
Abstract
Abstract
Objective:
The purpose of this study was to investigate the normal lingual frenulum anatomy in newborns and to evaluate tip–frenulum distance as an objective diagnostic tool for identifying newborns at risk for anterior and posterior tongue tie and breastfeeding difficulty.
Materials and Methods:
The distance from the tongue tip to the insertion of the lingual frenulum was measured in a group of 100 healthy newborns to establish normative data. The presence of a visible or palpable cord was noted. Inter-rater reliability was assessed. Breastfeeding surveys including a maternal pain scale and Infant Breastfeeding Assessment Tool (IBFAT) were administered on days of life 2 and 14 to determine whether these findings predict breastfeeding difficulty.
Results:
Mean tip–frenulum length was 9.07 mm. Intraclass correlation coefficient between observers for tip–frenulum length was 0.82. A visible cord was identified in 21 subjects (21%). A palpable cord was identified in 59 subjects (59%). Unweighted κ coefficients for inter-rater reliability of visible and palpable cords were 0.91 and 0.47, respectively. Visible cord and shorter tip–frenulum distance were independently predictive of higher maternal pain scores. A positive correlation was identified between tip–frenulum length and IBFAT scores for mothers with two or more previous breastfed children.
Conclusions:
Tongue tip–frenulum length correlated with maternal nipple pain, and was useful as an objective tool for identifying newborns at risk for ankyloglossia. Maternal breastfeeding experience appears to be an important factor in the link between tongue anatomy and breastfeeding difficulty. The presence of a palpable cord was variable across examiners, and should be interpreted with caution when evaluating newborns for posterior tongue tie.
Introduction
A
The diagnosis of ankyloglossia is typically subjective, reliant on the practitioner's assessment of the limitation in tongue movement, and clinical significance of the tethering. The Hazelbaker Assessment Tool for Lingual Frenulum Function was developed to identify infants with clinically significant ankyloglossia. 4 This tool includes measures of appearance and function, but has not been widely adopted in clinical practice as it is time consuming and demonstrates only moderate inter-relater reliability (κ = 0.49). 5 Many other classification systems have been employed to evaluate the structure and function of the frenulum and tongue (see Power and Murphy 3 for a review), but no one measure is simple, reliable, and validated for clinical use. Furthermore, cases in which the examination is unclear or doesn't match the history can present a clinical dilemma for physicians and parents.
There is very little published literature defining normal lingual frenulum variability in neonates, further complicating the issues of defining pathological ankyloglossia. In addition, the more recently defined entity of “posterior” or “submucosal” tongue tie is less obvious on examination and has no validated diagnostic criteria.6,7
The purpose of this study was to investigate the normal lingual frenulum anatomy in newborns, and to evaluate tip–frenulum distance as a simple, objective tool for identifying and characterizing frenulum anatomy in newborns. We then sought to determine whether this tip–frenulum length was correlated with breastfeeding difficulty in healthy newborn infants and their mothers.
Materials and Methods
This is a prospective cohort study approved by the University of Rochester Institutional Review Board.
Examination of newborns
A cohort of full-term infants born at a tertiary academic hospital and cared for in the standard birth center comprised the study group. An initial sample size of 100 newborns was selected as an estimated convenience sample. The research staff met with nursing staff on a scheduled periodic basis to review the census of new dyads on the hospital floors. All full-term neonates and their mothers were potential study candidates. Exclusion criteria included prematurity, time spent in the neonatal intensive care unit, craniofacial or chromosomal disorders, and prior oral or tongue surgery. Parents of term infants in the newborn nursery that met inclusion and exclusion criteria were approached and gave written informed consent.
