
Abstract
Abstract
Background and Objectives:
Tennessee has low breastfeeding rates and has identified opportunities for improvement to enhance maternity practices to support breastfeeding mothers. We sought a 10% relative increase in the aggregate Joint Commission measure of breastfeeding exclusivity at discharge (TJC PC-05) by focusing on high-reliability (≥90%) implementation of processes that promote breastfeeding in the delivery setting.
Methods:
A statewide, multidisciplinary development team reviewed evidence from the WHO-UNICEF “Ten Steps to Successful Breastfeeding” to create a consensus toolkit of process indicators aligned with the Ten Steps. Hospitals submitted monthly TJC PC-05 data for 6 months while studying local implementation of the Ten Steps to identify improvement opportunities, and for an additional 11 months while conducting tests of change to improve Ten Steps implementation using Plan-Do-Study-Act cycles, local process audits, and control charts. Data were aggregated at the state level and presented at 12 monthly webinars, 3 regional learning sessions, and 1 statewide meeting where teams shared their local data and implementation experiences.
Results:
Thirteen hospitals accounting for 47% of live births in Tennessee submitted data on 31,183 mother–infant dyads from August 1, 2012, to December 31, 2013. Aggregate monthly mean PC-05 demonstrated “special cause” improvement increasing from 37.1% to 41.2%, an 11.1% relative increase. Five hospitals reported implementation of ≥5 of the Ten Steps and two hospitals reported ≥90% reliability on ≥5 of the Ten Steps using locally designed process audits.
Conclusion:
Using large-scale improvement methodology, a successful statewide collaborative led to >10% relative increase in breastfeeding exclusivity at discharge in participating Tennessee hospitals. Further opportunities for improvement in implementing breastfeeding supportive practices were identified.
Introduction
H
The “Ten Steps to Successful Breastfeeding” (Ten Steps) compiled by WHO and UNICEF provide a package of evidence-based guidelines for maternity practices to improve breastfeeding. 7 Implementation of the Ten Steps has improved breastfeeding initiation and duration in diverse maternity care settings, including urban U.S. safety net hospitals.8,9 Hospitals can earn Baby Friendly Hospital Initiative (BFHI) designation through a formal external review process documenting implementation of all Ten Steps. 10 In addition, a dose–response effect of Ten Step implementation on breastfeeding initiation and sustainment has been demonstrated; even implementation of five steps can increase breastfeeding duration.11,12
Tennessee, like much of the southeastern United States, has low breastfeeding rates, but is unique as the only state with major metropolitan areas in both Appalachia and the Mississippi River Delta Regions, two geographic regions with markedly poor population health outcomes including very low breastfeeding rates.13,14 In 2010, 65.4% of Tennessee babies initiated breastfeeding, but only 9.2% were exclusively breastfed at 6 months, 14 far below the Healthy People 2020 breastfeeding goals of 81.9% initiation and 25.5% exclusivity at 6 months. 15 Tennessee also perennially ranks in the lowest quintile nationally for implementing maternity practices that support breastfeeding, as measured by Maternity Practices in Infant Nutrition and Care (mPINC) surveys.16,17
The Tennessee Initiative for Perinatal Quality Care (TIPQC) is a statewide perinatal quality collaborative seeking to improve health outcomes for mothers and infants through large-scale quality improvement (QI) initiatives. 18 TIPQC leadership voted to develop a multicenter, statewide QI initiative to improve local implementation of supportive maternity practices, and to increase breastfeeding initiation rates across Tennessee.
However, as evidenced by Tennessee's poor mPINC performance at the time of project development, 17 hospital breastfeeding culture represented a substantial challenge. Hospital leaders, bedside nurses, and physicians frequently expressed that “our mothers don't breastfeed.” Most participants self-reported limited formal QI experience and most hospitals noted low resource allocation for systems improvement efforts, which created additional challenges. No Tennessee hospitals had BFHI designation when project design started, and <5% expressed interest in this designation. Despite these challenges, hospital administrators were anticipating the mandatory reporting of the Joint Commission Perinatal Care Core Measure 05 for exclusive breastfeeding at hospital discharge (TJC PC-05), 19 and so expressed interest in a minimally data-intensive improvement initiative. Accordingly, TJC PC-05 breastfeeding exclusivity measure was selected as the primary outcome for the breastfeeding project. The primary aim of the breastfeeding project was achievement of a 10% relative increase in aggregate breastfeeding exclusivity at hospital discharge, as measured by TJC PC-05, through high-reliability (>90%) implementation of processes that promote and support breastfeeding in the delivery setting (the Ten Steps to Successful Breastfeeding).
