
Abstract
Abstract
Background and Objectives:
Pasteurized donor human milk (“donor milk”) is an alternative to formula for supplementation of breastfed infants. We conducted a survey to determine (1) prevalence, trends, and hospital-level correlates of donor milk use for healthy newborns in the northeast United States and (2) clinician knowledge and opinions regarding this practice.
Methods:
We conducted parallel surveys of clinicians (88% nurse and/or lactation consultant) at (1) all birth hospitals in Massachusetts (MA) and (2) all birth hospitals served by a northeast United States milk bank. We asked about hospital use of donor milk for newborns ≥35 weeks' gestation and receiving Level I care in well nursery, hospital-related factors we hypothesized would be associated with this practice, and clinician knowledge and opinions about donor milk use.
Results:
35/46 (76%) of MA birth hospitals and 51/69 (74%) of hospitals served by the milk bank responded; 71 unique hospitals were included. Twenty-nine percent of MA birth hospitals and 43% of hospitals served by the milk bank reported using donor milk for healthy newborns. Hospitals that used donor milk for healthy newborns had higher exclusive breastfeeding at hospital discharge than hospitals that did not (77% versus 56%, p = 0.02). Eighty-three percent of respondents agreed or strongly agreed that using donor milk is an effective way to increase the hospital's exclusive breastfeeding rate.
Conclusions:
Many northeast United States birth hospitals currently use donor milk for healthy newborns. This practice is associated with higher exclusive breastfeeding at hospital discharge. Relationships with breastfeeding after discharge and related outcomes are unknown.
Introduction
O
Approximately 15.5% of all breastfed newborns in the United States receive formula supplementation in the first days of life. 2 Excessive formula use interferes with the establishment of lactation 3 and is associated with a four-fold higher risk of breastfeeding cessation by 2 months.4,5 Based on that evidence, reducing the unnecessary use of formula (a “breast milk substitute” as designated by the World Health Organization 6 ) during the birth hospitalization is a stated goal of the Baby-Friendly Hospital Initiative, 7 a global program to encourage maternity hospital practices that support of breastfeeding.
Pasteurized donor human milk (“donor milk”) is an alternative to formula for early supplementation and is used increasingly for very preterm infants in the neonatal intensive care unit (NICU).8,9 Our hospitals (Brigham and Women's Hospital and Boston Medical Center in Boston, Massachusetts [MA]) also offer donor milk to healthy newborns outside the NICU setting, and anecdotal evidence from colleagues suggests that this practice is also occurring elsewhere.
Using donor milk instead of formula for supplementation may be an effective strategy to reduce the use of breast milk substitutes, in keeping with recommendations of the Baby-Friendly Hospital Initiative. However, based on the physiology of early lactation, 3 donor milk supplementation could interfere with lactation in the same way that formula supplementation does. To our knowledge, no clinical evidence exists regarding either benefits or risks of this practice.
To begin to understand the use of donor milk for healthy newborns beyond our own institutions, we conducted a regional hospital survey to determine the extent of donor milk use for healthy newborns, and trends in this practice, in two groups of hospitals: (1) all birth hospitals in MA and (2) a defined group of birth hospitals in the northeast United States currently using donor milk.
Our secondary aims were to examine hospital characteristics that correlate with donor milk use in healthy newborns and to determine clinician knowledge and opinions regarding the use of donor milk for healthy newborns.
We hypothesized that the use of donor milk by birth hospitals in the northeast region was growing, and that specific hospital characteristics (current use of any donor milk, having a level III/IV NICU, Baby-Friendly Hospital Initiative designation, and higher exclusive breastfeeding rate) would be associated with hospital use of donor milk for healthy newborns.
Materials and Methods
Design, setting, and sample
This study was a cross-sectional online survey with two overlapping sampling frames. To determine the prevalence of donor milk use for healthy newborns among MA hospitals, we surveyed all birth hospitals in MA (n = 46 hospitals). To determine the hospital prevalence of donor milk use for healthy newborns among hospitals already using donor milk, we surveyed all birth hospitals that purchased milk from our regional Human Milk Bank Association of North America-certified milk bank (Mother's Milk Bank Northeast), which serves hospitals in 11 states and the District of Columbia (n = 69 hospitals). Due to overlap between sampling frames (n = 15 hospitals in both MA and milk bank sampling frames, see Fig. 1), the total number of unique hospitals targeted for the survey was 100.
