
Abstract
Abstract
Background:
Of the various barriers to breastfeeding, limited information is available on the relationship between prenatal stress and breastfeeding. This study investigates the association between prenatal stressful life event (SLE) exposure and breastfeeding initiation postpartum.
Materials and Methods:
Using Rhode Island Pregnancy Risk Assessment Monitoring System data from 2012 to 2014, SLE was defined as self-report of prenatal exposure to 14 predefined life events such as job loss or illness. Exposure to SLE was categorized by number and type of events. Multivariable logistic regression was performed to assess the relationship between SLE and breastfeeding initiation. Results accounted for complex survey design and were adjusted for maternal and infant characteristics (age, race, ethnicity, insurance, delivery type, parity, gestational age, birth weight for gestational age, and neonatal intensive care unit admission).
Results:
Among 3,353 respondents, 86% reported breastfeeding initiation, 74% reported exposure to ≥1 SLE, and 17% reported exposure to ≥4 SLE. Decreased odds of breastfeeding initiation were associated with prenatal exposure to ≥4 SLE (adjusted odds ratio [aOR] 0.67; 95% confidence interval [CI]: 0.48–0.95), emotional stressors (aOR 0.77; 95% CI: 0.61–0.98), and traumatic stressors (aOR 0.68; 95% CI: 0.50–0.91).
Conclusion:
This study underscores the impact of exposure to prenatal SLE on breastfeeding initiation among postpartum women. Findings may assist providers in identifying at-risk women for anticipatory guidance to improve breastfeeding rates.
Introduction
T
Life events are environmental stressors that may negatively impact health outcomes. 9 Epidemiologic studies suggest that psychosocial stressors, such as conflict, bereavement, and high perceived stress during pregnancy, are associated with low birth weight, preterm birth, and adverse neurodevelopmental outcomes in children.9–15 In separate studies among postpartum women, Copper et al. 16 and Zhu et al. 17 showed that perceived life stress was associated with increased odds of preterm birth. Zhu et al. 17 also demonstrated that for each unit increase in perceived life stress during early pregnancy, there was a nearly 100 g decrease in infant birth weight. 17
It is well established that maternal mental health and perceived social support can affect maternal breastfeeding attitudes and behaviors.1,4,5,18–21 There is limited information available, however, regarding the relationship between other environmental stressors and breastfeeding outcomes. This study investigates the association between prenatal stressful life event (SLE) exposure and breastfeeding initiation. The authors hypothesize that increased exposure to prenatal stress is associated with decreased breastfeeding initiation. Identification of specific barriers to breastfeeding related to life events among postpartum women may help direct providers' anticipatory guidance to improve breastfeeding rates in high-risk populations.
Methods and Materials
Study design and population
For this study, data from the State of Rhode Island (RI) Pregnancy Risk Assessment Monitoring System (PRAMS) was utilized. PRAMS is a population based, cross-sectional validated survey designed to collect state data on risk factors in the pre- and postnatal periods. Women having given birth to a live infant in the preceding 2–6 months are randomly selected from state birth certificate files and, subsequently, interviewed using mailed questionnaires and telephone surveys. Women are interviewed in both English and Spanish. Women with low birth weight infants are oversampled in the RI PRAMS to ensure representation of this high-risk population. Questionnaire responses are then linked to deidentified birth certificate data. Since 2012, the RI PRAMS has had a minimum response rate threshold of at least 60%. Three years of the latest RI PRAMS data available (2012–2014) were combined to increase the sample size. Institutional review board approval was not necessary, as the data used were of a completely deidentified, secondary data analysis dataset. 22
Of the 3,642 respondents from the 2012 to 2014 RI PRAMS dataset, 55 women with infant deaths and 93 women with missing information for living child status were excluded from the study. Those with missing information on the outcome (N = 122) or the exposure (N = 19) were also excluded. The final analytic sample was 3,353 women or 92% of the total 2012–2014 PRAMS respondents.
Independent variables
Maternal prenatal stress exposure was assessed using an SLE inventory from the PRAMS questionnaire. 22 The PRAMS SLE inventory is a modified life event inventory included in the PRAMS since 2004.22,23 The 14-item question assesses maternal exposure to a range of SLEs in the 12 months before childbirth (Fig. 1). As in prior studies,12,13,24,25 an SLE score was created by summing “yes” responses to each question item. Based on the distribution of sum SLE scores, SLE exposure was grouped into four exposure number categories: 0 SLE, 1 SLE, 2–3 SLE, and ≥4 SLE. In addition, separate variables were created for four different domains of SLE exposure: traumatic, emotional, financial, and relationship, as documented by prior studies (Fig. 1).12,25 These SLE exposure domain variables were categorized dichotomously (yes or no) if the respondent answered “yes” to at least one of the questions in that domain.