Methods
Approach
TIPQC convened a project development committee to engage stakeholders in the design of the project, including nurses, lactation consultants, physicians, hospital leaders, and Tennessee breastfeeding experts. The committee identified evidence-based practices to improve breastfeeding for statewide implementation from a breastfeeding literature review, including resources, policy statements, and protocols from WHO/UNICEF, AAP, AAFP, ACOG, the Academy of Breastfeeding Medicine (ABM), and the United States Breastfeeding Committee (USBC) toolkit on implementation of TJC measure for exclusive breastfeeding.3–5,20,21 Identified process indicators were organized to align with the Ten Steps to Successful Breastfeeding and provided to participating hospitals as a toolkit. Each of the Ten Steps was defined as one process indicator and measured by local hospital developed audit (number compliant divided by number measured).
Toolkit
The final toolkit included an executive summary, review of the evidence, summary of state and national breastfeeding data highlighting opportunities for improvement, review of large-scale breastfeeding promotion efforts,12,22 and Tennessee success stories. Technical guidance was provided on measuring the primary outcome according to TJC recommendations regarding inclusion and exclusion criteria. Identified process indicators were organized by the Ten Steps, and presented with a rationale for and suggested strategies to achieve high-reliability implementation. No specific guidance was provided for modification of participant's electronic medical record systems.
Pilot hospitals
Six pilot birthing hospitals were recruited to explore the feasibility of collecting TJC PC-05 while examining their maternity care practices as outlined in the toolkit. These hospitals were identified as institutions already collecting TJC PC-05 before the measure became mandatory, with an interest in improving their breastfeeding rates. Their collective experience exhibited a proof-of-principle that other hospitals could use as positive reinforcement to join the project. With the experience of the pilot teams, seven additional hospitals were recruited to join the project through project promotion at the TIPQC annual meeting, where many hospitals are in attendance. Incentives for participation were limited to access to collaborative guidance to improve maternity care practices to support breastfeeding, and recognition of participation on the TIPQC website. Hospital leaders were especially interested in the project in anticipation of the imminent requirement to report the mandatory TJC PC-05 measure.
Prework and QI training
At a statewide face-to-face kick-off meeting, convened and coordinated by TIPQC, interested hospitals brought their own breastfeeding improvement teams, made up of physicians, nurses, lactation consultants, and administrators and went through “QI 101” led by TIPQC QI experts. Individual hospital teams developed local aims and goals, explored effective team formation, devised an elevator speech, and planned the first PDSA (Plan-Do-Study-Act) cycle. DICE scores to determine likely success of the project (Duration, Team Performance Integrity, Commitment, Effort), key driver diagrams (a tool to conceptualize an issue and its components to demonstrate a pathway to achieve desired outcomes), and flowcharting were recommended QI tools. 23 Instructions were provided for completing monthly Leadership Reports and data collection according to TJC PC-05 requirements and entry into the statewide database. State leaders and pilot hospital teams guided new teams on a toolkit “walk-through” including discussion of rationale, strategies and resources for implementation, potential challenges, and pilot center experiences for each step. Teams also viewed posters from pilot hospital teams and shared early adopter experiences during networking opportunities.
Experience during pilot testing of the data collection tool confirmed stakeholder concerns that few hospitals had resources to concurrently implement multiple steps. Accordingly, hospital teams were encouraged to attempt to achieve high-reliability implementation on at least five of the Ten Steps using PDSA cycles as described in the Model for Improvement. 23 Selection of which steps to implement was left to each individual hospital team based upon what they thought they could accomplish in their own institution. Attempted implementation was defined by submission of process data on each step.
Learning collaborative work
Following the Institutes for Healthcare Improvement's Break-Through Collaborative framework, 24 all teams met in monthly webinar huddles (online group discussions), semiannual regional learning sessions, and an annual statewide TIPQC collaborative meeting. Each huddle included QI methods training, state aggregate data review, and standardized presentations of data and implementation experiences from each participating hospital, highlighting qualitative successes and challenges. Team presentations were guided by a Leadership Report tool to facilitate monthly collection and discussion of qualitative data describing local successes and barriers encountered during the project.
