
Abstract
Abstract
Background:
Preliminary qualitative research in upstate NY shows new mothers are worried about safety while breastfeeding. Little is known regarding prevalence of these concerns and their effect on breastfeeding outcomes.
Objectives:
(1) Determine frequency of breastfeeding safety and privacy concerns; (2) Explore their association with breastfeeding outcomes.
Methods:
Mothers were surveyed immediately and 1-month postpartum about breastfeeding goals; both surveys addressed privacy and safety concerns at home, work, and in public. Outcome data included breastfeeding intent, exclusivity, and duration. Breastfeeding/non-breastfeeding mothers were compared using Chi-square and multivariate analyses.
Results:
A total of 279 women enrolled. Of these 82.8% initiated breastfeeding; at 1-month 72% provided any breast milk, and 44% were exclusively breastfeeding. About 99% felt safe breastfeeding at home; 25% reported privacy concerns; and 5% felt “vulnerable or unsafe” while breastfeeding. At 1-month, 49% agreed there was a safe place to breastfeed/express milk at work (20% unsure). Non-breastfeeding mothers expressed more safety concerns outside home/at work: 18% breastfeeding versus 28% non-breastfeeding outside home; 27% breastfeeding versus 40% non-breastfeeding at work. Nearly 54% who reported feeling vulnerable/unsafe with breastfeeding initiated breastfeeding, compared with 86% not reporting this concern (p = 0.008). Fewer women initiating breastfeeding reported vulnerability/safety (3% breastfeeding versus 14% non-breastfeeding, p = 0.008) or privacy (22% breastfeeding versus 40% non-breastfeeding, p = 0.19) concerns. Associations held after controlling for age, race, parity, insurance, geography, and marital-status. Significant associations between initiation, privacy, and safety concerns did not extend to duration or exclusivity.
Conclusion:
Many breastfeeding women reported safety and privacy concerns, especially outside the home and at work, which may influence breastfeeding initiation. Further study may identify methods to address these issues, potentially increasing breastfeeding rates.
Introduction
B
This topic is relatively unstudied in the literature, and few reports address how maternal safety and privacy concerns affect breastfeeding. Keely et al. 8 reported that privacy concerns both inside and outside of healthcare settings impact breastfeeding behaviors in obese women. In this qualitative study, mothers' struggles with privacy were associated with early cessation of breastfeeding and switching to formula feeding. In the workplace, social support and the availability of private spaces in which to express milk may prolong breastfeeding exclusivity,9,10 whereas the lack of such support may encourage formula feeding.11,12
Unpublished data from focus groups of a multi-generational inner-city population in Rochester, NY, identified safety and privacy concerns for breastfeeding mothers (A. Dozier, PI: NIH-NICHD, Grant # RO1-HD055191. A community partnership for breastfeeding promotion and support. Focus groups, unpublished data). Therefore, as part of a larger project to evaluate an intervention to increase breastfeeding rates this community, we conducted secondary analysis of new mothers who lived in a low-income, high-risk area of Rochester, NY. We surveyed mother's breastfeeding attitudes, experiences, and outcomes. Our goal was to assess the frequency of breastfeeding safety and privacy concerns, and explore their association with breastfeeding outcomes.
Methods
This is a secondary data analysis of the project entitled, “A pilot test to evaluate the feasibility and acceptability of an intervention designed to increase breastfeeding rates in Monroe County” funded by the Wilson Foundation in Rochester, NY. The study included mothers over 18 years with live births at an academic hospital between April, 2015 and May, 2016. Mothers of multiples were included in the analysis, but reported on their first baby only. Mothers who were too medically unstable to complete the survey and mothers whose babies were removed from their care were excluded. The University of Rochester's Institutional Review Board approved the study protocol.
