
Abstract
Abstract
Background:
It is not uncommon for mothers to have persistent pain with breastfeeding beyond the first few weeks after birth. Persistent pain can be multifactorial, with neuropathic pain maintained by central sensitization being one dimension. Our knowledge in delineating categories of persistent pain is simple and not very sophisticated.
Methods:
We have developed and tested a Lactation Quantitative Sensory Test (L-QST) to quantify the neuropathic component of persistent breastfeeding pain. We present three case reports of neuropathic breastfeeding pain and treatment, and we discuss the potential role of histamine and catecholamines in persistent breastfeeding-associated pain.
Conclusions:
The L-QST can be a useful tool to quantify neuropathic pain. Further studies are needed to test inter-observer reliability and reproducibility of this tool. Antihistamines can be considered for treating persistent pain in breastfeeding women with a history of allergy or atopy, and beta-blockers may be helpful in women with multiple pain disorders.
Introduction
P
In our clinical practice, we have observed variation in pain sensitivity among women with persistent pain, and we have developed and implemented a Lactation Quantitative Sensory Test (L-QST) in an effort to distinguish neuropathic functional pain from other causes. Here, we present the rationale for L-QST, followed by three cases managed in our clinic.
Methods
Rationale for quantitative sensory testing
Wide inter-individual variation exists in pain perception. Individuals can perceive a nonpainful stimulus as painful (allodynia), or can experience increased pain from a normally painful stimulus (hyperalgesia). 5 Both allodynia and hyperalgesia can complicate management of persistent breastfeeding-associated pain. For example, for a lactating woman with allodynia, an anatomically normal latch may be perceived as painful. Similarly, a woman with hyperalgesia may experience slight nipple compression during let down as excruciating. A standardized method is therefore needed to quantify pain perception.
To accomplish this goal, we used principles from quantitative sensory testing of women with vulvodynia to develop the L-QST. In previous studies of vulvodynia/vestibulodynia, a decrease in the threshold for pain with pressure suggests central sensitization.5–7 For the L-QST, we used the cotton-ball end of a Q-tip as a standardized nonpainful stimulus, and the sharp end as a standardized painful stimulus. We marked the Q-tip at 1 cm intervals from 0 to 10 cm to facilitate measurement of distances during the exam.
L-QST procedure
Before testing, the patient undresses from the waist up and puts on a gown open in the front. We begin the exam by touching the right shoulder with the cotton ball, applying just enough pressure to blanch the skin. This establishes “normal” sensation, remote from the breast. We explain that we will move medially from the lateral edge of the breast toward the nipple, applying the same pressure to the skin at 1 cm intervals. We ask her not to watch during testing, and to focus on her perception. She is asked to tell the examiner to stop when the cotton ball feels different.
When the patient reports that the sensation is different from the original perception on her shoulder, we ask if it is “unpleasant,” “painful,” “different,” or “other.” We then ask her to quantify this altered perception on a scale of 0–10. We record the distance from nipple to the point of altered perception using markings on the Q-tip shaft. We repeat this process on the lateral side of the left breast. We then move to medial side of the right breast, establishing “normal” cotton ball perception on the sternum and moving toward the nipple, and then the medial side of the left breast. We alternate between breasts because when we performed a complete exam on the right breast first, we found consistently higher pain scores on the left breast, raising concern for contralateral sensitization by the exam procedure. 8
Following assessment of allodynia with the cotton ball end of the Q-tip, we break the wooden shaft of the Q-tip to create a sharp tip. We establish “normal” pin-prick sensation on the shoulder, and then we move medially toward the nipple at 1 cm intervals until the sensation feels different. As with the cotton ball, we ask if it is “unpleasant,” “painful,” “different,” or “other,” we ask her to quantify this altered perception on a Scale of 0 to 10, and we record the distance from the nipple to the point of altered perception. These assessments are recorded in a standardized form (Fig. 1 UNC-Lactation QST form).