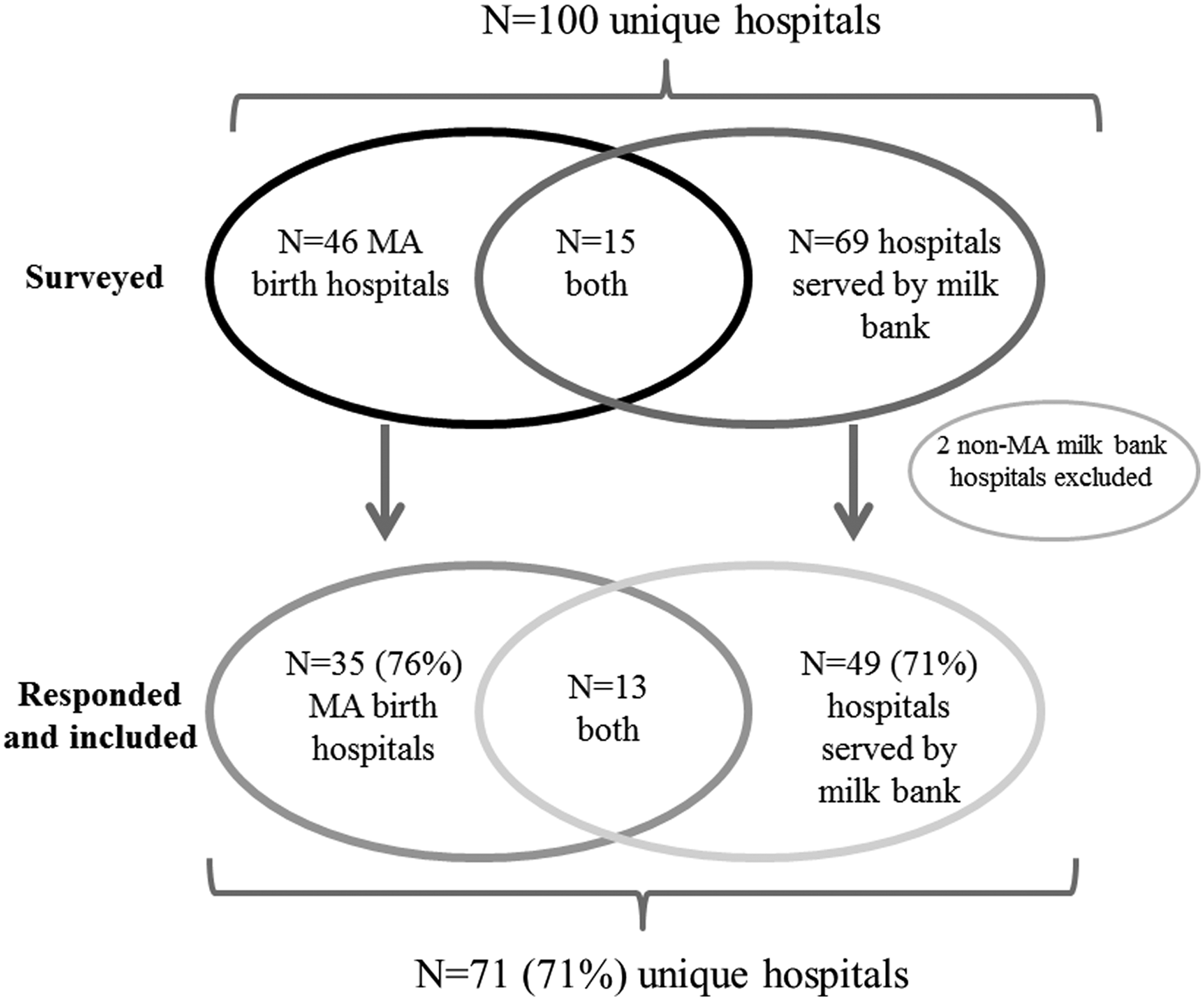
Parallel sampling frames and response rates for hospital survey of donor milk in healthy newborns. Of 100 hospitals initially contacted, 46 represented all MA birth hospitals and 69 represented hospitals in 11 states and the District of Columbia served by a single regional milk bank (Mother's Milk Bank Northeast); 15 hospitals were in both groups (MA birth hospitals also served by the milk bank). Seventy-three hospitals (71%) responded to the survey and were included in the analysis, of which 35 were MA birth hospitals and 49 were milk bank hospitals; 13 belonged to both groups. Two responding non-MA hospitals identified by the milk bank were excluded because they reported no current use of donor milk anywhere in the hospital. In total, 71 hospitals were included in this study. MA, Massachusetts.