Huddles
Monthly webinar meetings for the participating hospitals were held online, hosted and led by TIPQC and state leaders. Participation in project huddles ranged from 6 to 13 hospitals (mean 9, median 10). An average of three team members per center participated in webinars. Each center presented a Leadership Report slide, including project charter with local aims; proposed, implemented, and tested changes; graphs of local measures; lessons learned including barriers and facilitators; recommendations/next steps; and team members. Frequent changes discussed on webinars included developing hospital breastfeeding policies, staff training, patient education, skin-to-skin, and rooming-in. Gaining buy-in from administration, physicians, nurses, and patients was also frequently discussed. Teams shared examples of patient education materials, staff training, policies, and process data from PDSA cycles. Celebrations and incentives used to facilitate staff training and process implementation were described. State leaders shared details of statewide opportunities for local teams, including World Breastfeeding Week, Big Latch On, and the statewide “Infant Care Summit” sponsored by Tennessee Department of Health. State and national initiatives, a Governor's proclamation for World Breastfeeding Week, and state and federal breastfeeding laws on breastfeeding in public and worksite lactation support were also highlighted.
Measures
The study population included mother–infant dyads based on TJC PC-05 specification, including allowable exclusions (discharged from neonatal intensive care unit [NICU], galactosemia, parenteral infusion, experienced death, length of stay >120 days, enrolled in clinical trial, and documented reason for not exclusively breastfeeding). 19 Hospitals reported TJC PC-05 using either the TJC-approved sampling strategy or the TJC-approved all-dyads strategy using data extracted from newborn charts. These data were validated by each institution's own processes (e.g., comparing chart review to TJC sampling). Reliability of implementation of evidence-based practices was measured using locally designed process implementation audits for each of the Ten Steps (numerator equals number of cases meeting the goal for each step and denominator equals number of cases examined). Most audits were done by chart review, although some were done by patient interview depending on each institution's resources and data extraction process. Some hospitals audited all process measures on an ongoing basis, whereas others periodically audited only a subset of process measures. Teams were encouraged to design and score clinical process audits to provide insights into their local practices. Hospitals were encouraged to share process data using the Leadership Report for the steps they were actively measuring during monthly webinars. Local process measures were aggregated based on each of the Ten Steps to follow aggregate improvement activity. Submitted data were checked for appropriate range and logic errors during data entry, and highlighted for correction in automated project reports available to local teams.
Data collection and analysis
QI data were collected and managed using REDCap electronic data capture. 25 A standardized project report including data logic checks, completeness/duplicate checks, and statistical process control graphs was developed for the project in R software for statistical computing and graphics, 26 and was made available on-demand to participating hospital teams through the REDCap interface.
Outcome data
Each hospital team entered TJC PC-05 data for 6 consecutive months to establish a baseline before introducing local process changes. The monthly percentage of exclusively breast milk-fed infants was analyzed using statistical process control p-charts. For state-level aggregate charts with >1,000 cases per month, overdispersion was checked by calculating sigma for z-values, and control limits were corrected to avoid overdispersion where sigma >1 using Laney's method. 27
Process data
Locally devised and defined process audits proved difficult to aggregate at the state level, as locally derived operational definitions evolved with improved understanding of local barriers. Sample size varied with auditing approach; hospitals auditing electronic medical record (EMR) data generated larger cohorts, whereas hospitals implementing direct behavioral observation strategies generated smaller cohorts. Accordingly, local compliance was reported as number achieving the goal for each step divided by number observed for each month in the automated report, and teams were coached to construct local process data run-charts. Local process data were aggregated as monthly scatter plots of reported compliance percentages for discussion in statewide webinars and meetings. No statistical process control analysis was attempted given intercenter variation in approach and operational definition.
Ethical considerations
Since well-established evidence-based guidelines were implemented, no specific consent was required beyond local standard of consent for treatment. The overall collaborative initiative was reviewed by Vanderbilt University's IRB and deemed nonresearch clinical QI. Each participating hospital team obtained independent local review by their IRB or quality council. Participation was open to all delivery hospitals in Tennessee. No participating team or author declared any financial conflict of interest.
