
Abstract
Abstract
Objective:
Mothers of premature infants confront barriers to coming to volume (CTV; ≥500 mL/day mother's own milk [MOM] by postpartum day 14), a strong predictor of continued MOM provision at neonatal intensive care unit (NICU) discharge. We sought to determine concentrations of secretory activation biomarkers (MOM sodium, total protein, lactose, and citrate) during the first 14 postpartum days and to describe relationships among these biomarkers, pumped MOM volume, CTV, and pumping frequency.
Study Design:
This descriptive observational study collected serial MOM samples, pumped MOM volume, and pumping frequency during the first 14 postpartum days in 16 breast pump-dependent mothers who delivered <33 weeks gestation. Daily biomarker concentrations were compared to published normal values for mothers of term infants. Relationships among biomarkers, pumped MOM volume, and pumping frequency were determined.
Results:
On postpartum day 5, only 40% of MOM samples revealed normal concentrations of all four biomarkers, and normalcy was not maintained throughout the first 14 days. All eight mothers (50%) who achieved CTV had normal concentrations for four biomarkers at 5.4 ± 3.5 days postpartum and had more cumulative pumping sessions by day 5 (p = 0.03). A dose–response relationship between number of normal biomarkers and pumped MOM volume was demonstrated for postpartum days 3 (p = 0.01) and 5 (p = 0.04).
Conclusion:
Secretory activation is delayed in mothers who deliver prematurely and is closely tied to CTV, MOM volume, and pumping frequency. MOM biomarkers hold promise as objective research outcome measures and for point-of-care testing to identify and proactively manage mothers at risk for compromised lactation.
Introduction
H
In a recent study of 402 mothers of very low birthweight infants, 10 we reported that a significant predictor of continued provision of MOM through to NICU discharge was the mother's achievement of coming to volume (CTV; pumped MOM volume ≥500 mL per day) by postpartum day 14. 3 These and similar findings from studies of breast pump-dependent mothers of premature infants suggest a critical postpartum window during which the mammary gland is programmed optimally for long-term MOM synthesis.11–15 These data imply that evidence-based interventions and resources should be prioritized during the first 2 weeks postpartum to prevent low MOM volume later in NICU hospitalization. However, an imperative first step is to understand the biology, physiology, and behavioral mechanisms involved in CTV for breast pump-dependent mothers of premature infants.
Secretory activation (lactogenesis II; MOM “coming in”) is a well-defined process, by which the mammary gland transitions from preparing for lactation to actually secreting copious MOM, and represents the first step in CTV. 3 In brief, upon delivery of the placenta, the progesterone-inhibition of prolactin is removed, permitting prolactin to catalyze closure of open mammary epithelium paracellular pathways (PCPs). During PCP closure, MOM sodium and total protein decrease, while lactose and citrate increase, reflecting tight junction formation of the blood–breast barrier.16–19 In combination, these MOM compositional changes serve as biomarkers of PCP closure and secretory activation. 20 Although these biomarkers were described decades ago in healthy populations, only 1 study of 22 mothers of infants born between 31 and 35 weeks of gestation has measured them in an at-risk population. 21
Therefore, the primary purpose of this pilot study was to describe the concentrations and patterning of MOM biomarkers of PCP closure in mothers of premature infants during the first 14 postpartum days and to characterize the relationships among these MOM biomarker patterns, pumped MOM volume, and pumping frequency during the same period. We speculated that mothers with a greater number of normal MOM biomarkers would have greater pumped MOM volume and pumping frequency and be more likely to experience CTV than mothers with fewer normal and/or delayed MOM biomarkers.
Materials and Methods
This pilot study enrolled 16 mothers of premature infants who were admitted to a level III, urban NICU in the United States between October 2016 and March 2017. Data were collected during the first 14 postpartum days.
Sample
All mothers who met inclusion criteria were invited to participate and were approached antepartum or postpartum, depending upon the timing of maternal admission to the hospital. Mothers were approached within the first 24 hours postdelivery unless they were too medically unstable to ethically provide informed consent, or were physically unavailable due to delivery at a referral hospital. Inclusion criteria were as follows: gestation at delivery <33 weeks; decision to initiate lactation; refusal of hormonal contraception for 14 days postpartum; absence of maternal conditions or treatments that could impact lactation such as galactagogue use; English or Spanish speaking; singleton infant without severe congenital anomalies; and expected to survive. Mothers who had already experienced MOM coming in were deemed ineligible.