Mothers were surveyed at the hospital after giving birth, and again 1 month later by phone or home visit. Both surveys included questions on feelings of safety and privacy at home, work and in public; breastfeeding intentions and goals; return to work/school; and demographics. As no previously validated survey tool that included safety while breastfeeding existed, survey questions were designed by the investigator with expert input and piloted in nine cycles with 19 target patients and 3 interviewers. Pretesting enabled refinement of the survey questions. Safety and privacy were intentionally juxtaposed in questions, to clarify for respondents that these were separate areas of interest. In addition, the word “vulnerable” was added to the word “unsafe,” to help respondents more closely identify the feeling we were attempting to study. Surveys were administered by interviewers trained by the primary investigator to ensure consistency. When surveys were completed on paper in the home, data were double-entered for accuracy. Pretesting showed that women responded negatively to interviewers asking visitors to leave their hospital room for the survey, so visitors were not excluded during the interview. Due to the concern that visitors could influence how women answered, particularly with respect to home safety questions, each woman identified her visitors and their relationship to her. Results were then analyzed by category of visitor to check for significant variation.
At the time of the hospital interview, breastfeeding initiation was defined as an answer of “yes” to the question: “Are you currently breastfeeding or feeding any expressed/pumped breast milk your new baby?” Answers of “no,” or, “I tried a few times but have decided not to breastfeed” were both marked as “No breastfeeding initiation.” At the 4 week interview, mothers answered the question “How are you feeding your baby as of today?” and were categorized as either “No breastfeeding,” “Any breastfeeding,” or “Exclusive breastfeeding” (breastfeeding with or without pumping at 1 month without formula supplementation). Mothers responded to six safety questions (Table 1) on a four point Likert scale from strongly disagree to strongly agree; these data were analyzed as a binary variable: “Agree” or “Disagree.”
“Would” was used for women intending to feed only infant formula.
“Pumping” was used instead of “breastfeeding” for all questions to women who were pumping only, not feeding at the breast.
This question was only asked to women who had ever breastfed or pumped milk.
Zip code data were collected to determine the effect of place of residence on breastfeeding and safety. In Rochester, NY, nine zip codes clustered around the inner-city have been associated with the poorest medical outcomes and highest rates of poverty and violence; these were categorized as “High-Risk Zip.” 13
We compared breastfeeding and non-breastfeeding mothers' (any breastfeeding versus no breastfeeding) responses about safety and privacy concerns using Chi-square and multivariate analyses, controlling for demographic variables found to be associated with breastfeeding in bivariate analyses (insurance, education, marital status, high-risk zip code, baby's father living in the home, Women, Infants and Children Supplemental Food Program [WIC] participation, age), in addition to parity and race.14–17 A p-value of <0.05 was considered statistically significant.
The primary study from which this secondary analysis was gleaned included an intervention and a control group, and was conducted in a pre and post format. We compared demographics and breastfeeding rates between the control and intervention groups and found no statistically significant differences, so the groups were combined for this subanalysis. To ensure that the intervention did not alter perceptions of safety and privacy, we also analyzed the preintervention group's responses independently and found the same results as when the postintervention group was included. We are therefore including the analysis of both the pre- and postgroups together.
Results
Demographics
Between April, 2015 and May, 2016, 279 women met inclusion criteria and were interviewed during their birth hospitalization and 239 women reached for their 1 month interview (86% retention). About half self-identified as White/Caucasian, and a quarter as Black/African American (Table 2). The age range was 18–42. About half were privately insured, with the rest publically insured (38%) or uninsured (9.7%). Regarding place of residence, 38% lived in a “High-Risk Zip” area. Other demographic characteristics of our study population and associations with breastfeeding are shown in Table 2.
Statistically significant.
WIC, Women, Infants, and Children Supplemental Food Program.
Among our sample, 231 of women (83%) initiated breastfeeding and 171 (72%) reported breastfeeding at 1-month follow-up, with 105 (44%) breastfeeding exclusively at 1 month. Eighteen (9%) were feeding only pumped breast milk at 1 month. All demographic factors were significantly associated with breastfeeding outcomes except for parity, poverty outside of the “High-Risk Zip,” and living with one's mother.