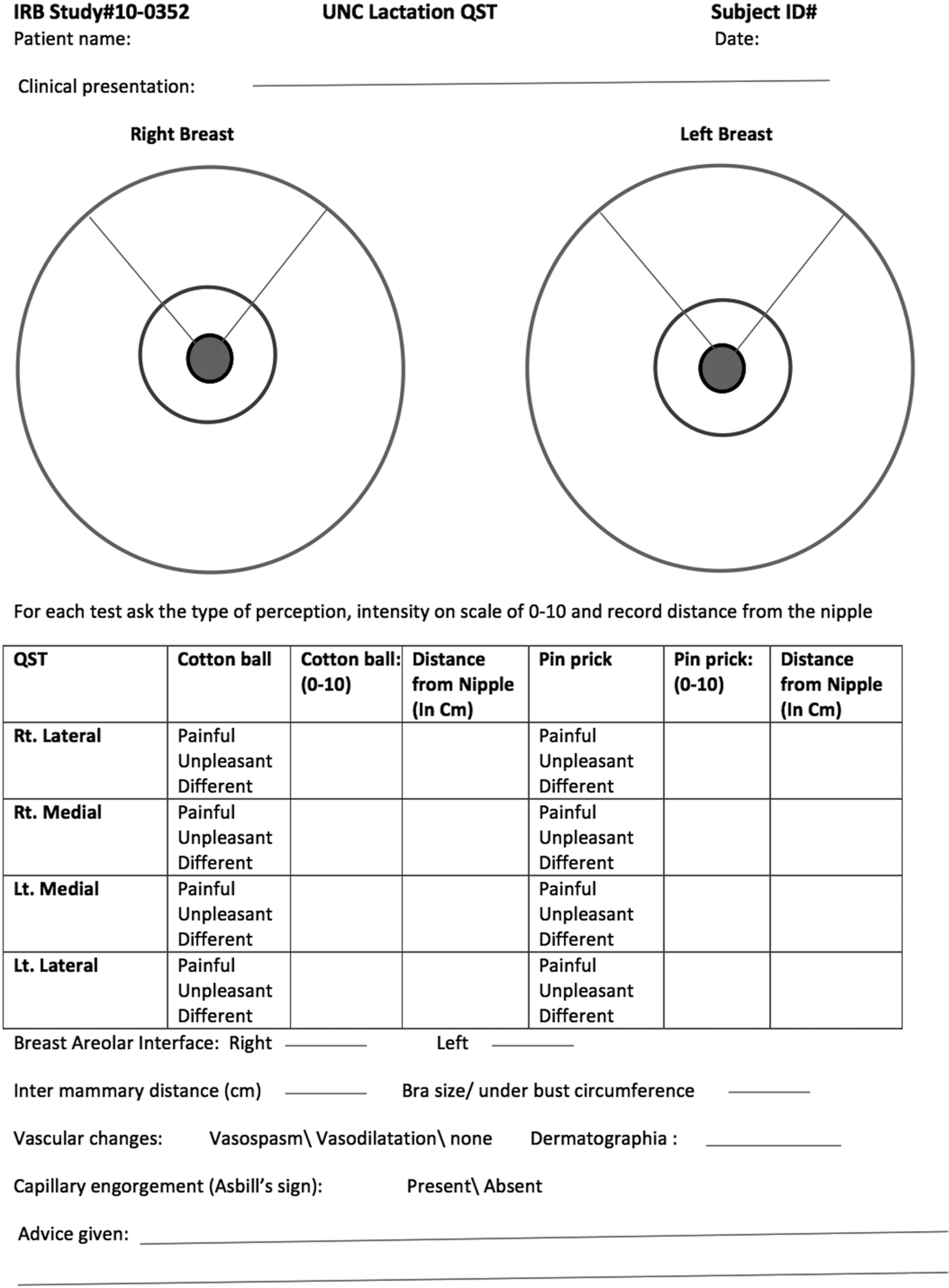
UNC Lactation Quantitative Sensory Testing Form.
Interpretation of QST: Sensory varies in different types of skin tissue, and most individuals experience both light touch and pin prick as “different” at the junction of two different skin types, such as areolar-cutaneous junction. In women without breastfeeding-associated pain, we have found a difference in sensation of light touch at either the areolar-cutaneous junction or the shaft of the nipple, and a difference in pin-prick at the areolar-cutaneous junction. However, among women with neuropathic central sensitization, light touch perception can be unpleasant at the outer edge of the breasts, and may even be painful (Allodynia). Similarly, they perceive pinprick as painful or unpleasant several centimeters out from the areolar-cutaneous junction. The boundary of this increased sensitivity is often marked by a lacey, capillary pattern in the skin, the Asbill sign, first described by article co-author Diane Asbill (Fig. 2). Of note, we have also observed this pattern in women without allodynia or hyperalgesia; the Asbill sign is therefore not pathognomonic of breastfeeding-associated pain. We speculate that the vascular changes observed are perceived as painful among women with CSS.