Of 20 mothers approached, 16 enrolled. This study was approved by the institutional review board, and written consent was obtained for mothers and their infants. Evidence-based lactation care emphasizing early and frequent double electric breast pump use was provided independent of study enrollment by NICU breastfeeding peer counselors and lactation consultants; pump use was encouraged over hand expression.2,3
Design
This was a nonrandomized, observational study that collected serial data during the first 14 postpartum days. Researchers who collected and managed clinical data were masked to laboratory measures of MOM biomarkers. Similarly, researchers who measured MOM biomarkers were masked to clinical data, including maternal prepregnancy, pregnancy and delivery risk factors, volume of pumped MOM, and the frequency of breast pump use.
Measures
For this pilot study, the following measures were collected: maternal and infant characteristics, MOM biomarkers of secretory activation, pumped MOM volume, and pumping frequency.
Maternal and infant characteristics
Maternal characteristics were collected from electronic medical records (EMR) for health characteristics, including age, parity, and health complications. Information about maternal eligibility for WIC benefits (Women, Infants, and Children Supplemental Security Income; household income ≤185% of poverty threshold), 22 educational attainment, and prepregnancy weight were acquired by questionnaire. Infant characteristics were collected from the EMR.
Pumped MOM volume
Mothers were provided with preweighed (nearest 0.1 g) MOM storage containers. When filled MOM storage containers were brought to the NICU, each container was weighed (nearest 0.1 g) on a scientific scale (Tanita, Japan) that remained in the infant's room throughout the study. A team of NICU bedside nurses who had been trained in the weighing and recording procedures performed these measures under research team supervision. MOM volume was calculated by subtracting the prefill container weight from the filled container weight (g). The MOM weights were converted to volume using 1 g weight = 1 mL volume. Although the density of MOM is slightly greater than water, this difference is miniscule for the small volumes of MOM measured, so MOM weights are considered an accurate standard for measuring MOM volume. 23
Pumping frequency
Mothers were instructed to maintain pumping logs (My Mom Pumps for Me!™), in which they recorded pumping start and end times for each pumping session. 24 Daily and cumulative mean and median pumping frequencies were determined by combining these maternal records with pumping times and dates written on weighed MOM bottles because some maternal pumping records were incomplete. If no pumping log or weighed MOM data were available, it was assumed that the mother had not pumped that day.
MOM biomarkers of secretory activation
Collection of MOM samples
As per clinical NICU protocol, mothers were instructed to label their MOM storage containers with the date and time that the pumped MOM was collected. All the filled containers were brought to the NICU for storage in temperature-controlled industrial refrigerators and freezers. During the study period, the research team collected 1.8 mL of MOM from containers twice daily, ∼12 hours apart for MOM biomarker analysis. For ethical purposes, samples were not collected when all the day's pumped MOM was needed for infant feedings. Each MOM sample was placed in a bar-coded cryocontainer, labeled with study ID, time and date, and stored at −20°C until all samples from all 16 mothers (n = 331) were shipped to the University of Western Australia (UWA) via commercial carrier, which monitored the temperature and integrity of MOM samples throughout transit.
Laboratory analyses of MOM biomarkers
For analysis of MOM sodium concentration, selective ion testing, which has previously been validated with flame photometry in milk and has been used in multiple human milk publications, was performed. 25 Frozen samples were thawed for 1 hour at 37°C, hand mixed for 15 seconds and subjected to three top-to-bottom inversions. Then, 300 μL was pipetted onto a sodium (B-722) ion selective electrode sensor pad (Horiba, Japan), for which calibration had been previously conducted according to manufacturer's recommendations. Values were recorded after digital display results had stabilized for 15 seconds.
The sensor pad was rinsed with double deionized water and wiped with disposable delicate task wipers (KimWipes, Kimberly-Clark Worldwide) before performing the next measurement. All samples were performed and recorded in duplicate; samples were rerun if the two results differed by more than 10%. The mean of the two measurements was used for the final value.
For analysis of total protein, lactose, and citrate concentrations, frozen samples were thawed and then shaken with Intelli-Mixer (RM-2, ELMI Ltd., Riga, Latvia) using UU mode for 15 seconds at 50 rpm, followed by three top-to-bottom inversions. Duplicate samples were withdrawn into glass capillary tubes (tube 41A2502; Kimble-Chase), one end sealed (Cha-Seal 43510; Kimble-Chase), and spun for 10 minutes in a flat-bed centrifuge (CEN 96221; Phoenix Scientific Industries Ltd.). The fat content was measured (modified creamatocrit method; Creamatocrit Plus™ Medela, AG),26,27 after which the capillary tubes were cut, and the skimmed MOM portion was used to measure total protein, lactose, and citrate.