Overall, 48% were married, 57% were multiparous, and 86% had prior breastfeeding experience, although for 22% of women this experience was <1 month. Regarding breastfeeding experiences, 68% of mothers identified their past breastfeeding experience as a “fairly good” or “very good.” When asked about their feelings on becoming pregnant, only 166 (60%) reported a planned pregnancy. Close to 167 women were employed or in school during pregnancy (79% of the 212 one month respondents) and 14 women were employed or in school at 1 month (7% of the 212 one month respondents).
Breastfeeding and safety or privacy concern frequencies
During their inpatient hospitalization, 99% of women in our cohort responded that there was a safe place to breastfeed in their home, while 81% felt there was a safe place to breastfeed outside of the home (Table 3). Of those who worked during pregnancy (N = 220), 158 (72%) reported having a safe place at work. A quarter (25%) of women reported privacy concerns and 13 (5%) agreed they would feel “vulnerable or unsafe” while breastfeeding.
N = 220, bN = 211.
–, no data.
In contrast, by 1 month postpartum, only 49% (versus 72% at baseline) of women agreed there was a safe place to breastfeed/express milk at work, and another 20% were unsure. Further, only 48% (versus 81% at baseline) agreed that there was a safe place to breastfeed when out of the home. As many as 44% of women reported taking measures to protect their privacy and 9% reported having taken measures to protect both their safety and privacy. No women reported only taking measures to protect their safety.
Associations with breastfeeding outcomes
At the hospital interview, non-breastfeeding mothers were more likely to report privacy concerns than breastfeeding women (40% non-breastfeeding versus 22% breastfeeding, p = 0.019), and were more likely to agree that they would feel vulnerable or unsafe while breastfeeding (14% non-breastfeeding versus 3% breastfeeding, p = 0.008) (Fig. 1). Though non-breastfeeding mothers expressed more concerns about safety outside of the home (40% non-breastfeeding versus 27% breastfeeding p = 0.099), and were less sure of a safe place to breastfeed at work (63% non-breastfeeding versus 73% breastfeeding, p = 0.209), these differences were not statistically significant. Only two women reported feeling unsafe at home, both of whom did not initiate breastfeeding (p = 0.021). About