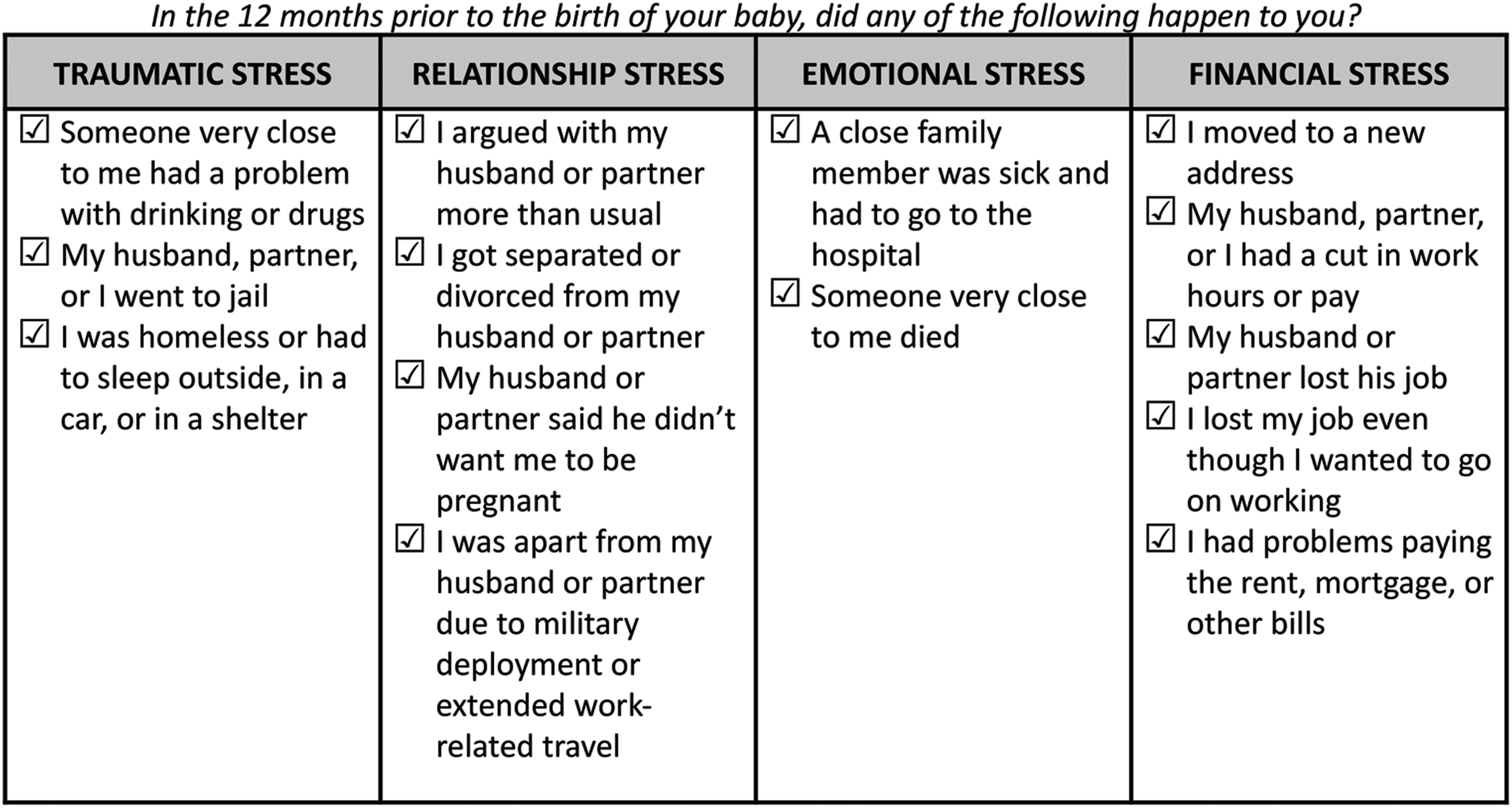
Stressful life event exposure index questions and stress type domains, RI PRAMS 2012–2014. RI, Rhode Island; PRAMS, Pregnancy Risk Assessment Monitoring System.