Total protein content was determined by the modified Bradford method using Bio-Rad protein assay dye reagent concentrate (500-006; Bio-Rad Laboratories). 28 The human milk protein standard for the assay was determined by the Kjeldahl method, as described by Atwood and Hartmann, 29 with detection limit of 0.035 g/L and interassay coefficient of variation (CV) of 5.9%. The recovery of a known amount of protein added to the milk samples was 100.4% ± 3.7%.
Lactose concentration was determined by enzymatic spectrophotometric assay, a method previously validated with high performance liquid chromatography, with detection limit of 2.02 g/L and interassay CV of 6.1%.30–32 The recovery of a known amount of lactose added to the milk samples was 98.8% ± 1.4%. Citrate concentration was determined by enzymatic spectrophotometric assay 30 with detection limit of 0.40 g/L and interassay CV of 15%. The recovery of a known amount of citrate added to the milk samples was 98.8% ± 4.3%.
Data analysis
All clinical and laboratory data were entered into Excel (Microsoft, Washington). Descriptive statistics were used to summarize sample characteristics, pumped MOM volume, and pumping frequencies. For each postpartum calendar day, mean daily values for each biomarker were calculated by averaging results from the two daily MOM samples when more than one daily sample was available. These mean daily values were compared with previously published reference ranges (mean ±3 SD) for mothers of healthy term infants with uncompromised lactation as follows: sodium (1.20–23.0 mM); total protein (9.2–31.7 g/L); lactose (100–223 mM); and citrate (2.24–6.40 mM).21,30,33 Descriptive statistics were used to determine the number of MOM biomarkers within these reference ranges (hereafter referred to as “normal” values) for each mother, as well as the percentage of mothers with 0, 1, 2, 3, or 4 normal biomarkers for each postpartum day.
Statistical analyses and graphic displays of serial biomarker concentrations and pumped MOM volume were carried out with RStudio 0.99.896 34 using package nlme for mixed effect modelling 35 and multcomp 36 for Tukey HSD comparison. For the comparison of milk volumes on either day 3 or 5 postpartum, the number of normal biomarkers was used as the fixed effect and the individual mother as the random effect. Post hoc comparisons using the Tukey HSD test were used to compare the mean milk volume between mothers with 1–4 normal biomarkers.
Tests for normality were performed, and when data were normally distributed, results were expressed as mean ± SD unless stated otherwise and non-normal data were expressed as median and interquartile range (IQR). Group comparisons were conducted using t tests if data were normally distributed and with Mann–Whitney u tests if non-normal. Differences were considered to be statistically significant if p < 0.05. Serial patterning of the four biomarkers and their relationship to pumped MOM volume were determined by constructing 14-day graphs of these variables for each mother. For these graphs, the daily biomarkers were depicted as a proportion of the maximum value by dividing each day's absolute concentration by the maximum concentration of that biomarker observed over the 14-day period in that mother, then multiplying by 100 [(observed daily value/maximum 14-day value) × 100].
Results
Characteristics of the sample
Characteristics of the mothers and their infants are summarized in Table 1. Noteworthy in this primarily minority, low-income sample is that nearly all (88%) mothers had at least one comorbidity in addition to preterm birth, 75% were placed on antenatal bed rest, and 66.6% were overweight or obese.
MOM biomarkers of secretory activation
In total, 331 MOM samples were analyzed, reflecting a mean of 20.8 samples per mother (range 1–28). Not all mothers provided sufficient MOM for twice-daily sampling because some mothers were unable to remove any MOM in the first days postpartum and because the study always prioritized MOM for infant feeding when volumes were low. Of 16 mothers, 4 (25%), 8 (50%), and 10 (62.5%) provided MOM samples for analysis on postpartum days 1, 2, and 3, respectively. The 6 (37.5%) mothers who provided their first MOM samples after day 3 (range 4–8 days) had small volumes of MOM on the day before samples being obtained that was prioritized for infant feedings.
