
Abstract

W
The U.S. Department of Agriculture's Food and Nutrition Service (FNS) administers 15 federal nutrition assistance programs, including the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). Established as a permanent program in 1974, WIC safeguards the health of low-income women, infants, and children by providing them access to nutritious foods, nutrition education, and breastfeeding support and referrals to various health and social services. Nearly 7.7 million women, infants, and children participated in the WIC in 2016, 1 and more than half of the infants in the United States are served by WIC 2 through clinics located throughout the country.
We were invited here today to present findings from the WIC Infant and Toddler Feeding Practices Study-2 (WIC ITFPS-2), also known as the Feeding My Baby Study. WIC ITFPS-2 is a large longitudinal study of infants and their caregivers enrolled in WIC during late pregnancy or early infancy. The study addresses a series of research questions regarding feeding practices, the association of WIC services with those practices, and the health and nutrition outcomes of children receiving WIC benefits.
While we have been asked to present these findings to you, we cannot take full credit for this important study. We want to recognize the important contributions of Patricia MacNeil who is the FNS WIC Division study liaison. We also want to acknowledge Anne Bartholomew, Chief of the Nutrition Services Branch at WIC, who is here with us today. We further acknowledge the study's Project Director from Westat, Nancy Weinfield, as well as the entire Westat team conducting the study; the study's Principal Investigator, Shannon Whaley, co-Principal Investigator, Lorrene Ritchie, and Linnea Sallack from Altarum. Finally, we acknowledge the entire FNS research team, both current and former. All contributors have dedicated their time and expertise to make this a successful study. A list of the entire research team is found at the end of this article.
WIC ITFPS-2 is a sentinel study in the WIC research community not only because it enrolled thousands of children at the beginning of the study but also because it intends to follow these children until they turn 5 years old, regardless of whether they continue to receive WIC benefits. The study provides insight into the breastfeeding patterns, dietary intakes, and health status of a national sample of WIC participants, which is something that has not been studied for about 20 years. The last time FNS conducted a study like this was in the mid-1990s with the WIC Infant Feeding Practices Study-1 (WIC IFPS-1), but in that study, the infants were followed only until their first birthday. The current study goes beyond that and our hope is that this study will provide us with insight into the longer term nutrition and health benefits of WIC.
Given its longitudinal nature, WIC ITFPS-2 will produce a series of reports. Its first report, the Intentions to Breastfeed Report, 3 focused on results from a prenatal survey and was released in June 2015. This article will focus on the information published in the second report, the Infant Year Report, 4 which was released in January 2017. This Infant Year Report is based on information gathered from prenatal interviews and from interviews conducted during the infant's first year of life. The findings focus on breastfeeding intention, initiation, and duration and the introduction of complementary foods. Additionally, the report compares infant feeding practices and perceptions between the current longitudinal study and WIC IFPS-1 conducted 20 years ago. Because these two studies had very similar methodologies, we are able to compare these results.
Study Design
WIC ITFPS-2 is a longitudinal study that includes a nationally representative sample of infants enrolled in WIC. The study follows children for the duration of the WIC eligibility period, until they turn 5 years of age, regardless of whether they continue to participate in WIC. Between July and November 2013, caregivers of infants in this cohort were enrolled in the study at 80 local WIC sites, which represented 27 WIC State agencies. Caregivers were eligible for enrollment as long as they met certain criteria: (1) pregnant or had an infant less than 2.5 months old; (2) first time enrolling in WIC for this pregnancy or child; (3) at least 16 years old; and (4) English or Spanish speaking. Based on these criteria, 4,367 caregivers were enrolled in the study, representing 80% of infants who were recruited based on eligibility. For the Infant Year Report, caregivers were included if they completed a 1- or 3-month postpartum interview, thus this report included findings from 3,777 caregivers.