Dependent variables
Breastfeeding initiation (yes or no) was defined as respondent report of ever having breastfed or fed pumped breast milk to their new baby. Breastfeeding duration was defined as the number of completed weeks the mother reported feeding her baby breast milk. If the respondent noted that she was still breastfeeding at the time of the questionnaire, the number of weeks was calculated from the date the questionnaire was filed and the infant's date of birth. Since the PRAMS questionnaire is returned starting 10 weeks postpartum, breastfeeding duration was assessed at the 10-week mark using a binary categorical variable (yes or no) of breastfeeding duration ≥10 weeks.
Covariates
Based on prior literature, several demographic and potential confounding variables were included in the analysis. Demographic characteristics include maternal age,5,7 maternal race and ethnicity6,8 (White non-Hispanic, Black non-Hispanic, Hispanic, and other), parity, marital status 5 (married or unmarried), and primary insurance payer at delivery5,26 (private or public/none). Maternal prepregnancy body mass index was calculated from self-reported height and weight just before pregnancy and categorized as underweight or normal (<25 kg/m2), overweight (25 to <30 kg/m2), or obese (≥30 kg/m2).27–29 Smoking exposure was defined as maternal self-report of smoking during the last 3 months of the most recent pregnancy.
Postpartum depression (PPD) symptoms were defined using the two item Patient Health Questionnaire (PHQ-2), a validated screening tool for depression.19,30,31 On the PRAMS questionnaire, respondents were asked to mark “always,” “often,” “sometimes,” “rarely,” or “never” to the following two questions: (1) Since your new baby was born, how often have you felt down, depressed, or hopeless? (2) Since your new baby was born, how often have you had little interest or little pleasure in doing things? Respondents were categorized as having PPD symptoms (yes or no) if they answered “always” or “often” to either, or both, of the two questions. Postpartum family and community support was measured using a five-item question assessing maternal access to help in regards to monetary support, bed rest, emotional support, help if tired or frustrated, and transportation assistance. Mothers responded “yes” or “no” to each question, and “yes” responses were summed to create a level of community and family support variable, ranging from 0 to 5.
Several infant and delivery characteristics were derived from birth certificate data, including: delivery mode (vaginal or cesarean), gender, birth weight (normal [≥2,500 g] or low birth weight [<2,500 g]), gestational age (term [≥37 weeks] or preterm [<37 weeks]), and birth weight for gestational age (small for gestational age (<10th percentile), appropriate for gestational age (≥10th percentile and ≤90th percentile), or large for gestational age (>90th percentile)). History of neonatal intensive care unit (NICU) admission was defined as maternal report of the infant being admitted to the NICU after delivery.
Data analysis
Statistical analysis was performed using STATA version 14.0. 32 To examine population estimates and adjust for low birth weight oversampling, nonrespondents, and noncovered samples, all analyses were weighted and accounted for complex survey design, as recommended by PRAMS methodology. 22 Descriptive statistics of demographics and covariates was examined by SLE exposure number. Unadjusted odds of breastfeeding initiation were calculated using logistic regression and then adjusted for demographics (maternal age, race, and insurance type) and potential confounders (parity, delivery mode, gestational age, birth weight for gestational age, and NICU admission). Covariates were included in the model based on clinical significance and statistical association with the outcomes (if p < 0.1). Due to sample size limitations and correlation with maternal demographic variables, marital status, maternal medical disease, and maternal smoking were not included in the final regression analysis. Observations (N = 309, 9.2%) were excluded from the primary adjusted analysis when individual covariate percent missing was <5%.
Several secondary analyses were performed to further characterize the association between SLE exposure and breastfeeding. Unadjusted and adjusted odds of breastfeeding initiation were obtained for each of the four SLE exposure domains. In addition, to assess a potentially different association between breastfeeding initiation and prenatal SLE exposure by maternal PPD, a stratified analysis by maternal PPD symptom status was also performed. In addition, because of potential differences in breastfeeding initiation, sensitivity analyses were done excluding women with births before 35 weeks and women without exposure to SLE in separate covariate adjusted regression models. Finally, to assess the association with duration of breastfeeding, odds of breastfeeding at 10 weeks postpartum were obtained according to SLE exposure number and domain.
Results
Participant characteristics and demographics by SLE exposure are shown in Table 1.
Adjusted Wald Test, p < 0.001.
Pearson chi-squared test of independence, p < 0.05.
Pearson chi-squared test of independence, p < 0.001.
