
Abstract
Abstract
Background and Objectives:
To promote exclusive breastfeeding, supplements are not recommended without medical indications such as clinical evidence of dehydration. Loss of ≥10% of birth weight (BW) often triggers supplementation due to nursery staff's concern for dehydration. Studies have demonstrated that transplacental passage of maternal intrapartum intravenous fluids for anesthesia may inflate BW. Researchers have proposed using newborn's 24-hour weight (24HW), after fluid diuresis, as preferred reference for weight loss calculation. The mother–infant unit at Hartford Hospital, a Baby-Friendly Hospital, implemented this recommendation into routine practice in March 2014. This study was conducted to evaluate this practice change's safety and effectiveness in decreasing supplementation.
Methods:
We performed a retrospective chart review on healthy full-term newborns delivered by C-section in 12 months before (n = 404) and a 12-month period after (n = 263) incorporating the 24HW into routine practice. Overall supplementation rate, maximum weight loss, length of stay (LoS), and peak transcutaneous bilirubin (TcB) were compared.
Results:
Overall supplementation rate decreased from 43.6% pre- to 27.4% postintervention and in first-time mothers from 51.9% to 31.0%. Among infants losing ≥10% of BW, the supplementation rate decreased from 63.9% to 26.2%. There was no significant increase in maximum weight loss, peak TcB level, or LoS overall or in those with ≥10% weight loss from birth.
Conclusion:
Routine use of 24HW as the reference for newborn weight loss calculation reduced supplementation and did not increase untoward effects during the hospital stay.
Introduction
I
Dehydration is considered a medical indication for supplementation if based not only on neonatal weight loss but also on the presence of clinical signs such as dry mucus membranes, sunken fontanelle, tenting, decreased urine output, and abnormal blood chemistries. In the nursery, newborns are routinely weighed on the night shift, and a weight loss of ≥10% from birth frequently triggers concern of mother and nursery staff for insufficient intake of breast milk and dehydration. This may lead to supplementation when other signs of dehydration are absent or not assessed. Studies have shown that the transfer of maternal intrapartum fluid may augment the infant's birth weight (BW).11,12 Diuresis of this fluid by the infant occurs largely in the first 24 hours of life.13–15 Some researchers have recommended using the 24-hour weight (24HW) instead of BW as the reference in calculating percentage weight loss for infants whose mothers received fluid during labor.13,16 The mother–infant unit at Hartford Hospital, a designated Baby-Friendly Hospital since 2000, adopted this recommendation in March 2014, as a potential means to decrease unnecessary supplementation of breastfeeding infants.
Materials and Methods
Study design
We performed a retrospective chart review of breastfeeding infants born by C-sections before and after the implementation of the 24HW measurement into routine practice. The study excluded vaginal births as these infants are typically discharged 2 days after birth, whereas following C-section births, infants usually stay 3–4 days allowing for a longer monitoring period. All data were collected after discharge, and informed consent was waived. Patients were identified using the Women's Health perinatal dataset.
Outcome measures
We compared the supplementation rate during the hospital stay for infants born 1 year before and 1 year after implementation of the practice change. Subgroup analyses were performed for infants of primiparous and multiparous mothers. Three potential untoward outcomes during the hospital stay were assessed: infant's maximum percentage weight loss from BW, length of stay (LoS), and hyperbilirubinemia determined by peak transcutaneous bilirubin (TcB). Routine bilirubin screening is performed on all newborns at Hartford Hospital around 48 hours or for concern for jaundice.
Study period and subjects
Preintervention data were collected from January 1, 2013 to December 31, 2013 and postintervention from June 1, 2014 to May 31, 2015, allowing for a 2-month washout period after start of the implementation on March 25, 2014. Newborns of mothers who planned to breastfeed were included in the study if they met the following criteria: full term (390/7–416/7 weeks), appropriate for gestational age, singletons, delivered by Caesarean section with an Apgar score ≥8 at 5 minutes, did not require Neonatal Intensive Care Unit (NICU) transfer, and no formula supplements were received in the first 24 hours of life (Fig. 1). Twenty-three newborns in the postintervention group were excluded, as no 24HW was documented at the time when the chart was still lacking a specific place for recording it. The final study sample was 404 preintervention and 263 postintervention subjects.