Results
Participation
Thirteen birth hospitals joined the project, accounting for 47% of Tennessee live births. Participating hospitals were widely distributed with almost half of the hospitals located in either the Mississippi River Delta or Appalachia. In total, 10 of the 13 hospitals were located in counties that are >25% rural and/or were located in the Mississippi River Delta or Appalachia. 28 Hospitals further differed in size, ownership model, delivery volume, and payer mix. Percentage of total charges derived from newborn care ranged from 0.21% to 6.42%29,30 (Table 1). All 13 participating hospitals participated in the state-wide kick off, with an average of four local team members attending per center.
Fraction of Medicaid net inpatient revenue to total net inpatient revenue.
Fraction of newborn charges to total inpatient charges.
From U.S. Census Bureau.
C, church; E, east; GH, government hospital district or authority; GL, government local; M, middle; NE, northeast; NP, not for profit; O, other; P, private; PRC, Perinatal Regional Center; Prop, proprietary; SE, southeast; W, west.
Outcome measures
Data were submitted on 31,183 mother–infant dyads from August 1, 2012 to December 31, 2013. An aggregate “special cause” (statistically significant change from baseline using statistical process control methodology, based on a priori established thresholds) improvement in breastfeeding exclusivity was achieved, increasing baseline TJC PC-05 from 37.1% during the baseline period to 41.2%, a relative 11.1% increase (Fig. 1). This increase was realized 2 months after hospitals began implementing evidenced-based practices with PDSA tests of change, and remained stable for the remaining 9 months. Baseline TJC PC-05 varied from 5% to 55% across 11 hospitals reporting baseline data. Five hospitals subsequently achieved >5 consecutive months above their baseline. One center that successfully increased for 11 consecutive months submitted no process data. “Special cause” aggregate improvement in TJC PC-05 was also noted after excluding the three hospitals in the collaborative that were also pursuing BFHI designation, increasing from 33.2% at baseline to 35.8%, a relative increase of 7.8% (Fig. 2).
