
Abstract
Abstract
Aim:
Oxytocin is a hormone involved in the mechanism of breastfeeding, uterine contractions, and social relationships. Atosiban (competitive oxytocin antagonist) is one of the most commonly used tocolytics for the threat of preterm labor in Europe. The aim of this study is to determinate if the administration of atosiban has any influence in the type of feeding in the term newborn at discharge. The secondary objective is to verify its effectiveness for the prevention of preterm delivery and in the possibility of applying treatment to complete lung maturation.
Materials and Methods:
Retrospective cohort study carried out in a tertiary University Hospital distinguished by WHO-UNICEF as a Baby-Friendly Hospital Initiative. The analysis included 264 women exposed to atosiban during a period of 4 years. One hundred met inclusion criteria. Unexposed infants born right after and before the exposed ones were selected as the not exposed subgroup (n = 200).
Results:
Among women treated with atosiban, 82% maintained exclusively breastfed (EBF), 8% had mixed breastfeeding, and 10% had formula feeding at discharge. In the nonexposed group, 82% maintained EBF, 9.5% had mixed breastfeeding, and 8.5% had formula feeding at discharge (p = 0.84). 97.5% of pregnant women treated with atosiban received corticosteroid for lung maturation, and 49.5% completed gestation with term newborns.
Conclusion:
There were no significant differences in the type of feeding at discharge between the atosiban group and the nonexposed group. In most cases, the administration of tocolytic therapy allowed to complete lung maturation.
Introduction
O
Atosiban is a synthetic competitive antagonist peptide of the oxytocin receptors, which is administered for the threat of preterm labor between weeks 24 and 33 of pregnancy. It has been observed that it binds to these receptors, reducing the uterine contractions by 75%.7,8
There are several barriers that avoid the flow of toxics from the mother to the fetus during pregnancy, such as the placental barrier and the blood–brain barrier. However, in the early stages of gestation, these barriers are immature and small quantities of toxics or drugs could reach the fetus.9–11 Atosiban has been shown to spread through the placental barrier by 12%, independently of the time of therapy administration, although it does not appear to accumulate in fetal circulation. 12
Due to the importance of oxytocin in the regulation of the mother–child bond and in breastfeeding, it is possible that the administration of an antagonist of this hormone has some repercussion on its physiological functions. 5 Few studies have evaluated the effect of tocolytic treatments on the mother–child binomial in the medium or long term. 13 Atosiban is one of the most commonly used tocolytics due to its insignificant systemic side effects, although it has not proved more efficacy than other tocolytics. 12 Besides, the cost of a treatment cycle with atosiban is 90 times greater than the therapy with other tocolytics such as nifedipine. The hypothesis of our study is that the administration of atosiban for the threat of preterm labor could modify the neurohormonal mechanism related with breastfeeding, even though the pregnancy comes to the end.
The main objective of the study is to evaluate the possible effects that the administration of atosiban for prevention of preterm birth could have in breastfeeding at the time of discharge in infants born at term. The secondary objective is to verify its effectiveness for the prevention of preterm delivery and in the possibility of applying treatment to complete the lung maturation.
Materials and Methods
Retroprospective cohort study over a 4-year period (2012–2015) was performed at a tertiary University Hospital distinguished by WHO-UNICEF as a Baby-Friendly Hospital Initiative (BFHI). Two groups of pregnant women were identified, treated, and not treated with atosiban. For the second group, newborns at term who were born immediately before and after the exposed ones were selected, according to the inclusion and exclusion criteria.
Women with single pregnancy, term delivery, and newborn with Apgar score at 5 minutes >7 were included. The exclusion criteria were multiple pregnancy, preterm newborn with Apgar score ≤7, admission of the newborn to the intensive care unit within 48 hours after birth, and newborns born in other hospitals. The study was approved by the local Ethics Committee.
In the exposed group, atosiban administration was performed according to the usual protocol of the center. First, a vial of 0.9 mL of Tractocile® injectable solution (6.75 mg) was administered over 1 minute; then, two vials of 5 cc of Tractocile perfusion solution (37.5 mg) were given for 48 hours.
For epidural anesthesia, mothers received levobupivacaine at 0.125% (Chirocane®; Abbott) combined with fentanyl or ropivacaine at 0.2% (Naropin® Polybag®; AstraZeneca) combined with fentanyl.
In vaginal deliveries performed at our center, the newborn who does not need resuscitation maneuvers is placed on the mother, dried, and kept in early skin-to-skin contact for 90 minutes. After this time, routine care (weight, height, cephalic perimeter, ocular prophylaxis, and antihemorrhagic prophylaxis) is performed. If the mother wants to give breastfeeding and the newborn does not suck the breast spontaneously, the action on the mother–child dyad can favor the beginning of the breastfeeding. During hospital stay, nurses carry out continuous health education favoring breastfeeding.