half (54%) of the women who reported feeling vulnerable/unsafe with breastfeeding initiated breastfeeding, compared to 86% who did not report this concern (p = 0.008) Fewer women who initiated breastfeeding reported vulnerability/safety concerns: 3% breastfeeding versus 14% non-breastfeeding, p = 0.008. At 1 month postpartum, there were no statistically significant differences between breastfeeding and non-breastfeeding mothers regarding safety or privacy.
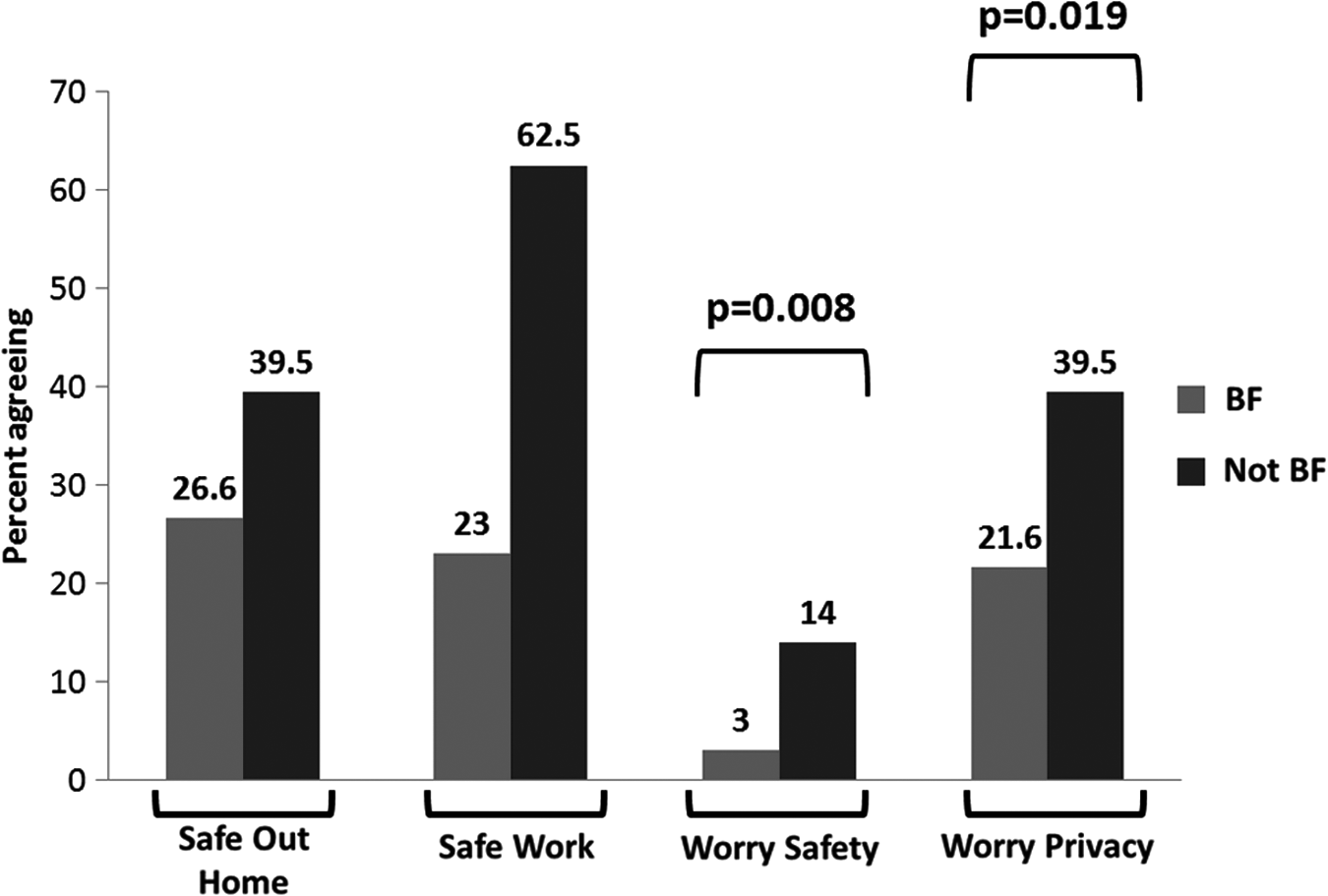
Self-reported safety and privacy concerns between breastfeeding and non-breastfeeding women in the hospital. BF, breastfeeding.
Associations with place of residence
In a zip code analysis, those living in a “High-Risk Zip” initiated breastfeeding less often than those living in other areas (76% High-Risk Zip versus 87% outside, p = 0.034), though these women did not report more safety or privacy concerns. At 1 month, those in the “High-Risk Zip” continued to have lower rates of breastfeeding than those outside (59% versus 79% outside, p = 0.002). Also, those in the “High-Risk Zip” codes had lower rates of feeling unsafe breastfeeding outside of the home (39% in versus 62% outside, p = 0.002).
Associations with race/ethnicity
Women identifying as Asian/Pacific Islander had the highest reported rates of privacy concerns during the hospital interview (62% worried about privacy), while black/African American (15%) and Hispanic/Latina women (18%) reported the least concern (p = 0.005). Among White/Caucasian mothers, 37 women (26%) reported worries about privacy while breastfeeding. Between racial/ethnic categories, differences were non-significant in breastfeeding initiation or worries of safety in the home, out of the home or at work. Figure 2 shows differences in breastfeeding rates and safety concerns by self-identified race/ethnicity. At 1 month, there were significant differences in any breastfeeding rates between groups, with Asian American women reporting highest rates (100%) and black/African American women reporting the lowest rates (58%) (p = 0.016 across all groups). Additionally, feeling unsafe breastfeeding out of the home at 1 month varied by race/ethnicity, with black/African American women reporting least concerns (34%) and Asian American/Pacific Islander women reporting the most concerns (67%) (white (60.7%), Hispanic/Latina (50%), Other (46.2%), p = 0.021 across all groups).