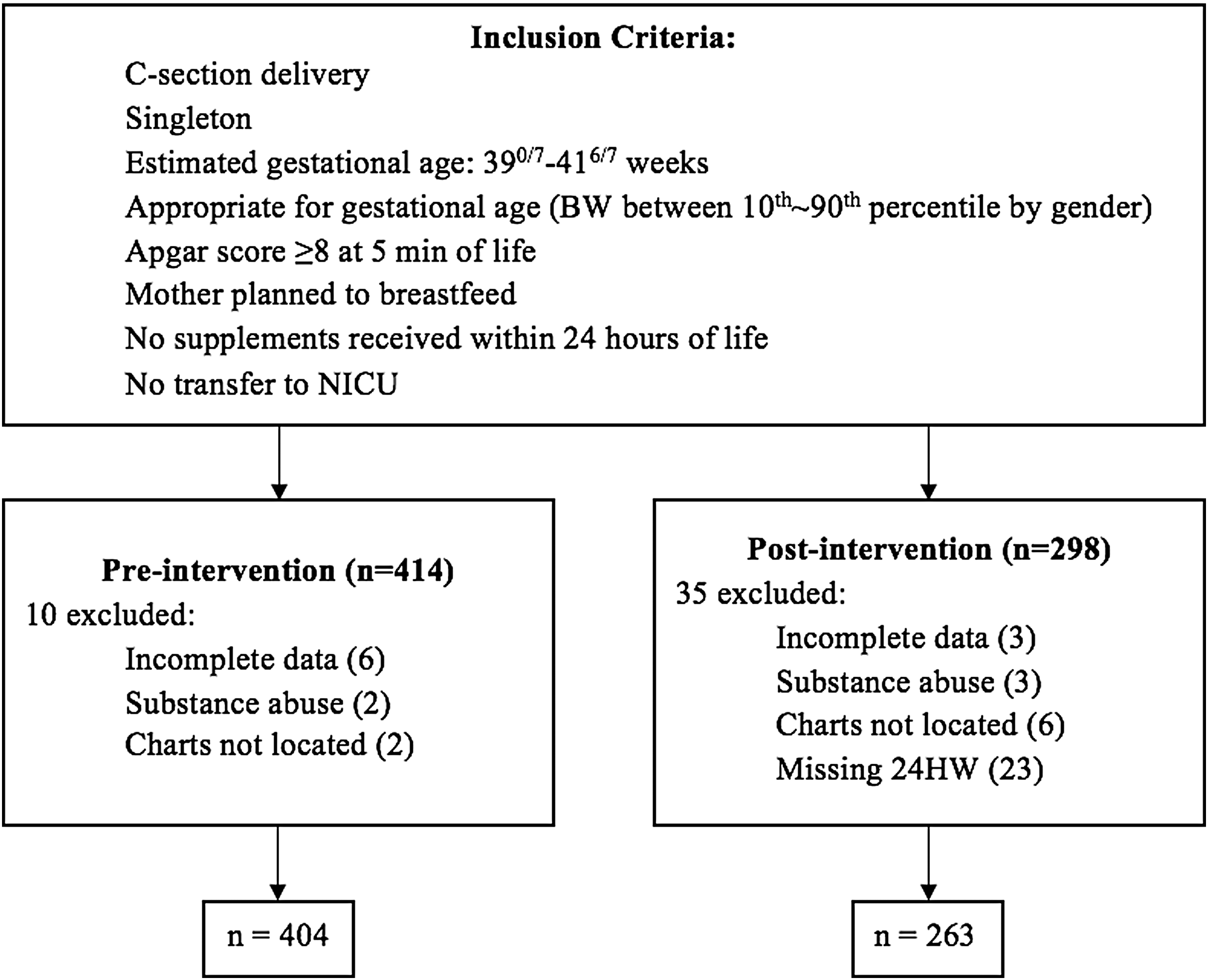
Inclusion criteria and study sample. BW, birth weight; 24HW, 24-hour weight; NICU, Neonatal Intensive Care Unit.