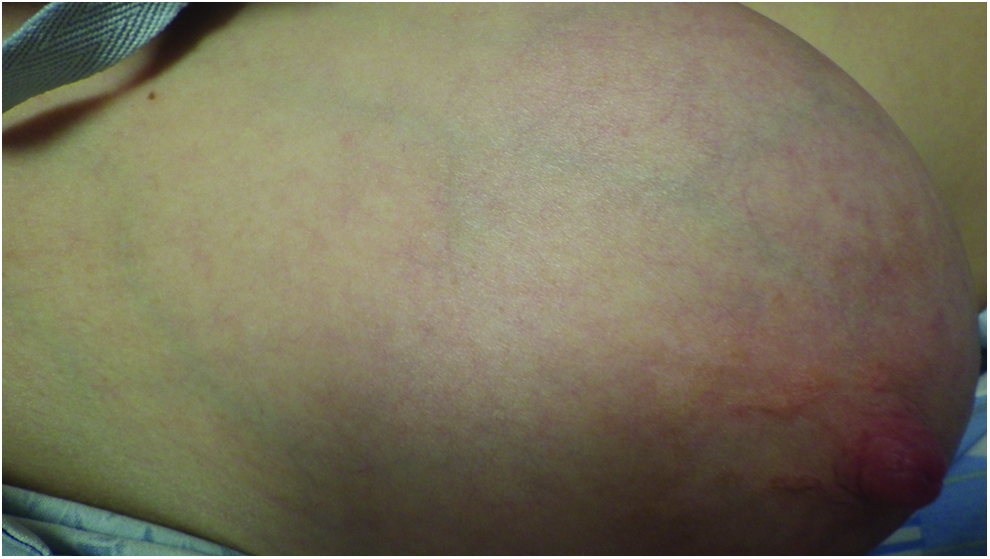
Asbill's Sign/Lacy capillary pattern. Color images available online at www.liebertpub.com/bfm
Potential mechanisms of pain sensation
We propose that histamine and catecholamines may contribute to centrally mediated breastfeeding-associated pain.
Persistent breastfeeding-associated pain is commonly described as itching or burning. Similar symptoms can be caused by mast cell degranulation and release of histamine. Histamine is released from mast cells when they are activated by antigen-bound IgE, or in response to other stimuli, such as stress or mechanical stimuli. This can be evident clinically as dermatographia, or skin-writing, resulting in erythema and induration after stroking of the skin. We assess our patients for dermatographia by dragging wooden tongue depressor blade across the surface of the forearm. Histamine binds to H1 receptors that are present on small blood vessels and terminal neurons, stimulating vasodilatation of small capillaries and irritating sensory neurons, which is perceived as itching. 9 We speculate that histamine release may contribute to the hyperalgesia and allodynia observed at the boundary of the Asbill sign. Antihistamines reduce allergic inflammation by inhibiting mast cell activation by downregulating intracellular calcium ion accumulation. 9
Several lines of evidence support the hypothesis that histamine and mast cell degranulation may play a role in breastfeeding-associated pain. Numerous mast cells are present in the breast, and anaphylaxis with breastfeeding has been described in case reports.10–12 This phenomenon is thought to be related to mast-cell instability in the setting of falling levels of gonadal steroids in the early postpartum period.10–13 Indeed, some authors have suggested that uterine mast cells play a role in human parturition. 14 We speculate that mast cell instability, triggered by falling progesterone levels, may mediate increased breast sensitivity in the early postpartum period. 15
Emerging evidence in animal studies has established the role of histamine in inducing nociception, 16 maintaining sympathetically mediated neuropathic pain 17 and altering pain-related behaviors. 18 Histamine in the locus coeruleus modulates noradrenaline in pain perception. 19 Histamine also contributes to pain in the temporomandibular joints (TMJ) of rats 20 and may contribute to irritable bowel syndrome in humans. 21 For women with a history of allergic or atopic disease, dermatographia, or chronic pain syndromes, we offer a trial of nonsedating antihistamines as a potential therapy for persistent breastfeeding-associated pain. We counsel women that this is an off-label use of the medication, and we review that antihistamines could in theory affect milk supply; however, in a series of 51 women treated with antihistamines, 1 of 51 reported a reduction in milk supply. 22 As noted in the “Case Study 1” below, we have found antihistamines can reduce persistent breastfeeding-associated pain in some women.