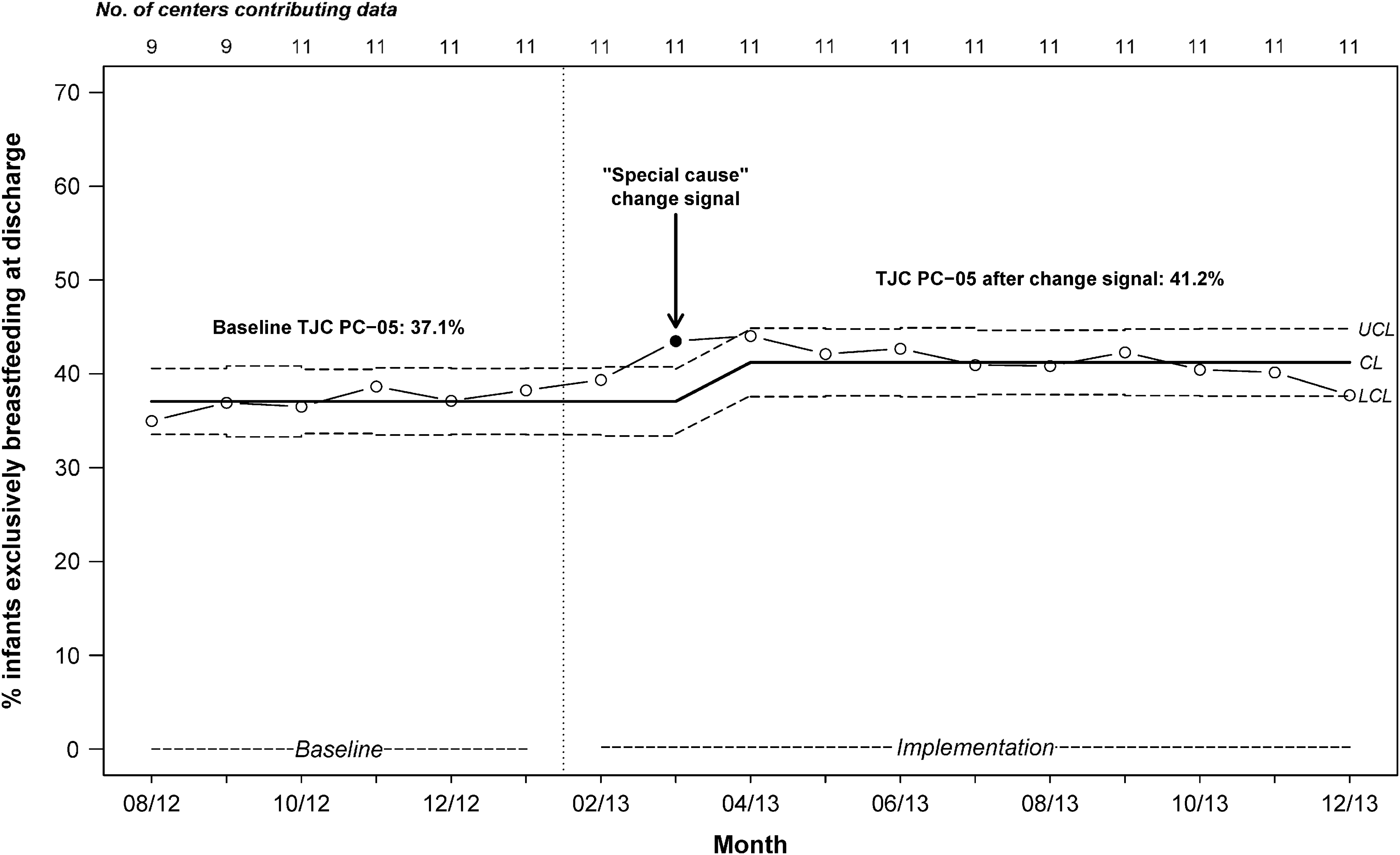
p-chart of monthly percentage of infants exclusively breastfeeding at discharge, using aggregate TJC PC-05 data from all participating hospitals. Solid black dot: “special cause” change signal, a statistically significant improvement from baseline TJC PC-05; CL: mean TJC PC-05, note CL is recalculated after “special cause” change signal on 3/13 reflecting new mean TJC PC-05 after “special cause” improvement. Note month-to-month variation within UCL and LCL does not achieve statistical significance. CL, control limit; LCL, lower control limits; UCL, upper control limits.
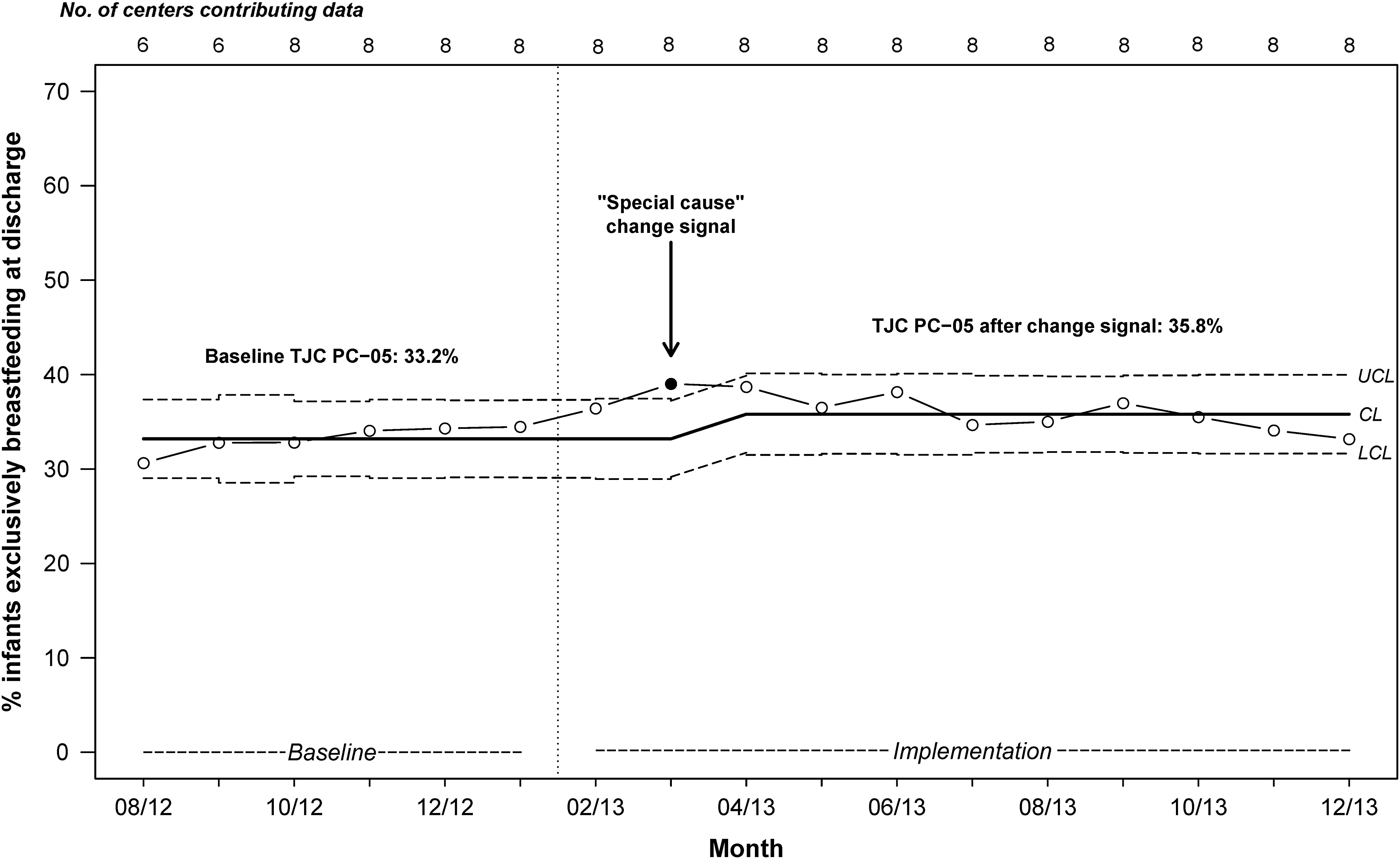
p-chart of monthly percentage of infants exclusively breastfeeding at discharge, using aggregate TJC PC-05 data from participating hospitals not pursuing Baby Friendly designation. Solid black dot: “special cause” change signal, a statistically significant improvement from baseline TJC PC-05; CL: mean TJC PC-05, note CL is recalculated after “special cause” change signal on 3/13 reflecting new mean TJC PC-05 after “special cause” improvement. Note month-to-month variation within UCL and LCL does not achieve statistical significance.
Process measures
Local practice changes associated with aggregate improvement were challenging to summarize given the small number of hospitals, variation in Ten Steps audit strategy, and deidentification requirements of data use agreements. However, 10 of 13 hospitals successfully submitted process data in conjunction with a local test of change, 7 of which achieved high reliability (defined as >90%) on at least one step as entered to REDCap by step number. Fewer than half reported process audits on >5 of the Ten Steps and only 2 achieved high-reliability implementation on >5 of the Ten Steps (Table 2). No correlation was possible between number of implemented steps and rates of exclusive breastfeeding because submission of process audit data was not sufficiently consistent across all centers to support a robust analysis of association.