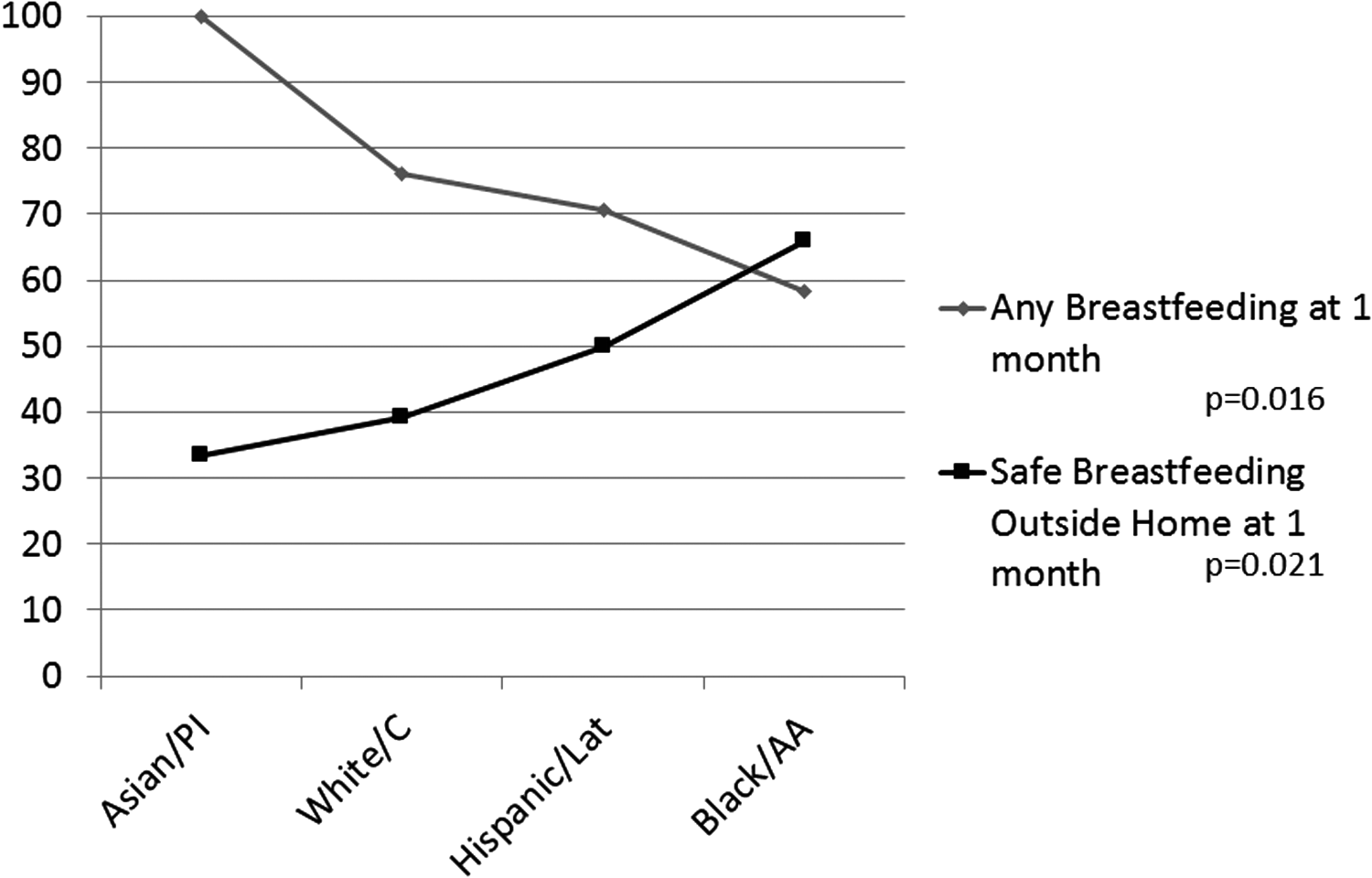
Breastfeeding at 1 month and reports of safety concerns breastfeeding outside the home reported by race. PI, Pacific Islander; C, Caucasian; Lat, Latina; AA, African American.