We identified the health professional responsible for lactation efforts at each hospital through our professional networks (MA hospitals), using a contact list provided by the milk bank. This study was approved by the Institutional Review Board at Brigham and Women's Hospital. Consent was provided when the respondent clicked on a statement endorsing her willingness to participate in research.
Measurement
We adapted a survey used previously to evaluate donor milk utilization among Level III NICUs. 8 Domains assessed in our survey included the following: (1) hospital characteristics, including the highest level of neonatal care defined according to AAP guidelines, 10 Baby-Friendly Hospital Initiative status (certified or on the pathway, neither), and exclusive breastfeeding status as reported by the hospital to the Joint Commission (performance measure PC05, percent of singleton newborns ≥37 weeks' gestation fed breast milk only during the hospitalization) 11 ; (2) donor milk utilization, including use among newborns receiving different levels of neonatal care, year that hospital started using donor milk, criteria for use, and payment; and (3) clinician knowledge and opinions about donor milk, rated on a five-point Likert scale. The full survey is available upon request.
Data collection
Surveys were administered using Research Electronic Data Capture (REDCap™) tools hosted at Brigham and Women's Hospital. REDCap is a secure web-based application specifically designed to support data capture and management for research studies. 12 Survey links were embedded in emails sent to each participant. Surveys were initially sent in January 2017, with reminders sent through March 2017.
For hospitals that did not respond to the initial email requests, we identified secondary contacts through our professional networks complemented by internet searching, and emailed them survey links. For a small number of hospitals (n = 6) for which two respondents completed the survey, we verified agreement on the status of donor milk use for healthy newborns (yes/no), and chose one completed survey at random for inclusion in our analysis of provider knowledge and opinions. Three hospitals originally identified through the milk bank subsequently answered “no” to the question of whether any donor milk is used in the hospital; those hospitals were excluded from analyses because our intent was for the milk bank sampling frame to represent hospitals currently using donor milk.
Data analysis
The main outcome variable (dichotomous) was current use of donor milk for healthy newborns, defined as newborns ≥35 weeks' gestation receiving basic care (Level I according to AAP guidelines). 10 We calculated the proportion of hospitals using donor milk for healthy newborns separately within each sampling frame (all MA birth hospitals and all hospitals served by milk bank). To examine associations of hospital characteristics with donor milk use for healthy newborns, we analyzed data from all hospitals together. For dichotomous hospital characteristics (any donor milk used, Level III/IV care, Baby-Friendly certified, or on pathway), we compared proportions between hospitals that did versus did not report using donor milk for healthy newborns. We used Fisher exact tests and calculated relative risks with 95% confidence intervals (CIs). For the continuous variable (percent exclusive breastfeeding at discharge), we compared medians between hospitals that did versus did not use donor milk for healthy newborns and used Wilcoxon rank sum tests to determine statistical significance. These analyses were conducted in SAS 9.4 (SAS Institute, Inc., Cary, NC). We also used Excel (Microsoft, Seattle, WA) to plot the cumulative number of hospitals using donor milk for healthy newborns by year of initiation and fitted an exponential curve with calculated r 2 .