Although center level analysis of association with changes in TJC PC-05 was not possible, differences were apparent in the number of attempted steps as noted in Table 3. Most teams worked systematically to help mothers initiate breastfeeding within the first hour after birth (Step 4), but few worked to eliminate pacifiers or artificial nipples for breastfeeding infants (Step 9). High-reliability implementation of Step 6, giving infants no food or drink other than breast milk unless medically indicated, was accomplished by only one hospital. An example of a locally designed audit was a rooming-in (Step 7) audit that required notation on the baby's bedside chart of his/her location during the entire day. Another example was auditing skin-to-skin care after delivery (Step 4) by recording this in the electronic medical record on all patients.
PDSA, Plan-Do-Study-Act.
Barriers
Reported barriers to data submission systematically collected in Leadership Reports and huddles included hospital reluctance to release TJC data to bedside improvement teams, loss of designated personnel to extract data, volunteer fatigue regarding data extraction, and insufficient time to obtain data or perform PDSA tests of change. Restrictive data use agreements limited the ability to identify teams needing help and those excelling.
Other observed barriers included lack of physician support, especially regarding rounding procedures to enhance rooming-in, and using only medically indicated supplementation; staff members' personal experiences with breastfeeding; lack of trained lactation expertise available 24/7, and lack of opportunities and funding to increase lactation staff; financial and time burden required to train all staff on breastfeeding policies; inability to educate moms prenatally in many hospitals; and increased staffing requirements to assist skin-to-skin after vaginal and Cesarean deliveries. Community culture was consistently highlighted as a significant barrier, especially regarding prenatal intention for any breastfeeding, maternal request to both breastfeed and formula feed, family request to keep babies in the nursery, maternal request for supplementation, and family request for pacifiers. Resource allocation for QI work was also a barrier for many teams.