There were several different data sources for the Infant Year Report. The study team conducted site visits and surveyed WIC staff working at the local sites. The study team also conducted key informant interviews with state and local agency staff. These surveys and interviews were conducted to shed light on some of the characteristics of the WIC clinics and their staff. The study team also gathered participant-level data through an initial in-person survey with the caregivers or mothers of the infants, and these initial in-person interviews were followed by telephone interviews that occurred as frequently as every 2 months for the first year of life. During these interviews, we were able to gather information on breastfeeding initiation and duration, the introduction of complementary foods, and caregiver's perceptions of WIC services. While this information was collected through self-report and introduces the potential for reporting bias, a major strength of the study design is that the recall period was short. The study also used administrative data to collect information already collected during WIC clinic visits—such as infant length and weight. For infants who were no longer receiving WIC, the team attempted to collect anthropometric data through the infant's healthcare provider. The study methodology and interview schedule are detailed elsewhere. 4
To help guide the analyses on breastfeeding beliefs and intentions, the study's research team and Peer Advisory Panel developed a conceptual model of infant feeding practices as shown in Figure 1. 5 This conceptual model, which incorporates theory and findings from the literature, hypothesizes that prenatal maternal beliefs, along with current advice, experiences, and maternal health, influence intentions to breastfeed and, in turn, breastfeeding initiation.
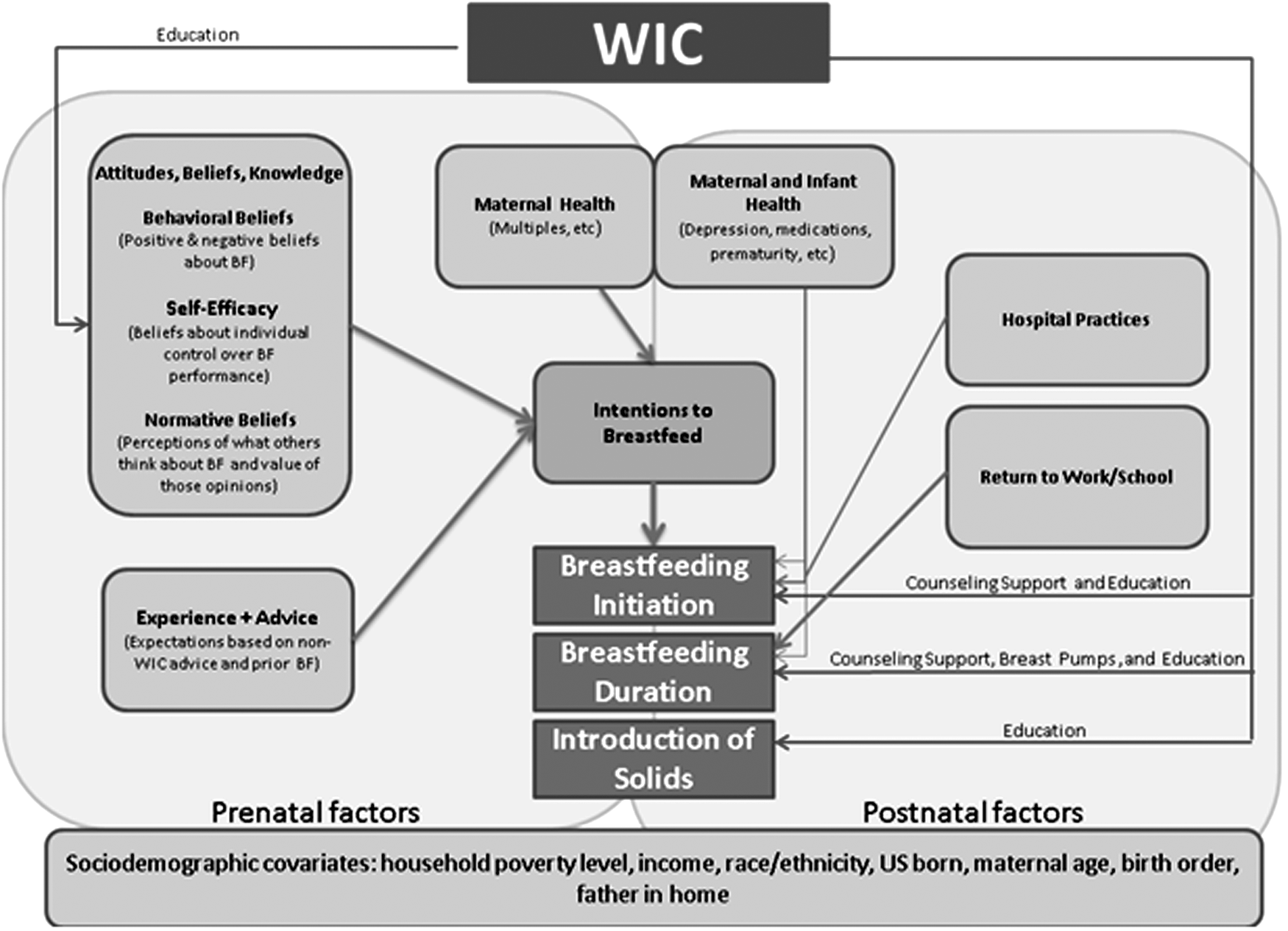
Infant feeding practices conceptual model by Harrison et al. 5 WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Analyses were performed using SAS 9.3 (SAS Institute, Inc., Cary, NC). Descriptive statistics (e.g., counts, proportions, means, medians, and cross-tabulations) were applied when examining outcomes by subgroups of interest. Unless otherwise specified, all results are weighted to produce nationally representative estimates; all significance testing was performed at a level of p ≤ 0.05.