Among women who breastfed, N = 2,919.
CI, confidence interval; SLE, stressful life event; RI, Rhode Island; PRAMS, Pregnancy Risk Assessment Monitoring System; NICU, neonatal intensive care unit.
Gestational age ranged from 23 to 42 weeks, with a median of 39 weeks. Overall, 74% of the study population was exposed to at least one SLE in the prenatal period, and 17% reported exposure to four or more SLEs. Women with the highest stress exposure were more likely to be younger (p < 0.001), have public or no insurance coverage (p < 0.001), be Black or Hispanic (p < 0.05), smoke during pregnancy (p < 0.001), have less family and community support (p < 0.01), and have PPD symptoms (p < 0.001) than women in the lowest stress exposure group. Infants of women in the highest stress exposure group were more likely to be small for gestational age, preterm, and require admission to the NICU (p < 0.05).
Among postpartum women, 86% reported initiating breastfeeding after delivery. The distribution of breastfeeding outcomes among the study population is shown in Table 1. Less women in the highest stress group initiated breastfeeding compared to women without exposure to SLEs, 83% and 88%, respectively (p < 0.001).
Unadjusted and adjusted odds of breastfeeding initiation are shown in Table 2. After adjusting for maternal age, race, ethnicity, parity, insurance type, delivery mode, gestational age, birth weight for gestational age, and NICU admission, women with exposure to ≥4 SLE had 0.67 (95% confidence interval [CI] 0.48–0.95) decreased odds of breastfeeding initiation than women without exposure to SLEs. Odds of breastfeeding initiation were not different among those exposed to 1 or 2–3 SLE compared to women without stress exposure.
Adjusted for maternal age, race, ethnicity, parity, insurance type, delivery mode, GA, birth weight for GA, and NICU admission.
Adjusted Wald test, p < 0.05.
aOR, adjusted odds ratio; GA, gestational age; OR, odds ratio.
Secondary analyses
Odds of breastfeeding initiation differed for some of the SLE exposure domains (Table 2). After adjusting for covariates, women with exposure to traumatic and emotional stressors had 0.68 (95% CI 0.50–0.91) and 0.77 (95% CI 0.61–0.98) odds of breastfeeding initiation compared to women without those types of stressors, respectively. The odds of breastfeeding initiation were not different among women with and without financial stress or relationship stress.
In a stratified analysis, the association between stress exposure and breastfeeding initiation was stronger in women with PPD symptoms (Table 3). Among women with PPD symptoms, those with exposure to ≥4 SLE had 0.13 (95% CI 0.03–0.59) decreased odds of breastfeeding than those without stress exposure. In contrast, among women without PPD symptoms, odds of breastfeeding initiation were not different between stress exposure groups after adjustment.
Adjusted for maternal age, race, ethnicity, parity, insurance type, delivery mode, GA, birth weight for GA, and NICU admission.
Adjusted Wald test, p < 0.05.
PPD, postpartum depression.
When women with births before 35 weeks were excluded, odds of breastfeeding initiation were similar to the primary analysis (results not shown). When women without SLE exposure were excluded, the inverse association between SLE exposure and breastfeeding initiation strengthened. For example, compared to women exposed to one SLE, adjusted odds of breastfeeding initiation were 0.58 (95% CI 0.41–0.81) for women with exposure to four or more SLEs. In addition, adjusting for family and community support did not change the results of the primary analysis (results not shown).
Finally, we examined the relationship between SLE exposure and breastfeeding at 10 weeks postpartum. Adjusted odds of breastfeeding at 10 weeks did not differ by SLE exposure (results not shown). Among women who breastfed, those with exposure to emotional SLEs had 0.82 (95% CI 0.67–0.99) decreased odds of breastfeeding at 10 weeks, compared to women without exposure to emotional type events, given maternal and infant demographics.
Discussion
In this large population-based study, a strong association was found between increasing prenatal SLE exposure and breastfeeding initiation. Irrespective of prenatal stress exposure, it is encouraging that the proportion of women initiating breastfeeding in this study exceeds both the national estimates from the Centers for Disease Control and Prevention and the national goal set forth by Healthy People 2020. 3 The present study does, however, document a disparity in breastfeeding initiation with regards to prenatal SLE exposure, particularly for women with the highest stress exposure.