Results
Thirty-five (78%) of 46 MA birth hospitals and 52 (75%) of 69 hospitals served by the milk bank (73 of 100 unique hospitals) responded; 14 hospitals were represented in both sampling frames (MA hospitals also served by the milk bank). We excluded two non-MA hospitals identified by the milk bank who responded, but reported no current use of donor milk anywhere in their hospital, leaving 49 (71%) of milk bank hospitals included. Figure 1 shows these sampling frames and respective response and inclusion rates. Sixty-three (89%) respondents reported being an international board-certified lactation consultant and/or registered nurse.
Characteristics are shown in Table 1 for all hospitals combined and stratified by sampling frame. Just over half of all hospitals reported providing Level III and/or IV care, and a similar proportion reported being designated or on the pathway to designation by Baby-Friendly. The median percent of infants exclusively breastfeeding was 63% (range, 7–92%).
Milk bank hospitals from 11 states and the District of Columbia were identified through their current use of donor milk from a single regional milk bank (Mother's Milk Bank Northeast). Thirteen hospitals were in both sampling frames (MA and milk bank). Highest level of care defined according to the American Academy of Pediatrics guidelines. 10 ‘Healthy newborn’ is defined as newborn ≥35 weeks' gestation receiving Level I care. 10 Exclusive breastfeeding at hospital discharge is defined according to the Joint Commission. 11
MA, Massachusetts.
Twenty-three (32%) respondents reported that their hospitals currently use donor milk for healthy newborns. According to sampling frame, 10 (29%) of MA hospitals and 21 (43%) of hospitals served by the milk bank reported using donor milk for healthy newborns. Of the 23 hospitals that reported current use of donor milk for healthy newborns, 20 responded to the survey question, “What year was donor milk first offered to healthy newborns in your hospital?” Figure 2 shows the cumulative number of hospitals engaged in this practice rising exponentially from 2008 to 2016.

Cumulative number of birth hospitals using donor milk for healthy newborns, defined as newborns ≥35 weeks' gestation who are receiving routine care (Level I). Data are from a 2017 survey of 73 lactation providers at birth hospitals in the northeast United States. Respondents were asked to identify the year the hospital started providing donor milk to healthy newborns. Reported use of donor milk for healthy newborns increased from one hospital in 2008 to 20 hospitals in 2017, consistent with an exponential increase in the number of hospitals over this time period (exponential trend shown as dashed line).
Table 2 shows associations of donor milk use for healthy newborns with hospital characteristics. The percent of infants exclusively breastfeeding at hospital discharge was higher in hospitals that provide donor milk to healthy newborns than hospitals that do not (77% versus 56%, p = 0.02). Baby-Friendly Hospital Initiative designation was also associated with more use of donor milk for healthy newborns, but confidence limits did not exclude the null (relative risk 2.18, 95% CI 0.87, 5.47).
Exclusive breastfeeding at hospital discharge was defined according to the Joint Commission. 11 Level III or IV care defined according to the American Academy of Pediatrics guidelines. 10
Unable to calculate relative risk due to zero cell.
Fisher exact test.
Wilcoxon Rank Sum test.
Practices within hospitals that currently use donor milk for healthy newborns (n = 23) are shown in Table 3. All hospitals reported having a written policy regarding the use of donor milk, and all but one reported requiring parental consent for donor milk. All but one hospital reported paying for donor milk from a hospital budget; the estimated amount spent on donor milk in the past year ranged from $200 to $12,000.
Only hospitals currently using donor milk for healthy newborns were asked these survey questions. Percentages may not sum to 100% due to rounding.
Some hospitals selected >1 payment method.
Table 4 details respondent knowledge and opinions about donor milk. Whereas 97% agreed or strongly agreed that studies show health benefits of donor milk for very preterm infants, somewhat fewer (78%) agreed or strongly agreed with the same statement for healthy newborns. Ninety-four percent of respondents agreed or strongly agreed with the statement that studies show that using donor milk increases exclusive breastfeeding after hospital discharge for healthy newborns. Eighty-three percent agreed or strongly agreed that using donor milk is an effective way to increase the hospital's exclusive breastfeeding rate.
Percentages may not sum to 100% due to rounding.
Eighty-eight percent of respondents were board-certified lactation consultants and/or registered nurses.