Figure 1 illustrates patterning of the 4 MOM biomarkers for 3 of the 16 mothers who exemplified the range of patterns seen in the cohort. The graphs reveal postpartum directional trends with overall decreases in sodium and total protein and increases in lactose and citrate. However, significant between-mother variability in the timing, slope, and stability of these directional changes was noted, indicating delayed or incomplete PCP closure (patterns B and C). In the cohort as a whole, of the four biomarkers, citrate normalized first (median [IQR] 3 [2.75–4] days), followed by lactose (3 [3–4] days), sodium (3.5 [2.75–5] days), and total protein (4 [4–9] days).
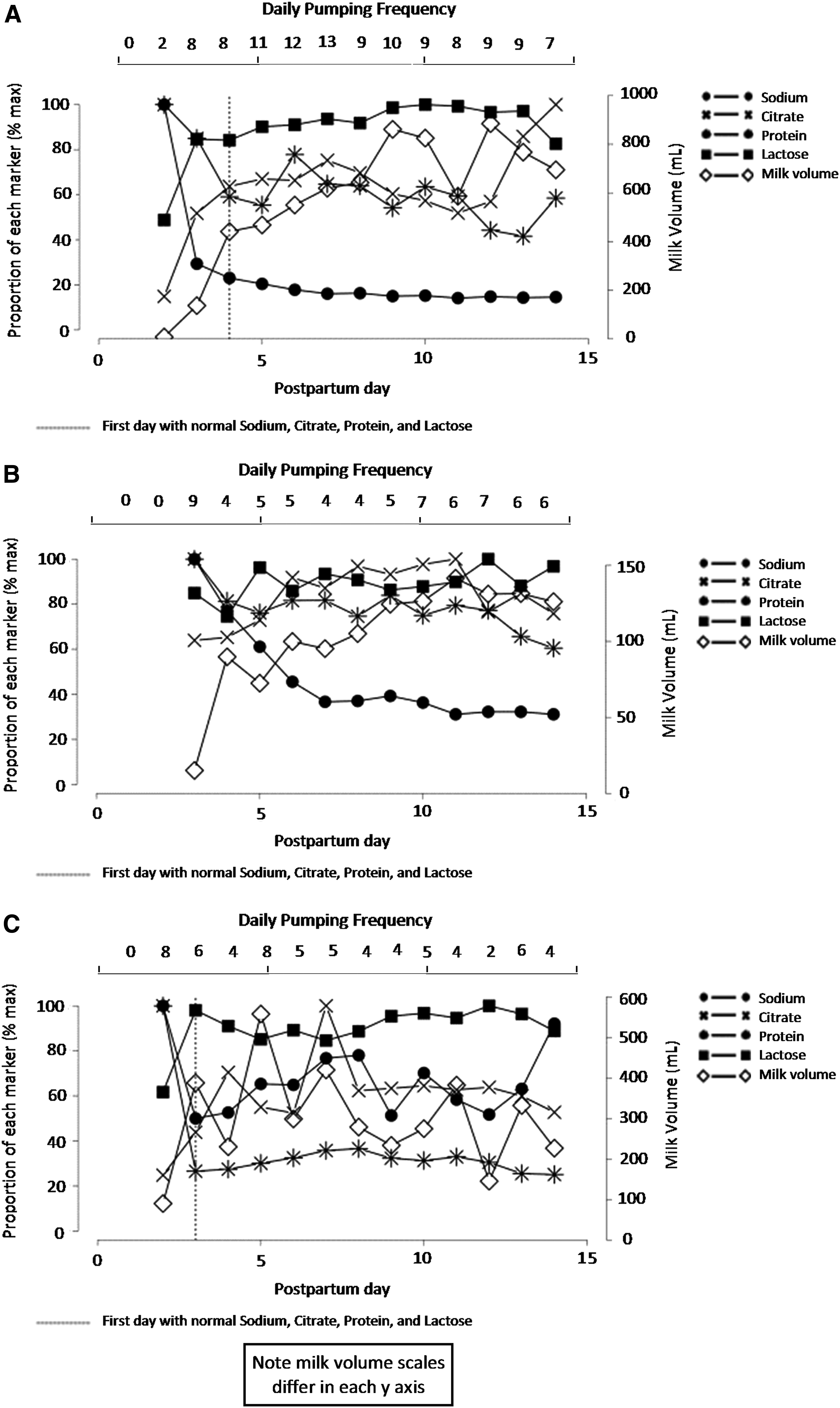
Patterns of MOM Biomarkers and Pumped MOM Volume for Three Subjects.