Study Results
Demographic characteristics of study sample (unweighted)
Among the 3,777 caregivers who completed a 1- or 3-month interview, 59% identified as white and 26% as African American or black. The remaining 15% identified as a race other than white or African American or black. Thirty-eight percent of the study participants identified as Hispanic or Latino. Almost half (47%) of the caregivers enrolled in the study were 26 years or older, while about 41% were 20–25 years, and 12% were 16–19 years. Additionally, 41% of caregivers were having their first child, while about 27% were having their second, and 32% were having their third child.
Caregiver perceptions of breastfeeding
Caregiver perceptions regarding the benefits of breastfeeding differ from what was reported 20 years ago in the WIC IFPS-1. Overall, higher percentages of women agree with the statements on benefits. For example, in the mid-1990s, 61% of caregivers agreed with the statement “Breastfed babies are healthier than formula-fed babies.” In the current study, 80% agreed with this statement. The responses by women of all racial and ethnic subgroups were uniformly more positive in the current study than they were nearly 20 years ago.
The percentage of caregivers who agreed with perceived barriers to breastfeeding also has changed since the 1990s. For example, 20 years ago, 41% of caregivers agreed with the statement that breastfeeding ties a mother down and 34% agreed that breastfeeding takes too much time. In the current study, less than 20% of prenatal women agreed with these statements. The study also found a more than 20 percentage point difference in comfort with breastfeeding in public—20 years ago, 61% of mothers agreed that breastfeeding in public was not something they wanted to do, but this response dropped to 37% in the current study. Nonetheless, a few issues still remain challenging. For example, more than 50% of women agreed that breastfeeding means no one else can feed your baby and that with bottle feeding, the mother knows the baby is getting enough to eat.
Breastfeeding practices
Some of the most noteworthy findings from the Infant Year Report involve breastfeeding initiation and duration. In the current study, 83% of mothers initiated breastfeeding, compared with 56% in the WIC IFPS-1 conducted during 1994 and 1995 (Fig. 2). The percentage of women participating in WIC who continue to breastfeed (exclusively or in combination with formula) also has risen notably since WIC IFPS-1. At 1 month postpartum, the percent of breastfeeding mothers increased from 33% in the mid-1990s to 61% in 2014. Between 3 and 12 months postpartum, the breastfeeding rates have more than doubled since the earlier study. The important breastfeeding support efforts of WIC, such as the WIC peer breastfeeding counseling program, in combination with the breastfeeding support and protection efforts of so many other government and nongovernment agencies, have likely contributed to the higher breastfeeding rates among women enrolled in WIC. However, the news is not all positive. You will also note the similar slopes in trend lines, suggesting that despite the increase in breastfeeding initiation and duration, the drop-off rate has not changed substantially over the past 20 years, and the drop-off is greater than what we see in national data released by Centers for Disease Control and Prevention. 6 While important progress has been made in increasing breastfeeding, the majority of mothers continue to stop breastfeeding earlier than recommended. 7
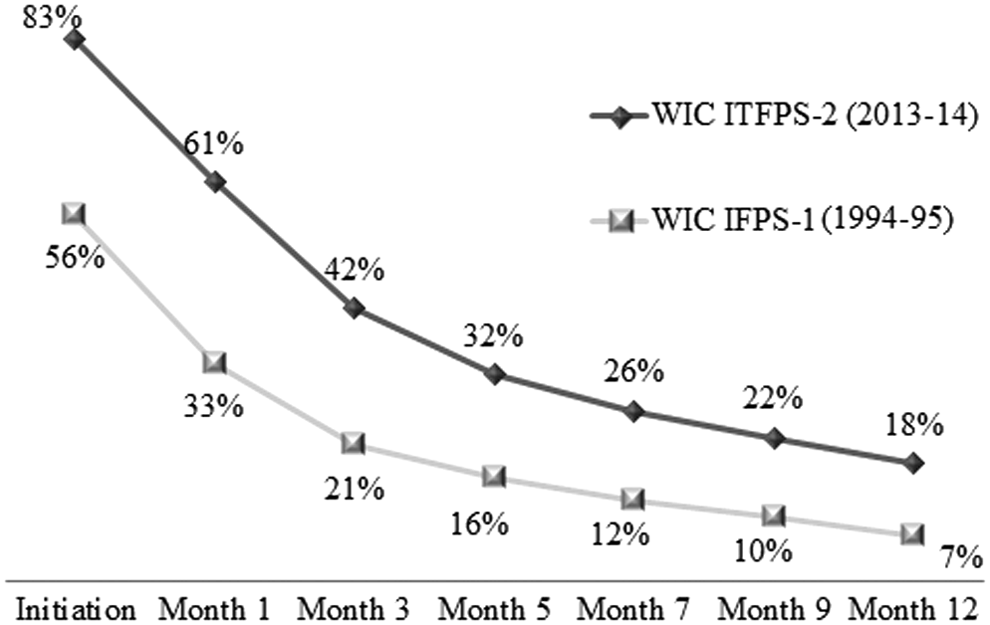
Breastfeeding rates by age of infant: 2013–2014 compared with 1994–1995. WIC IFPS-1, Infant Feeding Practices Study-1; WIC ITFPS-2, Infant and Toddler Feeding Practices Study-2.