Maternal data included age, parity, previous breastfeeding experience, insurance status, C-section type (planned or unplanned), length of labor, and volume of fluid received. Infant data included BW, 24HW (for the postintervention group only), number of voids and feeds in the first 24 hours of life, lowest weight achieved, maximum TcB level, LoS, and whether the baby was ever supplemented with formula during the hospital stay.
Weight measurement
All infants were routinely weighed at birth using Scale-Tronix® Pediatric Scales 4802D (accurate to the nearest 1 g). The intervention required that nurses obtain the weight of all infants at 24(±1) hours of life. Subsequent daily weights were obtained per nursery routine on the evening shift. Nurses and providers were educated about the scientific evidence behind the 24HW and instructed to routinely consider this weight as baseline for subsequent weight loss calculation and assessment of feeding adequacy before initiating supplements based on BW alone. Before weighing infants, nurses were encouraged to counsel mothers that the infant weight loss in the first 24 hours was largely due to diuresis of intrapartum fluids and that the 24HW would serve as baseline for further weight loss. Nurses' feedback on how to integrate the practice change into their workflow resulted in clustering measurement of 24HW with the critical congenital heart disease screening mandated by the State of Connecticut. The infant flow sheet was revised to include a specific place to document 24HW, allowing for easy comparison with BW and daily weight. Subsequent daily weights were obtained as per routine on the night shift.
Statistical analyses
Group sample sizes of 194 preintervention (assuming a proportion of 0.4 infants supplemented with formula in this cohort) and 127 in postintervention (assuming a proportion of 0.25 infants supplemented with formula) achieve 80% power to detect a difference between the pre- and postintervention group proportions of 0.15. The test statistic used is a two-sided Z test with pooled variance. The larger sample sizes in the project (404 preintervention and 263 postintervention) allowed for subgroup analysis with sufficient power.
A significance level of 0.05 was used for all statistical tests. Chi-square and Fisher's exact tests were used to compare discrete variables and independent sample t-tests to compare continuous variables between groups.
Results
Demographics
There was no statistically significant difference between the two groups of subjects in terms of maternal ethnicity, insurance status and age, infant gender ratio, estimated gestational age, Apgar score at 5 minutes of life, BW, percentage delivered with labor, and the number of voids and feeds in the first 24 hours of life (Table 1).
p-Value generated from chi-square test.
p-Value generated from independent t-test.
EGA, estimated gestational age; BW, birth weight; SD, standard deviation.
Supplementation
In the postintervention group, 27.4% of infants were supplemented, in comparison with 43.6% preintervention (p < 0.001; Table 2). Among primiparous mothers, the proportion of infants supplemented fell from 51.9% to 31.0% after the intervention (p < 0.001), whereas, in infants of multiparous mothers, the proportion supplemented showed a smaller but still significant decrease from 36.8% to 24.5% (p = 0.017).
p-Values generated from Fisher's exact tests.
p < 0.001.
p < 0.05.
Among infants losing ≥8% of BW (a cutoff for clinical intervention recommended by the AAP 1 ), the supplementation rate dropped from 49.6% to 26.2% (p < 0.001) after the practice change. When a cutoff point of ≥10% weight loss from BW (commonly known as the “rule of thumb”) was used, 64% were supplemented preintervention compared with only 26% preintervention (p < 0.001).
Infant weight loss
Comparison between the pre- and postintervention group showed no significant difference in the distribution (p = 0.053; Table 3) or mean maximum percentage weight loss (p = 0.309; Table 4). No infant in either group experienced clinical dehydration requiring transfer to the neonatal intensive care unit during the hospitalization.
p-Values generated from chi-square tests.
24HW, 24-hour weight.
p-Values generated from chi-square tests.
p-Values generated from independent t-tests.
p < 0.01.
TcB, transcutaneous bilirubin.
TcB level and LoS
There was no significant difference between the two groups in mean peak TcB attained or the proportion of infants with a level ≥15 mg/dL (phototherapy level per AAP guidelines 17 for full-term low-risk infants at 48 hours or high intermediate risk zone at 72 hours of life per the Bhutani nomogram 18 ). There was a small decrease in mean LoS after the intervention from 3.6 to 3.5 days (p = 0.004). Notably, there was no significant difference in mean peak TcB or LoS pre- and postintervention for infants who lost ≥8% or ≥10% BW.