Successes
Qualitative successes were also collected systematically through Leadership Reports and shared in huddles, and at regional and annual meetings. Teams shared what worked well and how they solved challenges to help other teams struggling with the same issues. For example, one team created a policy requiring physicians to round in the rooms, which enhanced efforts for rooming-in. Another team created a “Stop Sign” on the formula cabinet to remind staff to educate families before providing requested formula for nonmedically indicated reasons. Another team initiated education in obstetrician offices, and one team created and distributed a physician packet with breastfeeding information and resources, to prepare physicians for hospital QI work and to better support postpartum mothers with resources for breastfeeding expertise in the community.
Discussion
Through a statewide QI collaborative initiative, aggregate breastfeeding exclusivity at discharge increased by 11.1% from August 2012 to December 2013, in hospitals responsible for 47% of Tennessee live births. Participating hospitals accounted for <20% of Tennessee birthing hospitals. Nonparticipating hospitals were predominantly smaller and rural. Diverse facilities serving patients from Appalachia to the Mississippi Delta Regions reported numerous challenges but frequent successes in testing and implementing the Ten Steps to Successful Breastfeeding in maternity care practices. Geographically dispersed hospitals with different resources and commitment levels to breastfeeding promotion were able to improve breastfeeding initiation and exclusivity at discharge. Some facilities pursued formal BFHI designation and attempted all Ten Steps, but most worked on only a subset. Importantly, significant aggregate improvement in TJC PC-05 was observed even in hospitals working on a limited number of steps.
Concurrent validation of self-reported QI data was limited, but parallel data streams suggest improvement in state breastfeeding rates during the project period. Tennessee breastfeeding initiation rates rose over the project period, from 64.4% at inception to 71.1% at closure. 31 Similarly, Tennessee's composite mPINC score rose from 62 (of 100) in 2011 to 67 in 2013.32,33 Discerning project effect from a “rising tide effect” is a potential limitation, given multiple contemporaneous breastfeeding promotion and support initiatives and the absence of a nonparticipant control group.6.34 However, direct participation in national breastfeeding support initiatives by Tennessee hospitals was limited, with only two hospitals participating in the concurrent Best Fed Beginnings project. 35 Of note, improvement in Tennessee was demonstrated in hospitals that participated in both the TIPQC and Best Fed Beginnings project, as well as in hospitals that only participated in the TIPQC project, suggesting that the State level project successfully engaged and facilitated improvements in a broader segment of the State population. Even those hospitals unable to commit to working toward full implementation of the Ten Steps required for Baby Friendly designation were still able to achieve an aggregate increase in exclusive breastfeeding with this statewide collaborative, highlighting the importance of engaging hospitals at various levels of readiness to improve maternity care practices.
During the TIPQC project period, other collaborative initiatives were improving maternity care practices focused on attaining BFHI designation, whereas others with special recognition programs promoted variable enrollment criteria and improvement aims. The TIPQC Breastfeeding Project was distinct from other maternity care practice initiatives in several ways. Tennessee included participation of both high- and low-commitment hospitals from the Mississippi Delta to Appalachia, and still demonstrated an aggregate improvement in TJC PC-05. No external funding was provided to project teams, who were supported only by their local administrations. Teams were allowed to choose which of the Ten Steps to work on—their local “low-hanging fruit”—however, they were encouraged to achieve high reliability implementation of at least five steps, to enhance the documented dose–response effect. Although audits were recommended for each step, teams were able to create their own audit mechanisms, rather than use designated audit templates. There was no designation or recognition associated with this project, beyond listing as a participant on the TIPQC website. The most novel difference in the TIPQC breastfeeding project was the approach to “do what you can” while measuring TJC PC-05, in diverse hospitals, some with incredibly low breastfeeding rates.
With this simple and pragmatic approach, most hospitals were able to submit process data on Step 4 (Table 3), breastfeeding within the first hour, citing during huddles that this step was something they could accomplish within their local setting. They were encouraged by each other in the collaborative regarding techniques, challenges, and successes for implementation. Although no balancing measures were required for the project, safety while skin-to-skin was a key component of each hospital's implementation plan for Step 4 and discussed during huddles.