Associations with other residents in the home
We saw significant differences in breastfeeding rates depending on who the mother lived with at baseline and 1 month, as reported in Table 2, but found few differences in concerns about privacy or safety. At baseline, living with the baby's father, the paternal or maternal grandmother of the baby did not appear to affect concerns of privacy or safety. Numbers of women living with unrelated adults were too small from which to draw useful conclusions. Living with any other children decreased the likelihood of reporting privacy concerns (with any children, 20% concerned versus without any children, 32% concerned, p = 0.029). At 1 month, women living with the father of the baby were less likely to report having a safe space outside of the home to breastfeed (living with father 44% safe versus without father 60% safe, p = 0.057), while living with any children increased the likelihood of having a safe space outside the home (with any children 55% safe versus without children 36% safe, p = 0.013).
There were no significant associations between safety and privacy concerns and exclusive breastfeeding intent or breastfeeding exclusivity at 1 month.
Regression analysis
In multivariate regression analysis, controlling for insurance, education, marital status, high-risk zip code, baby's father living in the home, unrelated adults living in the home, WIC participation, age, parity, and race/ethnicity, we found an association between safety and privacy concerns and breastfeeding initiation at baseline (Table 4). Women who worried they would feel vulnerable or unsafe while breastfeeding were 5.9 times less likely to initiate breastfeeding (odds ratio [OR] 5.884, confidence interval [CI] 1.362–25.41, p = 0.018), while women who worried about privacy were 3.4 times less likely to initiate breastfeeding (OR 3.449, CI 1.445–8.232, p = 0.005). Those who did not have a safe place outside the home to breastfeed were 2.6 times less likely to initiate (OR 2.597, CI 1.086–6.211, p = 0.032), while not having a safe place to breastfeed at work was not associated with initiating breastfeeding (OR 1.905, CI 0.784–4.630, p = 0.155).
Controlling for insurance, education, marital status, high-risk zip code, baby's father living in the home, unrelated adults living in the home, WIC participation, age, parity, and race.
Statistically significant.
OR, odds ratio; WIC, Women, Infants, and Children Supplemental Food Program.
At 1 month postpartum, we found no statistically significant differences in breastfeeding outcomes by concerns about privacy and vulnerability/safety outside of the home and at work. Additionally, 1 month breastfeeding rates were not associated with baseline concerns of privacy, vulnerability/safety outside of the home and safety at work.
Discussion
Breastfeeding initiation rates and duration at 1 month in our sample were similar to NY state and Monroe County rates at 83% initiation (82.2% New York State 1 ), and 72% any breastfeeding at 1 month (73% Monroe County; A. Dozier, unpublished data). Breastfeeding exclusivity at 1 month was 44% for our sample, compared to rates for low-income women (34%) and non-low income women (64%) in Monroe County.
Safety and privacy concerns while breastfeeding were common in our community, with almost 5% of women reporting immediately postpartum they would/did feel vulnerable or unsafe while breastfeeding; about 10% of women took measures to protect their safety and privacy while breastfeeding at 1 month postpartum. Lower breastfeeding initiation was associated with concerns at baseline about safety/vulnerability, safety outside the home, and privacy concerns, even while controlling for potential confounders. Women who expressed concerns of safety/vulnerability while breastfeeding were almost six times less likely to initiate breastfeeding than those without these concerns. These findings add to prior research showing that women with anxiety were less likely to initiate breastfeeding, 2 and that privacy concerns can impact breastfeeding rates. 8
Women's concerns increased at 1 month postpartum, with more reporting concerns of safety outside the home and at work than they reported during their hospital stay. In the hospital survey, most women (72%) thought there was a safe place to breastfeed or pump at work, but this dropped to 49% of women at 1 month, and another 20% were unsure of their safety at work. It is possible that reentering the community as a breastfeeding mother led to difficult experiences that caused these concerns. However, neither baseline nor 1 month concerns for safety and privacy appear to be associated with 1 month breastfeeding rates.