Several lines of evidence suggest that catecholamines also play a role in centrally mediated pain syndromes. For example, in injury and inflammation, noradrenaline contributes to feedback inhibition of pain, 8 and noradrenaline lesions of the locus coeruleus in animal models decrease development of allodynia and hyperalgesia.23–27 In addition, beta-adrenoceptors are implicated in modulation of pain sensitivity, 28 and drugs that increase norepinephrine levels, such as tricyclic antidepressants and SNRIs, can promote analgesia. 29 There is also evidence that variation in catecholamine metabolism is associated with pain sensitivity.30,31 Chronic pain disorders are associated with increased catecholamine levels and reduced activity catechol-O-methyl transferase (COMT). In an animal model of COMT inhibition, investigators found that both adrenalectomy and beta-adrenergic receptor antagonists prevented development of hypersensitivity.32,33 Moreover, genetic variations in the COMT enzyme are associated with pain syndromes, such as TMJ disorder16,17 and with differential sensitivity to pain processing. 33 Prior studies have found that treatment with propranolol ameliorates TMJ in patients with specific COMT polymorphisms 34 and increases pain tolerance in women with menstrual-related mood disorder. 35 In women with breast allodynia or hyperalgesia, we have also found that propranolol can be helpful. We initially began using propranolol based on evidence of relief for TMJ and migraine prophylaxis.36,37 For women with allodynia, especially in the setting of other chronic pain disorders, we offer a trial of propranolol, typically starting with 20 mg three times a day. We counsel women that this is an off-label use of the medication. Existing evidence suggests that low levels of propranolol are present in milk; no special precautions are required. 38
Case study 1
A 31y/o G1P1 at 8 weeks postpartum presents with pain and low milk production. Her breastfeeding course was complicated by cracked nipples during week 1 postpartum, and her pain did not improve after the infant underwent a frenotomy at 4 weeks. When we saw her at 8 weeks, there were no visible nipple cracks, and the infant orofacial and suck exam was within normal limits. She was both breastfeeding and supplementing with formula.
She reported significant pain in her left breast at the end of every feeding, which she described as an itching and burning sensation with average intensity of 8 on a scale of 0–10. She has similar pain in between feedings almost every day.
Physical examination was notable for asymmetrical breasts, with a small right breast and normal-appearing left breast with veining and an average amount of palpable glandular tissue. She also had marked dermatographia in response to stroking of the forearm with a tongue depressor. On L-QST, pain lateralized to the left side, with allodynia and hyperalgesia 10–12 cm from the nipple, consistent with a possible functional pain syndrome (Table 1).
Treatment
Given dermatographia and itching, burning pain, the patient was advised to initiate cetirizine 10 mg QD. One week later, she reported her pain was markedly improved, rating her pain as “much better” on 5-point Likert scale of “much worse” to “much better.”
Case study 2
A G1P1 exclusively breastfeeding at 17 weeks postpartum called the UNC Lactation Warm Line reporting sharp, stabbing, and burning pain in the lower part of her left breast that wakes her up at night. She started having pain after 10 days of antibiotics for mastitis in left breast at 3 weeks postpartum. Previous treatments included a variety of hygiene measures to prevent thrush, heat to breasts, and clipping of the baby's lip tie at 11 weeks without much relief. The baby bit down on her left nipple at 15 weeks, and her pain had escalated over the following 2 weeks. She reported that ibuprofen had helped to “take the edge off.” Her history was notable for seasonal allergies, hypertension, migraines, hypothyroidism, bowel pain, pain with intercourse, dysmenorrhea, Graves' disease, recurrent miscarriages, infertility, and breast sensitivity in cold temperatures. A trial of cetirizine was suggested over the phone, and she was scheduled for follow-up in 2 weeks in the breastfeeding medicine clinic. On presentation at 19 weeks postpartum, she reported marked improvement with the antihistamine; her pain intensity had decreased from “slightly intense” to “very weak” and its unpleasantness had decreased from “very distressing” to “annoying.”