Limitations include the small number of participating hospitals, yet participants cared for a substantial proportion of live births, thus highlighting the need to engage smaller volume hospitals. Based on data from other multicenter efforts, greater aggregate improvements in breastfeeding exclusivity in Tennessee might be achieved as more hospitals achieve high-reliability implementation of more of the Ten Steps.11,12 Although hospitals were able to capture their exclusive breastfeeding rates (TJC PC-05), the implementation of at least five of the Ten Steps, with accompanying locally defined process audits, proved challenging for many participants. Many hospitals were not able to comply with this suggestion, and as a result correlation between the number of reliably implemented steps cannot be tied to observed increase in exclusive breastfeeding. These barriers may partially explain the lack of continued increase in TJC PC-05 over the project timeline. Validation of case selection, completeness of enrollment of identified population, and secondary validation of outcome or process data by independent observers also exceeded available project resources. Participants also noted substantial challenges obtaining institutional resources for QI work on well mother–infant dyads as newborns represent a tiny fraction of most hospitals' business (0.21–6.42%) (Table 1). However, cost savings from improved breastfeeding rates may help encourage support of future similar QI projects. 36 Resource limitations also restricted systematic data capture describing barriers to implementation, including cultural and socioeconomic factors differentially impacting facilities. Racial and ethnic diversity across Tennessee was not addressed in data collected in this project despite large existing disparities in breastfeeding; however, implementation of the Ten Steps has been recommended to reduce racial and ethnic disparities in breastfeeding rates 37 and should be explored in future projects.
Many lessons were learned during this first wave of hospital breastfeeding promotion in Tennessee. How to work as a functioning team, internally and across the state, was a definite highlight. Teams were excited to learn from each other in a collaborative context and appreciated sharing what did or did not work. Encouragement was another highlight; one hospital did not plan to participate at all due to extremely low baseline breastfeeding rates, but learned even small steps make a difference. The importance of culture change among staff, physicians, and families was another key lesson. Focusing on improved practices without pressure to reach a designation or recognition status helped motivate hospitals ready for small steps, who had opted not to participate in initiatives requiring a commitment to implementation of all Ten Steps. These lessons helped inform a subsequent QI project (termed “Wave 2”), bringing in more hospitals and highlighting successes of the original teams. We hypothesize that experienced teams from this project might be effective mentors in future State-wide improvement efforts that feature a greater emphasis on consistent data-driven process implementation for the Ten Steps.
In summary, this large-scale QI collaborative project provides an important proof-of-principle, as it was a low resource initiative open to all comers, and associated with increased breastfeeding exclusivity at discharge among a diverse group of Tennessee hospitals. Teams achieved improvement without financial remuneration or special recognition, which suggests that this work can be replicated in other settings. Further opportunities for improvement include identifying barriers and facilitators to implement evidence-based practice, investigating socioeconomic and cultural determinants of breastfeeding, and involving hospital leadership. 38 Additional work to understand and mitigate hospital barriers to full implementation of breastfeeding supportive practices is urgently needed.
Footnotes
Acknowledgments
The authors would like to thank the following people and hospitals for their support and participation in this project. This project was funded under a Grant Contract with the State of Tennessee through the Tennessee Department of Health, and was supported by federal funds from CFDA 93.778 through the Bureau of TennCare. The authors would also like to thank Dr. M.K. Key for her efforts in project organization and training and the Tennessee Department of Health, and especially Drs. Michael Warren and John Dreyzehner for their support. The authors would also like to thank the regional and state breastfeeding coalitions for promoting the project, and helping with breastfeeding resource development. Most of all the authors would like to thank the teams at all the participating hospitals and their staff for working diligently to improve breastfeeding friendly practices, and all the mothers, babies, and families in Tennessee.
Pilot hospitals: Baptist Memorial Hospital for Women; Baptist Tipton Hospital; Methodist Germantown Hospital; Methodist South Hospital; The Regional Medical Center; Monroe Carell Jr. Children's Hospital at Vanderbilt; Mountain States Health Alliance/Johnson City Medical Center.
Participating hospitals for Wave 1: Baptist Memorial Hospital for Women, Centennial Women's and Children's Hospital Tristar, Erlanger Medical Center, Johnson City Medical Center, Maury Regional Hospital, Methodist Le Bonheur Germantown Hospital, Methodist South Hospital, Monroe Carell Jr. Children's Hospital at Vanderbilt, Northcrest Hospital, The Regional Medical Center, St. Thomas Midtown, Sumner Regional Medical Center, University of Tennessee Medical Center, Knoxville.
Preliminary work on this project was presented as an abstract at the 2013 AAP NCE Section on Breastfeeding meeting, and the 2013 Academy of Breastfeeding Meeting.
Disclosure Statement
The authors have no financial relationships relevant to this article to disclose.