We know that mothers are also discontinuing breastfeeding earlier than they intend. At the 1-month interview, mothers were asked how long they intended to breastfeed. The majority (73%) of WIC ITFPS-2 breastfeeding mothers reported that they planned to breastfeed for more than 6 months. However, follow-up inquires revealed that regardless of how long the mother intended to breastfeed, ∼70% of mothers did not achieve their own personal breastfeeding duration goals. These findings are similar to what was reported in a national study that found 60% of mothers reported not breastfeeding as long as they wanted. 8 Additionally, these findings underscore the importance of continued breastfeeding support for mothers from all sources—family, health and child care providers, employers, and the communities in which they live.
As breastfeeding rates have increased among women enrolled in WIC, racial disparities in breastfeeding have narrowed. In WIC IFPS-1 from the mid-1990s, 34% of African American mothers and 53% of white mothers initiated breastfeeding, a difference of nearly 20% points. The current study revealed that 74% of African American women and 84% of white women enrolled in WIC initiated breastfeeding, reducing the disparity to 10% points. While continued efforts are needed to address disparities in breastfeeding, these findings are encouraging.
Reasons for breastfeeding cessation
As noted earlier, more than one-half of the mothers who started breastfeeding had discontinued any breastfeeding by 3 months. The top three reasons for breastfeeding cessation around 3 months postpartum reported by mothers enrolled in WIC ITFPS-2 were breast milk alone did not satisfy the baby (57%), inability to produce enough breast milk (56%), and the baby lost interest in nursing (34%). These top reasons exhibit very few significant associations with key sociodemographic variables, indicating that the top reasons are the same for most women regardless of circumstance or characteristics. It should also be noted that these reasons are also reported in other national studies,8,9 so these reasons are not exclusive to the WIC population.
The implications of these findings are that mothers' perceptions of breast milk adequacy and baby's interest in breastfeeding may lead to the cessation of breastfeeding and, in turn, lower breastfeeding rates. As such, these topics could be areas on which WIC peer counselors and pediatric care providers could provide additional support to breastfeeding mothers.
Complementary feeding
Complementary feeding is defined as the period when liquids, semisolids, and solids are provided to infants and young children to complement the milk feeding. The WIC infant food packages and accompanying education on the introduction of complementary foods are aligned with American Academy of Pediatrics' recommendations 7 to introduce complementary foods at about 6 months of age. For the current study, early introduction of complementary foods was defined as the introduction of foods before age 4 months because at the time of data collection, there was still inconsistency in recommendations on timing of complementary foods and many practitioners were still recommending introduction between 4 and 6 months of age.
Twenty years ago, the WIC IFPS-1 estimated that ∼60% of caregivers started serving complementary foods before 4 months. In the current study, 20% of caregivers reported introducing complementary foods before 4 months of age. In addition, WIC ITFPS-2 caregivers introduced foods from key food groups (baby cereals, fruits, vegetables, and meats) at least 1 month later than observed in WIC IFPS-1. For example, infant cereals are being introduced 41 days later than they were 20 years ago. These are encouraging findings because it shows a trend of infant feeding that is more aligned with current recommendations and with the current WIC infant food packages.