Table 2 summarizes the percentages of mothers with normal concentrations of 0, 1, 2, 3, and 4 MOM biomarkers for each postpartum day. The highest percentage (40%) of mothers with normal concentrations for all four MOM biomarkers occurred on postpartum day 5. Over the 14-day study, 14 of the 16 mothers (87.5%) had at least 1 MOM sample with normal concentrations for all 4 biomarkers, and on average, this MOM sample was collected on postpartum day 6.7 ± 3.5. However, having normal concentrations for all MOM biomarkers for a single MOM sample did not mean that subsequent samples remained normal. All the abovementioned 14 mothers had subsequent MOM samples with fewer than 4 normal biomarkers, and the remaining 2 mothers never had a MOM sample with normal concentrations of all 4 biomarkers.
Pumped MOM volume and pumping frequency
The pumped MOM volumes and pumping frequencies (Table 3) reveal a wide range of daily and cumulative values. The median postpartum day of pumping initiation was day 1.5 (range 1–7) with 50% of mothers starting on day 1 (day of delivery). All mothers intended to pump for ≥2 weeks at study entry, and 87.5% (n = 14) of mothers met this personal goal, whereas the remaining two mothers pumped for only 4 and 12 days.
Median, IQR, and Mann–Whitney test results reported if non-normal data.
n = 6, as two mothers who did not achieve CTV never had normal biomarkers.
One mother started pumping on day 7, accounting for the low end of the range.
Chi-square test results.
IQR, interquartile range; CTV, coming to volume; MOM, mother's own milk.
Of 16 mothers, 8 (50%) achieved CTV, and these eight mothers demonstrated higher mean daily pumping frequencies for the 14 day study, as well as higher cumulative pumping frequencies in the first five postpartum days compared with mothers who did not achieve CTV (p = 0.03 and p < 0.001, respectively). Mothers who pumped on average at least five times daily throughout the study (n = 7) were likely to achieve CTV (85.7%), whereas only 22.2% of mothers who pumped fewer than five times daily (n = 9) achieved CTV (p = 0.01).
MOM biomarkers and pumped MOM volume
On postpartum day 3, mothers with four normal biomarkers had higher mean milk volumes than those with two normal biomarkers (421 mL vs. 15 mL, p = 0.017). On postpartum day 5, mothers with four normal biomarkers had higher mean milk volumes compared to those with one normal biomarker (577 mL vs. 65 mL, p = 0.041). Even with small sample sizes for this pilot study, these findings suggest a dose–response relationship between the number of normal MOM biomarkers and pumped MOM volume. All eight mothers who achieved CTV (Table 3) had four normal MOM biomarkers at a median of 4 days postpartum. In contrast, the eight mothers who did not achieve CTV either had four normal biomarkers later in the postpartum period (median 9 days) or never had four normal biomarkers in the same MOM sample (n = 2).
Discussion
To our knowledge, this is the first study to measure multiple MOM biomarkers, pumped MOM volume, and pumping frequency through postpartum day 14 in breast pump-dependent mothers of hospitalized premature infants. Our findings from this pilot study reveal that although the directionality of MOM biomarkers conforms to normative data from mothers of healthy breastfeeding infants, there is evidence of delayed or impaired secretory activation in this at-risk population.
A similar conclusion was reached in the only other study of MOM biomarkers in 22 mothers who delivered prematurely, but at a later gestation than our sample (31–35 weeks vs. 26–32 weeks) and for whom data were collected only on postpartum day 5. 21 On postpartum day 5, our data reveal more mothers with normal MOM biomarkers (40% vs. 18%) and greater pumped MOM volume (364 mL vs. 180 mL) than did Cregan et al. 21 While the percentage of mothers with normal citrate concentration at day 5 was comparable for our findings and those of Cregan, respectively (73.3% vs. 77.3%), the percentage of mothers with normal sodium (86.7% vs. 31.8%), total protein (60% vs. 86.4%), and lactose (86.7% vs. 63.6%) concentrations differed in our study compared to Cregan et al. 21
Cregan recommended larger studies with serial measurement of MOM biomarkers in mothers of premature infants to determine whether secretory activation and subsequent lactation potential are impaired or merely delayed. 21 Indeed, our measurement of MOM biomarkers through postpartum day 14 reveals dynamic activity in the closure of PCPs not previously reported in humans except during active mastitis. 37 Specifically, 40% of the mothers in our study had four normal biomarkers on postpartum day 5, but over the next 14 days, this percentage decreased, a fact that would have gone unrecognized if MOM sampling had ended earlier. These findings suggest that mothers who are thought to have successfully completed secretory activation and CTV may remain at risk of early MOM volume problems and warrant careful monitoring at least through to the 14 postpartum day benchmark.