Discharge dates for vaginal deliveries were 2 days and 3 days for C-section mothers.
In caesarean sections, an attempt to initiate early skin to skin contact during the surgical procedure is also made if the maternal and/or fetal conditions allow it. If it cannot be done during the surgical procedure, it is performed once the dyad (mother/child) has been transferred to the recovery unit. The newborn remains always with the mother, unless they have to be admitted to the Neonatal Unit or to the Intensive Care Unit, respectively. During the hospital stay, the staff performs a continuous health education working about the breastfeeding, favoring the suckling and solving the doubts inherent to this process. In the same way, after discharge, mothers can consult their doubts about breastfeeding in a telephone attended by the midwives of the Obstetric Service 24 hours a day. 14
Data from clinical reports were collected. Information on the following variables was obtained: (1) demographic (age, nationality, and civil status); (2) maternal background (previous gestations, smoking habit, diabetes mellitus, hypothyroidism, and assisted or spontaneous gestation); (3) newborn data (gestational age at birth, weight, and sex). In addition, other variables related with pregnancy and delivery were collected: type of delivery (vaginal/caesarean section), gestational age at which atosiban was administered and number of cycles, administration of other tocolytics (nifedipine) and/or prenatal corticosteroids, or anesthesia at birth; Apgar score at 5 minutes and type of resuscitation. Finally, data on breastfeeding at discharge and administration of supplements if necessary were collected. Infants were considered exclusively breastfed (EBF) if they received no other liquids or breast milk substitutes in the last 24 hours before discharge.
Statistical analysis
Qualitative variables were described by absolute frequencies and percentages. In quantitative variables, normality was checked through the Kolmogorov–Smirnov test, calculating the mean and standard deviation if they fit a Gaussian distribution, and the median with 25 and 75 percentiles otherwise.
For the comparison between Atosiban versus No Atosiban groups, the Pearson chi-square test was calculated in case of qualitative variables; and in the case of small samples, the Fisher's exact test or the likelihood ratio correction was performed according to the presence of two or more categories, respectively. In the comparison of quantitative variables between these study groups, the Student's t test of independent samples or the Mann–Whitney U nonparametric test was performed depending on whether or not they fit a normal distribution, respectively.
All the analyses were carried out using SPSS version 14.0 software (SPSS, Inc., Chicago, IL).15–17
Results
During the study period, 264 pregnant women received atosiban, of which only 100 met the inclusion criteria and constitute the analysis sample (Fig. 1). The results of the epidemiological variables are shown in Table 1. Regarding the demographic data, pregnant women exposed to atosiban were younger and had a lower gestational age at the time of birth than the not exposed group. Only 8% of the women treated with atosiban received other tocolytics, such as nifedipine, compared to only 0.5% of the nonexposed (p = 0.001). The number of cycles of atosiban was one in 74%, two in 22%, and three cycles in 4%.
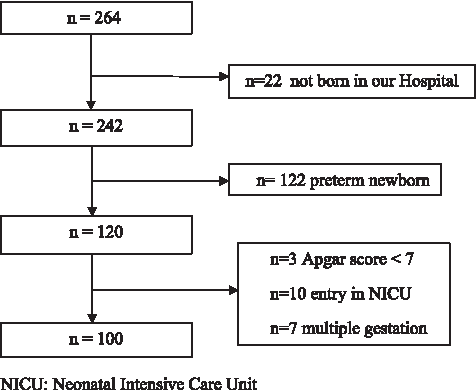
Flowchart of patients exposed to atosiban.
Quantitative variables are expressed as mean (standard deviation) and median (interquartile range) and qualitative variables are expressed as absolute frequency (percentages).
GA, gestational age.
In the exposed group, the newborns presented lower weight and were more frequently males than in the not exposed group. All infants had an Apgar test ≥9 at 5 minutes, with no difference between groups (p = 0.93).
With regard to the reanimation of the newborns, 76% of the exposed group did not require resuscitation, 19% needed aspiration of secretions, and 5% ventilation with positive pressure. In the nonexposed group, 74% did not require resuscitation, 22% required aspiration of secretions, and finally, 4% required positive pressure (p = 0.78).
The gestational age at which atosiban was administered was 30.02 ± 2.7 weeks. Among women treated with atosiban, 82% maintained EBF, 8% had mixed breastfeeding, and 10% had formula feeding at discharge. In the nonexposed group, 82% maintained EBF, 9.5% had mixed breastfeeding, and 8.5% had formula feeding at discharge (p = 0.84).