Discussion
Using donor milk for sick, preterm infants whose mother's own milk is in short supply is an increasingly widespread practice in the NICU setting,8,13 and one that is endorsed by the AAP based on strong evidence for health benefits in that patient population.1,9 Results from our survey demonstrate that the practice of using donor milk for supplementation during the newborn hospitalization is now disseminating to healthy newborn populations, at least in the northeast United States. We believe our study is the first to demonstrate the extent of this practice in birth hospitals within a geographic region (MA). Importantly, our results suggest an exponential rise in the number of hospitals offering donor milk to healthy newborns over an 8-year time frame (2008–2016) in our region, consistent with a substantial “drift” of a practice that is grounded primarily in evidence from sick, preterm populations.
Evidence from randomized trials in preterm, very-low-birth-weight infants demonstrates that the major health benefit of supplementing maternal milk with donor milk rather than formula is a reduction in the risk of necrotizing enterocolitis (NEC),14,15 a life-threatening gastrointestinal condition. Consistent with that evidence base, virtually all respondents in our survey agreed or strongly agreed with the statement that “studies show health benefits of donor milk for very preterm infants.” However NEC affects very preterm infants almost exclusively,16,17 whereas healthy newborns (even ones born late preterm at 35–36 weeks' gestation) face an extremely low risk of developing NEC.
Published data demonstrating clinical or health benefits of donor milk for healthy newborns are lacking. Our literature search yielded only a single two-patient case series describing this practice at a large birth hospital in Iowa 18 and a recently completed (but not yet published) randomized controlled trial that compared breastfeeding continuation outcomes between full-term newborns at risk for excessive weight loss supplemented with small volumes of donor milk versus routine care (NCT02221167). Nonetheless, the Academy of Breastfeeding Medicine (ABM) explicitly endorses the use of donor milk rather than formula if supplementation is required, 19 and the AAP also recommends supplementation with donor milk for healthy term infants, 1 although neither organization cites clinical evidence from healthy newborn populations supports this recommendation. In our survey, 78% of respondents agreed or strongly agreed that “studies show health benefits of providing donor milk to healthy full-term infants.” This perception of health benefits may also be common among mothers in the birth hospitalization period, as demonstrated by a recent qualitative study. 20 The practice of using donor milk for healthy newborns may be driven by a belief in its benefits, but objective evidence about health benefits is currently lacking.
The use of donor milk in healthy newborns has regulatory implications. The Joint Commission now requires birth hospitals with ≥300 deliveries per year to report the percent of infants who were fed only breast milk during the hospital stay, but does not discriminate maternal milk from donor milk. 11 Similarly, the Baby-Friendly Hospital Initiative requires certified hospitals to minimize the use of “breast milk substitutes” in keeping with the International Code of Breast Milk Substitutes, 6 but does not consider donor milk a breast milk substitute. 7 The intention of these organizations is to support breastfeeding by reducing early, unnecessary formula supplementation. However, birth hospitals wishing to improve their performance on the Joint Commission exclusive breastfeeding metric could conceivably do so by providing donor milk as a supplement rather than formula, without necessarily engaging in other practices that support exclusive direct breastfeeding.
Our finding that hospitals providing donor milk to healthy newborns had higher exclusive breastfeeding rates (assessed with the Joint Commission metric) supports our hypothesis that donor milk use is one factor contributing to better performance, and >80% of our respondents endorsed the statement that using donor milk is an effective way to increase the hospital's exclusive breastfeeding rate. Given the broad umbrella of the Joint Commission and the national effort underway currently to increase the number of Baby-Friendly-designated hospitals 21 —as well as a growing supply of donor milk from nonprofit milk banks 22 and for-profit companies (e.g., Medolac, Prolacta)—our findings suggest the importance of modifying metric definitions to differentiate babies fed exclusively their own mother's milk from those who receive supplementation with donor milk. The rationale for this suggestion is to provide clarity, because donor milk is considered a supplementary feeding according to a current ABM clinical protocol, 19 but is different from formula and other breast milk substitutes commonly used for supplementation.