Each newborn underwent examination of the oral cavity, including inspection and palpation of the floor of mouth for the presence or absence of a posterior band or cord, as outlined in prior publications for evaluation of posterior tongue tie.7,8 The tongue was lifted gently with two fingers to expose the frenulum, noting any potential posterior tethering under the mucosal curtain. Each subject also underwent measurement of the distance from the tip of the tongue to the attachment of the lingual frenulum (Fig. 1). The tip of the tongue was defined as the junction between the rough dorsal surface of the tongue (covered with filiform papillae) and the smooth ventral surface. This junction was readily apparent even for children with short tip–frenulum distances, where the anterior tongue may be notched or heart shaped. Inter-rater reliability was calculated for each measurement, and reported as the intraclass correlation coefficient (for continuous measurements) and κ (for categorical measurements). Secondary assessments included the presence of a thickened maxillary frenum or any apparent craniofacial anomaly. These data points were collected prospectively in a deidentified patient database. Parents were blinded to the result of their child's oral cavity examination before answering the survey questions.
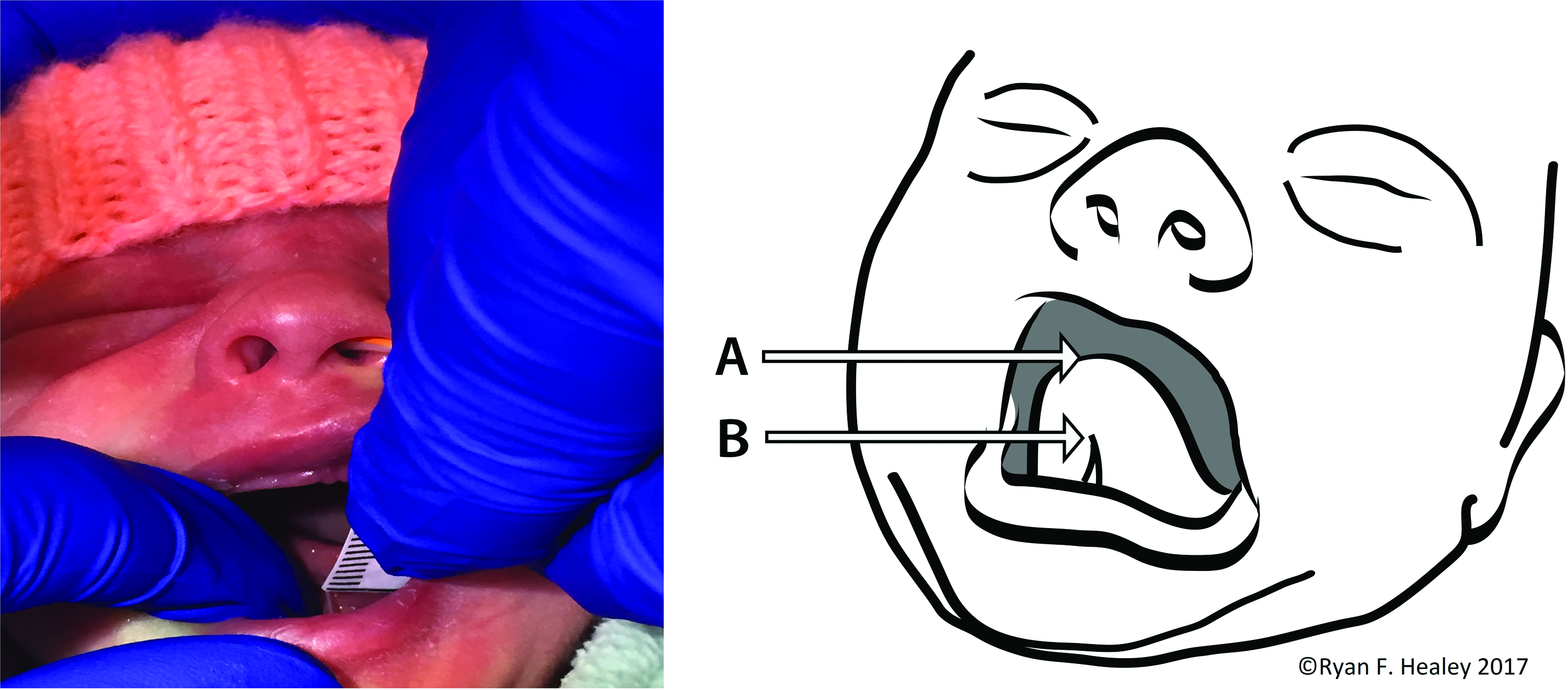
Tip–frenulum measurement. With the infant's tongue retracted superiorly, the distance from the junction of the dorsal papillated and ventral mucosal tongue
Breastfeeding survey
All mothers were asked to complete a survey including demographic data and questions about infant feeding. Surveys took place at least 48 hours after birth to allow adequate time for lactogenesis II and maternal familiarity with basic breastfeeding techniques, but within 1 week of birth to create a more homogeneous population for meaningful comparison. Demographic factors that may impact the physiology of infant latch and/or tongue tie, including maternal age, obstetric history, infant's APGAR scores at 1 and 5 minutes, and birth weight,9–12 were used for subgroup analysis. The Infant Breastfeeding Assessment Tool (IBFAT) (Appendix A) and maternal pain scale (Appendix B) 13 were used to evaluate the presence and quality or degree of nipple pain, rooting reflex, sucking pattern, and latch. Mothers were contacted again 2 weeks later through e-mail, mail, and/or telephone and asked to complete an identical survey (excluding previously collected demographic data) at that time. These survey data were analyzed to determine whether anatomical features of the infants noted on initial examination were correlated with the quality of breastfeeding as measured by the IBFAT. Mothers remained blinded of the newborn tongue examination at the time of this follow-up survey.
Data analysis