Perceptions of the WIC services
To gauge caregivers' perceptions of the WIC, they were asked about their experiences with the program and the support they received while breastfeeding and providing complementary foods to their infants. Among mothers who breastfed, more than 95% reported that their WIC site played a somewhat important or very important role in their decision to breastfeed their infant. This speaks to the importance of the breastfeeding support and nutrition education provided to mothers through WIC peer counselors and other staff members.
In addition to providing nutrition education on infant feeding, WIC provides food packages that are specifically designed to meet the nutritional needs of mothers and infants. For example, Food Package VII, the food package distributed to fully breastfeeding mothers, is tailored to the nutritional requirements of mothers who are breastfeeding. This food package is often referred to as the enhanced food package because it includes additional foods that help meet breastfeeding mothers' needs.
In the current study, the vast majority of breastfeeding mothers (91%) knew about the enhanced food package at 3 months postpartum. Among those who were aware of the package, 61% stated that this enhanced food package played an important role in their breastfeeding decision. Additionally, the enhanced food package also appears to be associated with longer breastfeeding durations as those moms who were aware of the food package also breastfed for 1.5 months longer than those who were not aware of the food package.
WIC food packages, such as the enhanced food package, are not the only benefit provided to participants; participants also benefit from the nutrition education provided by the program. When mothers were queried about where they obtain information on infant feeding at 5 months, nearly 60% of study mothers reported that they turned to their WIC office or clinic for this information. WIC sites were second only to doctors and other health professionals as a source of feeding information, and the support that WIC provides does not have to take place in the clinic. In some cases, WIC staff will make support calls to mothers, and our study found that mothers who receive these support calls were more likely to be exclusively breastfeeding at 1 month than those who did not receive the support calls.
Caregivers also reported making positive changes in how they feed their families or themselves as a result of WIC nutrition education. At both 3 and 13 months, ∼60% reported having made such positive changes, and most of these changes involved making better dietary choices. For example, 34% of mothers reported that because of WIC, they now know how to choose more healthy foods for themselves and their families. In addition, about 27% reported that they consume more fruits and vegetables because of the nutrition education they received through WIC.
Summary
In summary, key findings of the Infant Year Report of WIC ITFPS-2 include the following:
1. Breastfeeding initiation rates among women enrolled in WIC have risen over the past 20 years. The percentage of women who initiated breastfeeding in 2013–2014 is one and one-half times higher than it was in the mid-1990s when the first WIC IFPS-1 was performed. As breastfeeding increased, racial disparities in breastfeeding initiation narrowed from 19% points to 10% points. 2. The decline in breastfeeding over the first year postpartum is similar to the decline observed 20 years ago. Between 3 and 12 months, the current study demonstrated that breastfeeding rates were double the rates observed in the mid-1990s; however, there was still a progressive decrease in breastfeeding rates as infants approached their first birthday. Additionally, 70% of mothers in the current study did not breastfeed as long as they had intended. 3. Early introduction of complementary foods is much less prevalent among WIC participants than before. Data from the previous study showed that almost 60% of caregivers were introducing complementary foods to their children before they turned 4 months old, but now that number is down to only 20%. 4. Caregivers credited WIC with making positive changes in how they fed their infants and themselves. More than 95% of study caregivers who initiated breastfeeding said that WIC played an important role in their decision to breastfeed. 5. WIC participants received extensive support from WIC. Nearly 60% of caregivers reported that they have turned to WIC for information on feeding their infant, second only to their pediatric provider.
Footnotes
Acknowledgments
The authors would like to recognize the contributions of the following individuals who have provided valuable input on WIC ITFPS-2. Westat: Nancy Weinfield, Crystal MacAllum, Laurie May, Christine Borger, Jill DeMatteis, Jacque Wernimont, Beth Mittl, and Susie McNutt; Public Health Foundation Enterprises: Shannon Whaley; University of California Nutrition Policy Institute: Lorrene Ritchie; Altarum Institute: Linnea Sallack; and USDA Food and Nutrition Service: Jay Hirschman, Melissa Abelev, Renee Arroyo-Lee Sing, Anne Bartholomew, Patricia MacNeil, Valery Soto, and Lisa Southworth.
Disclosure Statement
No competing financial interests exist.