Using donor milk may be beneficial when supplementation is medically necessary, for example, by promoting increased breastfeeding as described previously in the NICU setting, potentially due to an increased awareness by families and staff of the importance of human milk. 23 Using donor milk rather than formula for medically necessary supplementation would also reduce exposure to formula marketing in the hospital setting, which is important because formula marketing can undermine a mother's confidence in breastfeeding. 24
However, the practice may also have unintended consequences, particularly among healthy newborns. In the United States, 20% of breastfed newborns receive some formula in the first 2 days of life. 2 Although supplementation is sometimes medically necessary and feeding very small amounts of formula may be a useful short-term “bridge” until a mother's milk supply is established, 25 most studies show that early formula use is associated with a shortened breastfeeding duration.4,5,26–29 The hypothesized physiologic mechanism by which early supplementation interferes with the establishment of breastfeeding involves a “vicious cycle,” whereby formula supplementation decreases the infant's demand to breastfeed, leading to milk stasis that feeds back to lower milk supply, creating or accentuating maternal concern about her supply, which increases formula supplementation. 3 This cycle leads eventually to early breastfeeding discontinuation. Although research on the topic of early supplementation has focused primarily on infant formula, it is biologically plausible that donor milk may also interfere with breastfeeding through similar mechanisms. In our study, it was notable that no hospital reported having a limit on the volume of donor milk per baby, but we did not quantify the actual volume typically dispensed or consumed by the baby, nor did we have data on breastfeeding continuation rates after hospital discharge.
The strength of our study is the relatively high (73%) response rate, facilitated by our use of professional contacts to identify a lactation-focused clinician at each target hospital. A limitation is that we studied only hospitals in the northeast United States, reducing generalizability. The percent of hospitals in states other than MA currently using donor milk for healthy newborns may be higher or lower than what we observed in our own state (29% of MA birth hospitals currently using donor milk for healthy newborns). In addition, the percent of hospitals using donor milk for healthy newborns is almost certainly higher among hospitals already using donor milk (e.g., 43% of our milk bank sampling frame), compared with a more representative sample of hospitals.
Nonetheless, our results clearly demonstrate that a growing number of hospitals in our region are currently using donor milk for healthy newborns. We surveyed primarily lactation consultants and nurses, who may exert a strong influence on breastfeeding-related practices within their hospital, but do not represent the knowledge or opinions of physicians or other healthcare professionals. We also relied on clinician report of their hospital's exclusive breastfeeding rate as reported by their hospital to the Joint Commission, with potential for error. In addition, we did not collect individual patient-level data, for example, regarding specific indications for use of donor milk (e.g., late preterm, other diagnosis).
Conclusion
The use of donor milk for healthy newborns is on the rise in birth hospitals in the northeast United States. This finding should be considered in the context of current ABM and AAP guidelines that endorse the use of donor milk for healthy newborns, as well as efforts to promote breastfeeding by advocacy and regulatory organizations such as the Baby-Friendly Hospital Initiative and Joint Commission. These organizations should consider modifying key breastfeeding metrics to distinguish exclusively breastfed (no supplement) infants from breastfed infant who receive supplementation with donor milk, and to ensure that incentives are designed to prioritize evidence-based practices that support direct and exclusive breastfeeding and decrease unnecessary supplementation, including supplementation with donor milk.
In addition, pediatricians and other clinicians caring for newborn infants in the hospital after birth should be aware of the lack of clinical evidence and potential for unintended consequences of this practice, including interference with early lactation. As a next step, a national survey such as Maternity Practices in Infant Nutrition and Care is well positioned to establish the extent of this practice in well-baby nurseries across the United States, as well as regional differences and relationships with other hospital practices. Further research is also urgently needed to determine the clinical outcomes related to the use of donor milk for medically indicated supplementation in the healthy newborn population.
Footnotes
Acknowledgments
The authors acknowledge Naomi Bar-Yam, PhD, and Cynthia Cohen (Mother's Milk Bank Northeast) for their assistance in identifying professional contacts at the hospitals included in this research. Funding: National Institutes of Health K23HD074648 (S.S.); Nurse Scientist Program, Brigham and Women's Hospital (K.E.G.); Karsh Award, Brigham and Women's Hospital (J.F.R.), and W.K. Kellogg Foundation (B.L.P.)
Disclosure Statement
No competing financial interests exist.