Demographic characteristics were reported as means and standard deviations (SDs) or n and percentage. Reliability was assessed with the κ statistic or the intraclass correlation coefficient, for categorical and continuous data, respectively. Univariate associations with IBFAT scores were evaluated using a linear model, either a regression analysis or a one-way analysis of variance (ANOVA), as appropriate to the independent variable. Associations with maternal pain scores were assessed with an ordinal logistic regression model, cumulating over the lower levels of pain scores, once it was determined that the proportional odds assumption of the ordinal model was met. Other outcomes used a linear model, either a linear regression or ANOVA, as suggested by the set of predictors. All analyses were carried out using SAS/STAT software, version 9.4 of the SAS System (Copyright © July, 2013; SAS Institute, Inc.) on a Windows 7 platform.
Results
Demographic characteristics
A total of 100 newborns were examined. Newborn subjects were 56% female. Birth weight ranged from 2,165 to 4,355 g. Average APGAR scores were 7.88 (range 1–9) at 1 minute and 8.92 (range 5–10) at 5 minutes. Complete initial survey data were available from 81 mothers (81% response rate). The 2-week follow-up survey was completed by 32 mothers (39.5% response rate). Although this follow-up survey response rate is comparable with typical expected response rates, the sample size was felt to be too small to draw significant conclusions. Thus, the results hereunder reflect responses to the initial surveys. The average maternal age was 30.4 years and 44% were primiparous. Of the multiparous group, mothers reported previous breastfeeding experience for one (25%), or two or more (12%) children. Of the 81 respondents on the initial survey, 62 intended to exclusively breastfeed, 8 mothers intended to exclusively bottle feed with formula, and 9 mothers intended to use both methods of feeding. Two mothers left this question blank. Maternal age, birth weight, change in weight from birth to discharge (measured as an absolute weight in grams and when recorded as a percentage of birth weight), and APGAR scores did not correlate with any measure of infant tongue anatomy (tip–frenulum length, visible cord, or palpable cord).
Distribution of tip–frenulum distance
The distribution of tip–frenulum lengths is displayed in Figure 2. Measured lengths ranged from 2 to 15 mm. Mean length from all measurements was 9.11 mm with a SD of 2.65 mm. Median length from all measurements was 10 mm. The 10th percentile for tip–frenulum length was 4.5 mm. The average difference between examiners in these measurements was 0.04 mm. Inter-rater reliability as measured by the intraclass correlation coefficient was 0.82 (95% confidence interval [CI] 0.74–0.87). The association between birth weight and tip–frenulum length was nonsignificant (r = 0.12, p = 0.23).