Weight loss at 24 hours (postintervention group only)
On average, infants lost 5.3% (standard deviation = 1.4%) of their BW in the first 24 hours with a range of 1.2–11.5%.
Those experiencing labor lost less weight (4.8% versus 5.5%; p < 0.001), had fewer voids (2.7 versus 3.8, p < 0.001), and fed less frequently (6.4 times versus 7.4 times, p < 0.001) in the first 24 hours of life, and their mothers received less fluid compared with those without labor. There was no statistical difference in their maximum weight loss during the hospital stay that occurred typically on day 2 or 3 of life (Table 5).
Of the 263 postintervention infants, 20 did not have length of labor recorded and were thus excluded from this analysis.
p-Values generated from independent t-tests.
p < 0.05.
p < 0.01.
p < 0.001.
Discussion
This study demonstrates a reduction in supplementation of healthy term infants delivered by Cesarean sections after incorporating simple practice changes into routine care: namely measurement of 24HW and utilization of this weight rather than BW as baseline for calculation of neonatal weight loss, education of nurses, lactation consultants and providers, and counseling of parents on the effect of intrapartum fluid transfer on their infants' weight and the utility of 24HW.
The overall supplementation rate decreased from 43.6% to 27.4% after implementation of the intervention. Although the proportion of supplemented infants of multiparous mothers dropped significantly (36.8% to 24.5%), the effect was most dramatic (51.9% to 31.0%) in infants of primiparous mothers. Primiparous mothers experience greater anxiety about breastfeeding and are more likely to perceive an insufficient milk supply and request supplementation for their infants when notified of weight loss by nurses during routine weighing on the night shift. Education of staff and mothers about the effect of intrapartum fluids on BW and use of the 24HW as reference point for calculating weight loss may have alleviated some anxiety and reduced unnecessary supplementation. It is also possible that first-time mothers are more receptive to this information than multiparous women, who are less likely to change their feeding practices due to prior experience.
The high percentage of neonates losing ≥8% and ≥10% BW in both pre- and postintervention groups in our study is consistent with the study of Flaherman et al. on weight loss in infants delivered by C-sections. 19 Our study found a dramatic reduction in supplementation of infants losing ≥8% BW (26.2% versus 49.6%) and ≥10% BW (26% versus 64%) after the intervention (Table 2). Thus, utilization of 24HW rather than BW as the baseline for estimation of infant weight loss may have prevented a rush to supplement. Since increased infant weight loss is common after C-sections, it is important that decisions to supplement these infants are not based on percentage weight loss from birth alone, but on clinical assessment of feeding and dehydration.
Only 5 of the 263 infants (2%) in the postintervention group lost ≥8% of 24HW (only 1 was supplemented) and none lost ≥10%. The low frequency of ≥8% weight loss from 24HW suggests the need for close monitoring, assessment, and possible intervention in infants reaching this level of weight loss.
It was important to consider potential untoward effects of the intervention. Statistical analyses showed that the mean and distribution of maximum percentage weight loss from BW did not differ significantly between the pre- and postintervention groups, despite less supplementation in the latter. However, the reduced supplementation rate in the postintervention group may explain a small increase in the proportion of infants losing ≥10% of BW (31.9% versus 24.0%). Since any infant with clinical concerns for dehydration would have received medically indicated supplementation, this finding may indicate a decreased tendency to supplement based on weight criteria alone.
There was no significant difference in hyperbilirubinemia between the two groups as measured by mean peak TcB level or percentage of infants with a level ≥15 mg/dL. The small but statistically significant shorter LoS in the postintervention group was possibly due to our institution's trend toward discharging mothers on the third rather than fourth day post-C-section, if doing well, and it is the mother's preference. It is reassuring that among infants who lost ≥8 or 10% BW, there were no significant differences in the three potential negative outcomes studied even though the supplementation rate was dramatically reduced postintervention.