Of the 242 women who had received atosiban and continued the pregnancy in our center, 236 (97.5%) completed the cycle of pulmonary maturation with corticosteroids, and 120 (49.5%) ended the gestation at term.
Discussion
The results did not confirm our hypothesis. The administration of atosiban during pregnancy has no effect on the type of lactation in term newborns at hospital discharge.
There are few studies evaluating the effect of tocolytic treatments for the threat of preterm birth on breastfeeding. In a retrospective study conducted in Serbia, 13 the duration of breastfeeding in women who received tocolytic treatment with betamimetics (hexoprenaline and fenoterol) for preterm labor was assessed. They collected information from 114 pregnant women with a mean age of 26 ± 4.3 years through questionnaires performed at the control visits with their pediatricians during the period of 1 year. Women who received tocolytic treatment (n = 15) had maintained breastfeeding for less time than untreated women (9.5 ± 5.7 months versus 4.5 ± 2.1 months). Likewise, a higher incidence of hypogalactia (80% versus 18%) was observed in the group of exposed mothers.
Animal studies showed that sheep fed with betamimetics reduced mammary gland tissue and decreased milk production. 18 In rodents, it has been shown that activation of the sympathetic system may inhibit milk production. 19 Therefore, it is possible that this tocolytic treatment has a negative effect on human lactogenesis. These results, for now, have not been observed in the case of atosiban.
In our study, most of the patients with tocolytic treatment also received corticosteroids for lung maturation before the end of gestation, and in almost half of the cases, the pregnancy ended at term. There are several studies about the efficacy of tocolytics, although none of them has shown greater efficacy than the others. 20 It has been observed that atosiban decreases uterine electrical activity 21 in a more specific way than the rest of tocolytics, thus minimizing systemic side effects, 22 and is similar to placebo in relationship with maternal-fetal and neonatal side effects. 23 All these reasons make atosiban one of the most widely used tocolytics in Europe along with nifedipine.
In a systematic review, Usta et al., observed that, compared with placebo, the percentage of women who continued to be pregnant and who did not need an alternative tocolytic was significantly higher in the atosiban group at 24 hours (73% versus 58%), at 48 hours (67% versus 56%), and at 7 days (62% versus 56%). In this meta-analysis, there were not significant differences comparing atosiban with betamimetics (ritodrine, salbutamol, and terbutaline), in the delay of delivery at 48 hours (6.6% versus 11.4%) or at 7 days (20.3% versus 22.4%). Similarly, atosiban and nifedipine were compared with a similar prolongation of gestation in both groups (29.03 ± 16.12 days versus 22.85 ± 13.9 days). 12
In a review of 95 studies on tocolytic treatments, Haas et al. observed that, in comparison with placebo, the probability of delaying delivery in the first 48 hours was greater with prostaglandin inhibitors (OR 5.39, 95% CI 2.14–12.34), followed by magnesium sulfate (OR 2.76, 95% CI 1.58–4.94), calcium channel blockers (OR 2.71, 95% CI 1.17–5.91), betamimetics (OR 2.41, 95% CI 1.27–4.55), and finally atosiban (OR 2.02, 95% CI 1.10–3.80). 24
In another recent review about different tocolytic treatments for prevention of preterm delivery on 2,485 women, no difference in delivery delay was observed in the first 48 hours between atosiban and placebo (RR 1.05, 95% CI 0.15–7.43), atosiban and betamimetics (RR 0.89, 95% CI 0.66–1.22), and atosiban and nifedipine (RR 1.09, 95% CI 0.44–2.73). 25
Our study has several limitations. In the first place, it has been carried out in a BFHI center, which could affect external validity. Losses to follow-up may limit the obtained results, although we consider that they have had no influence on them because the percentage is very low (8.3%). In addition, there are differences related to certain demographic variables between the two groups, such as the lower weight of infants exposed to atosiban, an effect already described in literature. In fact, the weight reduction observed by Flenady et al. was similar to that obtained by our group (138 g versus 128 g). 25 It should be noted that the mean gestational age of the group exposed to atosiban was also lower, which may influence the weight differences found.
Finally, the design of the study can also be a limitation because it is a retrospective study without the possibility of collecting other variables that could modify breastfeeding at the time of discharge, such as the use of a pacifier or the maternal experience with previous lactations.
Further studies are needed to assess the influence of atosiban and other tocolytics on the initiation and maintenance of breastfeeding in both term and preterm infants.
Conclusion
We have not found influence between the administration of atosiban during the threat of preterm labor and the type of feeding at discharge. In addition, this tocolytic drug allowed completing pulmonary maturation in most cases.
Footnotes
Acknowledgment
To all mothers who have objectively participated in this study.
Disclosure Statement
No competing financial interests exist.