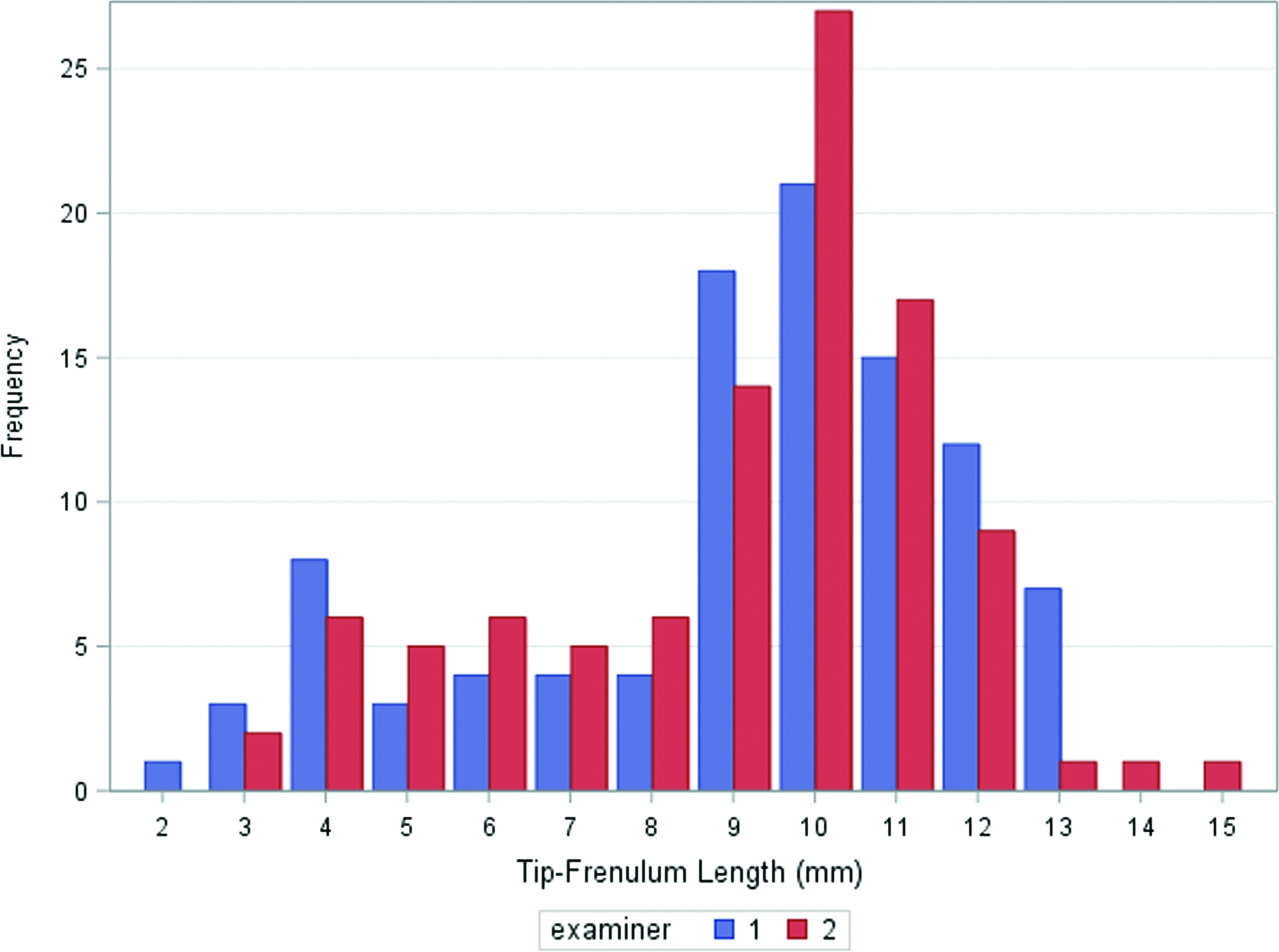
Distribution of newborn tip–frenulum distances. Color images available online at www.liebertpub.com/bfm
Visible and palpable cords
A visible cord was identified by one examiner in 21 of 100 (21%) subjects and by the second examiner in 20 of 100 (20%) subjects. Unweighted κ coefficient for visible cord was 0.91 (95% CI 0.81–1.0). Subjects with a visible cord identified by at least one examiner had a mean tip–frenulum length of 5.1 mm (95% CI 2.1–8.1 mm).