The strength of this study is its large sample size and original nature. To our knowledge, using 24HW as the reference for weight loss calculation has surfaced in the literature only as a recommendation.13,16 This study is the first to report its implementation into routine care in a Level 1 nursery and to demonstrate reduced in-hospital supplementation after its introduction. In addition, the study sought to assess safety of this practice change with respect to the three potential adverse effects measured and showed no increase in maximum weight loss, or hyperbilirubinemia during the 3–4 day hospitalization and no increased LoS in infants born in the year following the intervention.
A number of limitations of the study must be noted. We were unable to determine if there was an increase in the hospital readmission rate of newborns for dehydration and/or hypernatremia after implementation of the intervention. However, it was reassuring that there was no significant difference in maximum weight loss or hyperbilirubinemia between the two groups of infants over the hospital stay, and all infants met the same set of discharge criteria. Our study did not establish causality. We cannot exclude the possibility that unidentified secular trends in our mother–infant unit of our Baby-Friendly Hospital played a role in the overall reduction of supplementation, although this explanation is less likely in those losing ≥10% BW. We were also unable to determine which factors in the intervention contributed to the decrease in supplementation: 24HW measurement, utilization of this weight as reference for neonatal weight loss, nursery staff education, counseling of mothers, or a combination. The 24HW measurement itself increased awareness of nursing, pediatric, and lactation staff of usual weight loss on the first day of life when infant's intake is universally limited. Infants born by vaginal births were excluded from the study due to the inability to follow their feeding and weight for more than 2 days during their stay. However, since epidural anesthesia, accompanied by intravenous fluids and fluid boluses, is almost universal during vaginal births at our institution, we believe that using 24HW for subsequent weight loss calculation may also make clinical sense in these infants and will reduce unnecessary supplementation. This requires additional study for confirmation. Finally, we urge caution in extrapolating the results to early and late preterm infants who were also excluded from the study.
The relationship between labor and infant weight loss after C-sections warrants further investigation. In our study, infants who experienced labor lost less weight by 24 hours than those delivered without labor (4.8% versus 5.5% of BW), despite fewer voids and feeds. Over the entire hospital stay, however, there was no significant difference in their maximum weight loss (Table 5). Although accurate estimation of maternal fluid balance was unavailable, the decreased intravenous fluid volume in mothers who experienced labor before C-section is a possible explanation. An additional factor is labor-induced vasopressin release, promoting neonatal fluid retention and decreased voiding, resulting in less initial weight loss.20–25
Conclusion
We have demonstrated that a simple practice change of measuring and using infant's 24HW for neonatal weight loss calculation, along with staff and parental education, can reduce supplementation and promote exclusive breastfeeding in healthy term infants delivered by Cesarean sections. This practice change was not associated with increased in-hospital weight loss, bilirubin, or LoS. Further studies should investigate the utilization of the 24HW in infants delivered vaginally, and early-term and late-preterm infants as well as post-discharge readmission rates for dehydration to confirm the safety of this practice before widespread implementation. However, results of this study infer that 24HW is an important additional parameter to include in the assessment of weight loss and hydration in healthy term breastfeeding newborn infants delivered by C-sections and whose mothers receive intrapartum intravenous fluids. If adopted by other mother–infant units, this practice may help toward meeting the public health goals of increasing the rate and duration of exclusive breastfeeding as recommended by the WHO/UNICEF BFHI, 10 the AAP, 1 Healthy People 2020 National Goals,9,26 and the perinatal core measures of the Joint Commission on Hospital Accreditation. 10
Footnotes
Acknowledgment
The authors acknowledge and thank Dr. Sandra Motta, MD, FAAP, newborn hospitalist at Connecticut Children's Medical Center, for the initial literature search for the study; Mary A. Marshall-Crim, MSN, APRN, FNP, IBCLC, Department of Women's Health, Hartford Hospital, for contributing in the interpretation of results; Trudy Lerer, Dr. Zhu Wang, PhD, and the Research Department at Connecticut Children's Medical Center for statistical help, the nursing staff and lactation consultants of the Mother-Infant Unit at Hartford Hospital for their support and encouragement. The authors also thank Dr. Alison J. Draper, PhD, Maryann McGuire, RN, MPH, and Kathy Mallinson at Trinity College, Hartford, CT, for providing Ms. Deng the opportunity to participate in this project through the Health Fellows Program during her undergraduate study.
Disclosure Statement
No competing financial interests exist.