L-QST was notable for allodynia and hyperalgesia bilaterally. In addition, marked erythema appeared at the site of sharp touch at the chest wall, suggesting mast cell degranulation (Table 2).
Treatment
Given a history of multiple pain syndromes and evidence of allodynia and hyperalgesia, the patient was advised to continue the antihistamine and initiate propranolol 20 mg TID, with a plan to titrate up to 80 TID.
Follow-up
After a week of propranolol 20 mg TID and daily cetirizine, she reported having no pain. She discontinued the propranolol at 3 months and had no reoccurrence of the breast pain. She exclusively breastfed for 6 months and continued breastfeeding for 1 year.
Case study 3
A 35 y/o G1P1 presented at 4 weeks postpartum with “toe curling pain” with nursing. Her breastfeeding course had been complicated by cracks and nonhealing fissures, which had been treated with mupirocin and ibuprofen. Physical exam was notable for yellowish exudate adjacent to the fissures, suggesting staph aureus. Pain was worse with exposure to cold. She was treated with dicloxacillin and ibuprofen, and nifedipine for cold sensitivity. Two weeks later, she had completed her antibiotics and was pain-free with nifedipine. She represented 2 weeks later with new, different, right-sided burning pain, 8/10 throughout every feeding, which she rated as intense and intolerable.
On examination, tenderness was noticed on right pectoralis major near the sternum. L-QST was notable for right-sided allodynia and hyperalgesia (Table 3).
Treatment
Differential diagnosis at that time was functional pain, ductal infection, or musculoskeletal pain. The patient was advised to continue nifedipine and add propranolol, 20 mg TID. Given her recent treatment for mastitis and the hypothesized role of breast dysbiosis in breast pain, 39 probiotics were also suggested, and a referral was made for physical therapy.
Follow-up
Two weeks later, she reported that she stopped nifedipine after a couple of days. Her pain had completely resolved with propranolol and probiotics. She had cancelled her physical therapy appointment. On long-term follow-up, she said she stopped taking propranolol after 2 weeks and her pain did not return. She breast fed exclusively for 6 months and continued pumping for 12 months.
Discussion
In this case series, we present three breastfeeding mothers with intense, itching, burning pain and findings of allodynia and hyperalgesia, documented using a L-QST. Symptoms of breast itching and burning have traditionally been attributed to thrush. 40 However, Hale et al. found no evidence of candida species in a series of women with classic symptoms of ductal candida. 41 Histamine is also implicated in recurrent vulvovaginal candidiasis (VVC) infections: in a small study, women with a history of atopy and recurrent VVC who did not response to fluconazole alone had resolution of their symptoms when treated with fluconazole and cetirizine. 42 It is plausible that women with burning, itching breast pain and a history of VVC are presumptively diagnosed with ductal candida, but in fact, their symptoms are due to excessive histamine release. In the series presented here, we found that treatment with oral antihistamines and beta-blockers was associated with resolution of pain symptoms. We present this case series to stimulate research on effective treatments for allodynia and hyperalgesia in breastfeeding women. Our clinical experience with antihistamines and propranolol is encouraging; however, without a blinded, placebo-controlled trial, we cannot determine whether the patients' improvement was due to effective therapy, a placebo effect, or the natural course of the disease. In case 3, it is also possible that probiotics might have led to pain resolution. Further work is also needed to determine the inter-individual reliability of the L-QST, and to establish thresholds for sensitivity in normal, asymptomatic women.
Evaluation of persistent breastfeeding-associated pain is challenging, because a comprehensive workup requires evaluation of both the mother and child. The L-QST has the potential to assist the clinician in evaluation and management of this common condition. Moreover, both antihistamines and beta-blockers may be novel, effective strategies to reduce maternal pain and enable women to achieve their infant feeding goals. Further research is needed to determine the efficacy of these tools in clinical practice.
Footnotes
Acknowledgments
“Lactation Quantitative Sensory Testing (L-QST) In Persistent Breastfeeding Pain,” selected for Poster presentation at Academy of Breastfeeding Medicine Conference 2018, Atlanta, GA, USA.
“Lactation Quantitative Sensory Testing to Detect Neuropathic Component of Persistent Breastfeeding Pain” Poster presented at North Carolina Lactation Consultant Association Breastfeeding Summit, May 2017, Wilmington, NC, USA.
Disclosure Statement
No competing financial interests exist.