A palpable cord (which may or may not have been visible) was identified by one examiner in 59 of 100 (59%) subjects and by the second examiner in 44 of 100 (44%) subjects. Unweighted κ coefficient for palpable cord was 0.47 (95% CI 0.31–0.63). Subjects with a palpable cord identified by at least one examiner had a mean tip–frenulum length of 7.7 mm (95% CI 2.2–13.2 mm). When subjects with visible cords were excluded, the mean tip–frenulum length for the palpable cord group was 9.6 mm (95% CI 6.3–12.9 mm).
IBFAT scores
IBFAT results were scored from 0 to 3 for each question, for a total possible score of 12, with higher scores indicating more effective breastfeeding. In addition, an overall assessment of maternal satisfaction with breastfeeding was evaluated as “not pleased,” “fairly pleased,” “pleased,” or “very pleased.” In our cohort, IBFAT scores were positively correlated with maternal breastfeeding satisfaction (p < 0.0001). There was no association between birth weight and IBFAT scores (r = 0.06, p = 0.59).
In our study group, 54% of mothers had no previously breastfed children, whereas 46% had breastfeeding experience, from one (31%) to four (1%) prior children. When mothers were stratified by previous experience with breastfeeding, a positive correlation was identified between tip–frenulum length and IBFAT scores for mothers with two or more previous breastfed children. For mothers with less breastfeeding experience, no correlation was identified between tip–frenulum length and IBFAT scores (Fig. 3).