In the analysis by self-identified racial/ethnic group, we found that while black or African American women had the lowest rates of breastfeeding in our sample, consistent with national data,18,19 they also reported the lowest level of concern about safety and privacy. Conversely, women identifying as Asian or Pacific Islander had the highest rates of breastfeeding and the highest concerns of safety and privacy. Importantly, our multivariable analysis showed an association between breastfeeding initiation and safety and privacy concerns, even after controlling for race. It appears, therefore, that safety and privacy concerns may have an impact on the decision to initiate breastfeeding, independent of the impact of race.
We suspect that the higher rates of breastfeeding among Asian women may allow for more negative personal or witnessed experiences. Twamley et al.'s qualitative work in England showed that Southeast Asian women living in multigenerational households experienced more concerns about privacy while breastfeeding and this impacted their breastfeeding decision making. 20 It is possible that cultural or household factors play a role, including cultural differences in privacy attitudes, social norms, or in the interpretation of the survey question itself. On the other hand, Zhao et al. also found that Chinese women who had more knowledge of or experience with breastfeeding were more likely to accept breastfeeding in public places, indicating that education or psychosocial factors play important roles in attitudes toward breastfeeding, 7 and that they may be modifiable. These high rates of Asian American or Pacific Islander concerns of safety and vulnerability warrant further investigation.
We also found that women living in the “High-Risk Zip” had the lowest rates of breastfeeding as well as the lowest rates of reporting concerns of safety or privacy. The findings that breastfeeding rates are geographically distributed is consistent with a study from Kentucky that suggested that income, race, and geography all play a role in breastfeeding outcomes. 3 However, more research is needed to examine what is at play when our highest risk inner-city communities with historically poor medical, social, and violence outcomes show lower rates of concerns around safety while breastfeeding. It is interesting that women in our cohort who lived with other children, even if they weren't their own children, worried less about safety and privacy. On the other hand, mothers who lived with the baby's father showed more concerns of safety outside the home. These findings highlight the likelihood that factors inside the home influence, or potentially predict, experiences outside.
Limitations
This study had several limitations. First, generalizability is limited because the study was conducted in one county in upstate NY, where community conditions and culture are different from other parts of the United States. The sample size limited the power of subgroup analyses of racial and ethnic categories as well as further analysis of the small but substantial category of women exclusively pumping breast milk at 1 month postpartum (9%). The surveys were interviewer-administered to remove literacy as a barrier to participation, but this method may have contributed to social-desirability bias. Also, pretesting showed that women responded negatively to asking visitors to leave their hospital room for the survey interviews, so visitors were not excluded. Those in the room may have influenced how women answered, particularly with respect to home safety questions. However, survey responses were analyzed by visitor presence at the time of the interview and no statistical associations were found. Mothers were asked no questions about their experiences of trauma and abuse, which could represent a missed confounder. Experiences of privacy and safety/vulnerability are likely to be multifactorial and involve both actual, as well as perceived, threats to the individual and the infant. Future research examining women's experiences should take into account the impacts of media on women's experiences of safety.21,22 Finally, it is possible that privacy and safety/vulnerability concerns impact and inform each other, vary culturally, and may be difficult to differentiate. However, pretesting showed that question order helped to clarify and juxtapose these concepts for respondents, and our later analyses confirms their relative independence and different impact on breastfeeding outcomes.
Conclusion
Safety and privacy concerns while breastfeeding are common in our community and appear to increase for mothers at 1 month postpartum. These concerns were related to breastfeeding initiation but not duration at 1 month, even after potential confounders were controlled. Concerns were lowest in black or African American women and inner-city women, and highest in the Asian American/Pacific Islander group and suburban women. Further exploration of these associations through multiethnic qualitative studies is needed to further define these concerns so that we may ensure that every woman has the opportunity to breastfeed, and feel comfortable and safe doing so.
Footnotes
Acknowledgments
The authors would like to thank the Wilson Foundation (#040GR527967; PI: C.R.-C.) and the National Institutes of Health (PHS Grant # RO1-HD055191; PI: A.D.) sponsored “Community Partnership for Breastfeeding Promotion and Support” for their support of this project.
Disclosure Statement
Dr. C.R.-C. is on the medical board of May and Meadow, a digital health technology startup. No competing financial interests exist for the remaining authors.