Maternal stress during pregnancy is a global public health problem. 15 A recent population based study by Burns et al. 12 found that prenatal stress exposure is both persistent and broadly prevalent among varying populations of postpartum women. The present study similarly found that 74% of women were exposed to at least one stressful event in the prenatal period, with 17% reporting exposure to four or more stressors. After adjusting for socioeconomic status, maternal race and primary insurance payer remained important risk factors for the association between stress exposure and breastfeeding initiation, a finding which is consistent with the current literature.6,12,14,33
The relationship between different types of prenatal environmental stress and breastfeeding has not been shown consistently in the literature. One study by Provenzano et al. 14 investigating the effect of material and financial hardships on various pregnancy outcomes did not find a difference in the mean duration of breastfeeding among material hardship exposure groups. A recent cross-sectional survey study by Islam et al. 34 showed that women with exposure to childhood abuse or intimate partner abuse after childbirth had decreased odds of exclusive breastfeeding compared to women without exposure. Similarly, the present study demonstrates that emotional and traumatic events are important factors in breastfeeding initiation.
The effect of peripartum life stress and maternal mental health disorders on obstetrical and infant outcomes is likely linked and difficult to separate.5,6,9 Prenatal stress has been shown to increase risk of PPD and maternal anxiety. PPD and peripartum anxiety have also been associated with decreased breastfeeding rates.11,13,15,18–21 Findings from this study suggest a complex relationship among prenatal stress, PPD symptoms, and breastfeeding. The association between life events stress, particularly emotional and traumatic stress, on breastfeeding initiation found in this study may reflect a woman's emotional well-being and ability to care for both herself and her family. Women with high stress exposure may be in a disadvantaged position to then cope with the added stress of having a new baby in the home. With anticipatory guidance, providers may assess risk factors and identify resources that may aid in mobilizing social supports and maximizing achievement of a woman's breastfeeding goals. In prior studies, efforts to improve perceived social supports among peripartum women have demonstrated improvements in obstetrical and infant morbidities related to prenatal stress and mental health disorders.9,35
There are several limitations in the present study. The PRAMS survey does not address maternal intention to breastfeed. Intent to breastfeed among postpartum women has been shown to be a strong predictor of breastfeeding initiation and duration in some studies.6,36–38 In addition, continued breastfeeding past 10 weeks postpartum could not be ascertained, given that mothers return the PRAMS questionnaire as early as 10 weeks postpartum. Further studies are needed to determine if stress exposure is associated with longitudinal breastfeeding outcomes in high risk populations.
A strength of the PRAMS survey is the ability to gather population based data which are otherwise unavailable. 22 It is important to consider, however, that this self-reported questionnaire has limitations in the data available to assess other factors which may affect the relationship between stress and breastfeeding outcomes. Aside from overall family and community support postpartum, the PRAMS survey does not assess other resilience factors, such as religious affiliations, which may counteract the effect of life stress on maternal and childhood outcomes. In addition, the PRAMS survey does not assess access to individual or community breastfeeding specific resources and/or role models, partner support of breastfeeding, or hardships related to workplace access to breastfeeding resources. Other known factors which may impact breastfeeding and/or stress were also not included in the regression analysis due to limitations in sample size and unavailable data. These factors include smoking exposure, marital status, maternal medical disease (such as obesity, hypertension, and diabetes), unplanned pregnancy, and exposure to domestic violence. Not adjusting for these factors may have introduced unmeasured confounding into the analysis. Finally, due to limitations in sample size and available data, the effect of mental health disorders (including PPD, gestational depression and anxiety symptoms, and use of mood altering substances) could not be ascertained. Further examination of the effect of mental health disorders on the relationship between stress and breastfeeding is warranted.
Overall, this study highlights the effect of SLE exposure on breastfeeding initiation, especially for women with multiple exposures in the prenatal period. Additional qualitative studies are needed to further clarify the relationship between prenatal stress and breastfeeding in high risk mothers.
Conclusion
The present study adds to the current literature by assessing the effect of environmental stressors as barriers to breastfeeding among postpartum women. Maternal screening in the prenatal and immediate postnatal period for prior and ongoing life event stress may help providers identify women with whom counseling or other supports may improve breastfeeding outcomes.
Footnotes
Acknowledgments
The authors thank the entire Rhode Island PRAMS program for its hard work and support of this project. Results of this study were presented by Catherine Buck, MD, at the Harvard Newborn Medicine Fellows Poster Symposium in Boston, MA, in May 2017 and the New England Perinatal Society Meeting in Newport, RI, in March 2018.
Disclosure Statement
No competing financial interests exist.