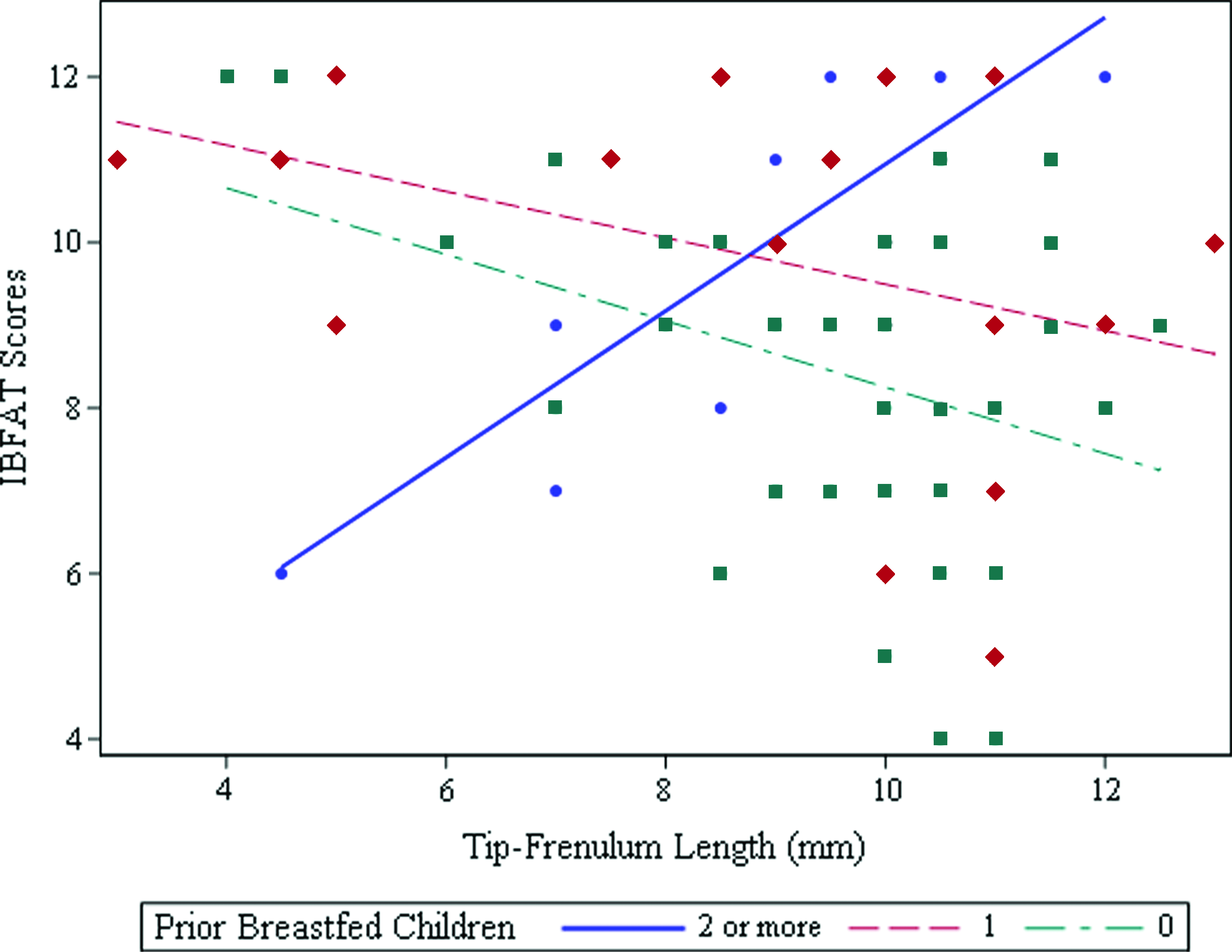
Effect of maternal breastfeeding experience on the relationship between tip–frenulum length and Infant Breastfeeding Assessment Tool (IBFAT) scores. Dots = 2 or more prior breastfed children; diamond shapes = 1 prior breastfed child; squares = no prior breasfed children. Color images available online at www.liebertpub.com/bfm
Pain scores
Figure 4 shows the effects of infant tongue anatomy on maternal pain scores. Tip–frenulum length was correlated with maternal pain scores (odds ratio [OR] 1.22, CI 0.99–1.51, p = 0.058). For each millimeter decrease in tip–frenulum length, mothers were 22% more likely to report nipple pain. The presence of a visible cord was also correlated with maternal pain scores, as mothers of infants with a visible cord were 3.65 times more likely to report pain (p < 0.05). The presence of a palpable cord also tended to result in higher maternal pain ratings, although this result was not statistically significant (p = 0.13).
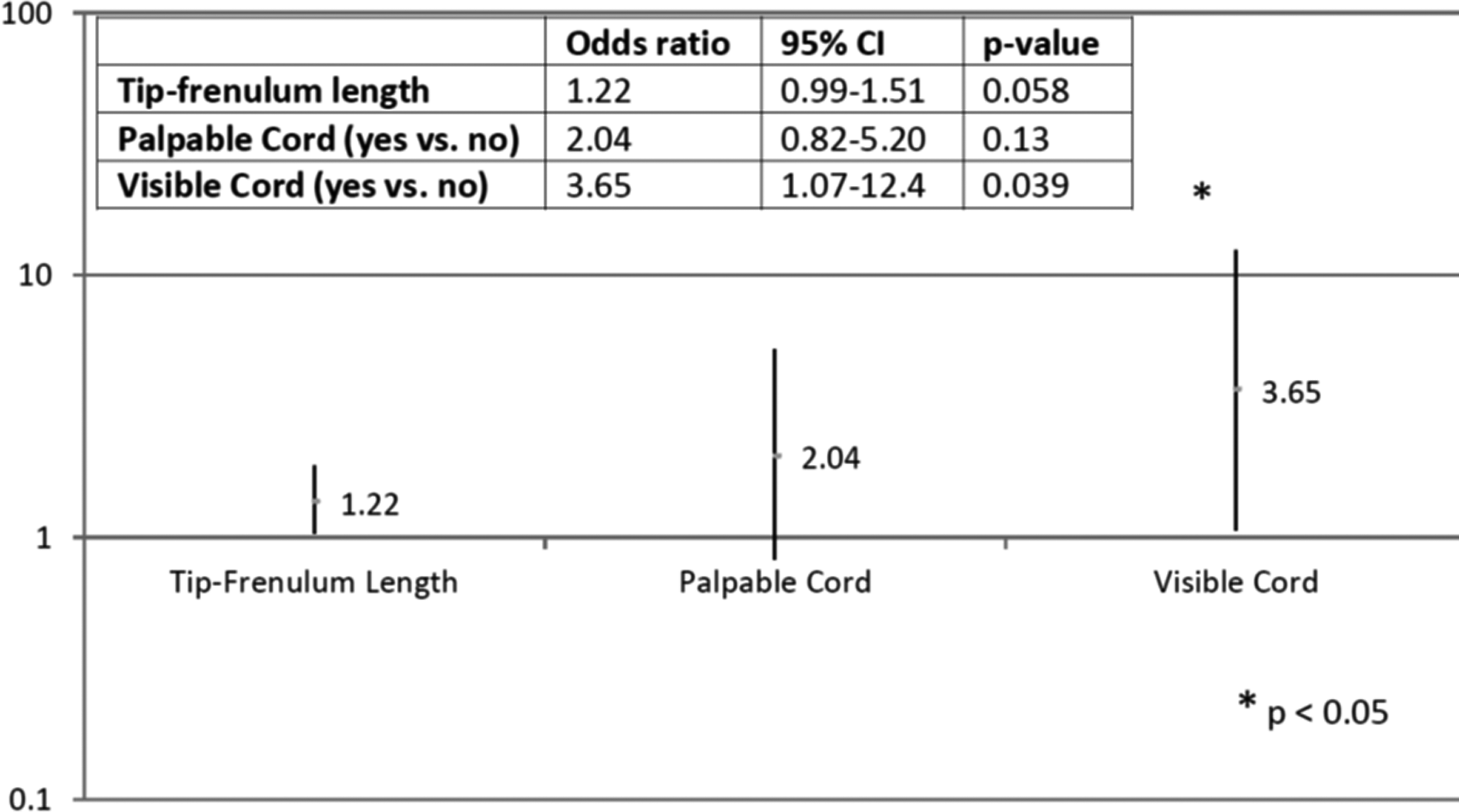
Odds ratios for higher maternal nipple pain. Values may not be directly comparable due to differences in continuous (length) versus categorical predictors. CI, confidence interval.
Discussion
This is the first study to use an objective measure of tip–frenulum distance as an adjunct for describing the degree of anatomical tongue tethering. The average tip–frenulum distance is between 9 and 10 mm, with 75% of subjects studied measuring >8 mm. We also found that shorter tip–frenulum distances were associated with greater experiences of maternal pain during breastfeeding. According to Schwartz et al., 14 for each day of maternal breast pain in the first 3 weeks of breastfeeding, there was a 10–26% chance of breastfeeding cessation. Tip–frenulum length may, therefore, be a helpful tool in identifying mother–newborn dyads at risk for early breastfeeding cessation.
Diagnostic criteria for ankyloglossia vary significantly, are inconsistently applied, and have only moderate inter-rater reliability. Including an objective measure of tongue anatomy with overall assessment of function and impact could aid clinicians in screening infants and making better clinical decisions regarding treatment. Several other authors15,16 have published measurements of the length of the lingual frenulum, but these studies involve older children after the development of the primary dentition, and many of the techniques require active participation from the subject. Measurements taken in awake newborns may be more challenging than for older children, but we have determined that the tip–frenulum technique is reliable and consistent between examiners, with little variability and a κ correlation coefficient as high as 0.82.
