Before the discovery of the presence of AM in mouse milk, 8 three previous studies have evaluated the presence of the AM in HM. Pio et al. and Ohta et al. focused their studies in HM of healthy mothers having delivered at term and obtained discordant results on AM concentrations.9–11 Ohta et al. detected AM only in 21% of samples (assay system IRMA) versus results of Pio et al., who found AM in all milk samples (radioimmunoassay RIA). Cekmen et al. analyzed HM of healthy and preeclamptic women and found AM in all samples (HPLC).9–11
Our data show for the first time the presence of this important peptide also in HM of mothers having delivered preterm infants and demonstrate that AM levels in preterm milk are significantly higher in respect to the term milk. Our results are in agreement with the previous literature demonstrating that AM levels in HM are higher than those reported in plasma; several human hormones and growth factors present in milk exceed their plasma concentration. 16 Anyway, the finding of significant changes in AM levels herein reported warrants further considerations. AM is a regulatory peptide and its expression was demonstrated in several tissues and biologic fluids such as plasma, cerebrospinal fluid, sweat, amniotic fluid, and urine.17–19 AM has been implicated in the modulation of several physiological functions, including cardiovascular tone, 20 central brain activity,21–24 bronchodilation, 25 renal function, 26 hormone secretion, 27 cell growth differentiation, 28 and immune response.29,30 Moreover AM has been investigated for its involvement in ischemia–reperfusion injury while in healthy infants has been shown to participate in the cascade of events promoting fetal/neonatal cardiovascular adaptation.22–24 AM has been also assessed for evaluation of benefits/side effects of in-utero vasodilation therapeutic strategies in pregnancies complicated by fetal chronic hypoxia.22–24 In this regard, an observation on AM and the occurrence of adverse neurological outcome has been reported in infants with congenital heart disease.22–24 Bearing in mind these important functions, it is possible to speculate that the presence of the active peptide AM in HM, and their variability in concentrations among milk degree (from colostrum to mature milk), gestational pathologies, and gestational age of delivery, could have some direct impact in the development of the neonate due to the several physiological activities that have been associated to it. In relation with the gastrointestinal tract, immunoreactive AM has been detected in human stomach, duodenum, jejunum, ileum, and colon, 31 and specific binding sites have been detected in rat stomach. 32 This distribution suggests a role for AM in the regulation of secretory-motor functions in the gastrointestinal tract, as well as in its development during the embryogenesis and the period immediately following birth. Since the developing intestine in the neonate is considered to be one of the main target organs for the growth factors present in HM, Pio et al. 9 demonstrated that milk has a growth promoting activity on human small intestinal epithelial cell line (Int-407). These authors suggest that since MoAb-G6 partially blocks the milk-induced growth, AM may be one of the growth factors present in milk. AM has also been described as an agent with antimicrobial activity against gastrointestinal microorganisms.29,30 This activity could be important for the protection of the neonate against gastroenteritis produced by intestinal pathogens. In the end, since some peptides are absorbed from the neonatal gastrointestinal tract and appear intact in plasma, 33 AM could also exert an activity in the modulation of tissue growth, as well as in the regulation of the immune system.
Finally, the present findings can also be of interest for future studies aimed at investigating the variability of AM concentrations in colostrum/transitional/mature milk under the same storage conditions and in the different gestational age of delivery. Moreover, it would be interesting to correlate the AM milk levels with the following parameters: AM plasma levels in mothers, frequency of breastfeeding, type of delivery, number of births, and also with gestational pathologies.
Conclusion
In conclusion, this study provides new and incremental evidences regarding the presence of adrenomedullin in HM, regardless of the gestational age at delivery. In particular, refrigeration of fresh HM in controlled conditions for 96 hours significantly affected its bioactivity and nutritional quality related with AM.
Footnotes
Acknowledgments
This study is part of the I.O. PhD International Program, under the auspices of the Italian Society of Neonatology and of the Neonatal Clinical Biochemistry Research Group, and was partially supported by grants to D.G. from “I Colori della Vita” Foundation, Italy.
Disclosure Statement
No competing financial interests exist.