While this pilot study does not have adequate power to investigate the factors that may influence closure of PCPs and CTV, these early findings suggest that both biology and behavior, especially the frequency of breast pump use, play an important role in these processes. It is noteworthy that the 50% of mothers who successfully achieved CTV in our study had both higher cumulative number of pumping sessions by day 5 and higher mean number of pumping sessions overall, and CTV was strongly associated with earlier normal concentrations of all four biomarkers in this subpopulation.
While we speculate that closure of PCPs and CTV may be modifiable with improved pumping behaviors, this small study does not permit thorough examination of unmodifiable risk factors related to premature birth and maternal and infant health that influence pumping frequency. Understanding the interaction of these modifiable and unmodifiable risk factors and their relationship to PCP closure and CTV remains a high priority research area, and a future larger study is planned to investigate these factors in greater detail.
Finally, we found significant relationships between the number of normal MOM biomarkers on days 3 and 5 postpartum and daily pumped MOM volume, echoing Cregan's day 5 findings. 21 One previous study in breastfeeding mothers with term infants reported that an abnormal elevation of a single MOM biomarker (sodium-to-potassium ratio) from a sample collected on postpartum day 7 was associated with the mothers' concurrent perceptions of insufficient MOM volume (OR 2.7). 38 In the Murase et al. study, early unplanned weaning was highest in mothers with abnormally elevated concentrations of this MOM biomarker, underscoring the importance of understanding the relationship between the biochemistry of PCP closure and delayed and/or impaired lactation in at-risk populations. 38
More data are needed to determine which biomarker(s) is most predictive of pumped MOM volume and CTV in mothers of premature infants. Similar to Cregan, we found that citrate, a biomarker known for over 40 years to be associated with the onset of copious milk production in dairy animals and humans, normalized before sodium in this preterm population.21,39 Larger studies are needed to determine if sodium or sodium–potassium ratio or citrate, either individually or in combination, would be the optimal marker(s) on which to base clinical decisions in this population.
Study strengths include our twice daily MOM biomarker sampling and the meticulous measurement of pumped MOM volume over a relatively long postpartum period in a diverse population of breast pump-dependent mothers of premature infants. This pilot study is limited by a small sample size and a likely underrecording of pumping frequency by mothers, especially during the first postpartum days when they were often ill themselves and coping with the NICU admission of their premature infant. An unavoidable limitation was the prioritization of early MOM for infant feeding, reducing the number of MOM samples available for biomarker analysis in the first days postpartum.
We also acknowledge that our biomarker measurement methods for sodium and lactose, while acceptable and previously validated, are not the most widely used in this field.25,30–32 However, should these biomarkers be found to be robust predictors of future MOM volume, it would be ideal to use a test that is available to both researchers and clinicians, which is true, for example, of selective ion testing for sodium but not of the gold standard flame photometry.
Conclusion
In summary, this pilot study reports abnormal and dynamic concentration of MOM biomarkers of PCP closure, suggesting delayed and/or impaired secretory activation that is accompanied by lower pumped MOM volume and the lack of achievement of CTV in mothers of premature infants. These findings are important because impaired lactation translates into a reduced NICU and lifetime dose of MOM for premature infants with a higher risk of costly and potentially preventable morbidities. Furthermore, these initial findings suggest that MOM biomarkers hold promise as objective outcome measures in studies that compare interventions to increase MOM volume in this population, and ultimately in point-of-care testing to identify and proactively manage mothers at risk for insufficient MOM volume.
Footnotes
Acknowledgments
Research was supported by grants from Rush University Children's Hospital Department of Pediatrics (R.H.), Family Larsson-Rosenquist Foundation (Trainee Travel Award to C.M.P.), and an unrestricted grant from Medela AG, Switzerland, for research assistant salary. The University of Western Australia team (D.G., C.T.L.) performed MOM analysis in-kind and provided partial funding for sample shipment.
Ethics/Consent Statement
Written consent was obtained from all subjects for participation in the study.
Authors' Contributions
All authors made substantial contributions to the study design, analysis, and interpretation of data, and drafting and revising the article. All approved the final version to be published.
Disclosure Statement
No competing financial interests exist.