Haham et al. 17 studied tongue anatomy in a group of normal neonates, and found that presence of a lingual frenulum was nearly universal. In their study, frenulum grade (based on the Coryllos system) did not correlate with breastfeeding difficulty or a clinical diagnosis of ankyloglossia. This study is novel in finding an association between an objective measure of frenulum anatomy and a known predictor of breastfeeding cessation, maternal nipple pain.14,18
No significant differences in IBFAT scores were identified with respect to infant tip–frenulum length when considering the entire population of mothers. However, when mothers were stratified according to their level of previous breastfeeding experience, mothers with two or more previously breastfed children reported a positive correlation between tip–frenulum length and IBFAT scores (Fig. 3). One explanation of this finding is that inexperienced mothers face a variety of challenges to breastfeeding that may overshadow the effect of tongue anatomy. In contrast, more experienced mothers, for whom the other factors may have been resolved when breastfeeding older siblings, more readily notice the impact of a short frenulum on their ability to comfortably breastfeed. This indicates that although a first-time mother may need more lactation assistance before determining a treatment course for a short tongue/tongue tie, a plan may be able to be more rapidly engaged with a mother with more experience.
More recently, a distinction has been made between anterior and posterior ankyloglossia.7,8,17,19–21 Posterior ankyloglossia has been identified in some infants with feeding difficulties and is described as a “thick, fibrous cord posterior to the ventral tongue mucosa… obscured by the ‘mucosal curtain’” 8 or “when the lingual frenulum was not very prominent on inspection but was thought to be tight on manual palpation or was found to be abnormally prominent, short, thick, or fibrous cord-like with the use of the grooved director.” 7 Frenotomy has been advocated for treatment of patients with a suspected posterior ankyloglossia, with variable and subjective results.7,8,20–22 Our data suggest that the presence of a visual cord carries a high degree of inter-rater reliability (κ = 0.91), 7 but inter-rater reliability for a palpable cord was substantially lower (κ = 0.47). This suggests that the diagnosis of posterior ankyloglossia by palpation of a thick, fibrous posterior cord as described in the literature may suffer from high interobserver variability, and should be interpreted with caution, particularly when considering surgical intervention.
The results of this study are interpreted within a small sample size of otherwise healthy newborns in one hospital in the United States. Whether these data can be extrapolated to older infants in other populations is yet to be determined. Because of the small sample size, it is possible that our normal distribution is actually bimodal, and further research will be necessary to determine this. Nevertheless, we did not perform post hoc sample size calculations, as these types of calculations have been shown to be methodologically flawed. 23 The assessments of breastfeeding are reliant on survey responses by mothers and, as such, are subjective. However, mothers were blinded to the results of the oral cavity examination in an attempt to limit bias.
Our objective in this study was to better define the anatomy of the infant tongue and lingual frenulum, and no clinical diagnosis of ankyloglossia was made. Breastfeeding is a complex interaction involving the mother–infant dyad with countless variables to predict its effectiveness. We present normative data in this study to guide clinicians in what should be a global assessment of tongue anatomy and physiology. Hopefully, this information will lead to a better understanding of the overall relationship of this anatomy with the physiology of infant feeding and the pathophysiology of ankyloglossia.
Conclusions
In our study, the newborn tongue tip–frenulum distance averaged ∼9 mm, with a SD of 2.5 mm. Shorter tip–frenulum length was correlated with higher maternal nipple pain scores. A large percentage (up to 59%) of otherwise normal newborns have a prominent palpable cord upon palpation of the ventral tongue in the region of the lingual frenulum. Further studies should be directed at investigating other diagnostic criteria to define clinically significant posterior ankyloglossia, and whether treatment with frenotomy can result in improved breastfeeding in these patients.
Footnotes
Acknowledgments
The authors sincerely thank Dr. Sema Hart for assistance in data collection; Drs. Shawn Newlands, Michael Cunningham, and Reza Rahbar for invaluable guidance in proof reading this article; and Ryan F. Healey for his artistic contribution.
Disclosure Statement
The authors have no disclosures to report.