
Abstract
Abstract
Background:
Despite a mother's intention to breastfeed, there are many barriers to feeding preterm infants that decrease breastfeeding rates.
Objective:
The objective of this research was to determine factors associated with successful direct breastfeeding (DBF) of the preterm infant at hospital discharge.
Materials and Methods:
A retrospective chart review of 69 preterm (<34 weeks' gestational age) infants in the neonatal intensive care unit, whose mothers intended to breastfeed, was conducted. Infant-, mother-, and feeding-related factors were examined by chi-square or t test for their relationship with breastfeeding success, and by multiple logistic regression to identify predictive factors.
Results:
Successful DBF at discharge occurred in 64%. Mothers of infants who were breastfed were older (p < 0.0001); had less psychiatric illness (p = 0.03); and were less likely to smoke (p < 0.0001) and use recreational drugs (p = 0.04). The infants had higher birth weights (p = 0.03) and lower incidence of bronchopulmonary dysplasia (p = 0.04). A higher proportion of infants received DBF at their first oral feed (p < 0.001), and were discharged earlier (p = 0.03). Reduced milk supply was cited for breastfeeding failure in 36%. Older maternal age (odds ratio [OR] = 1.24, 95% confidence interval [CI] 1.02–1.51) and DBF at the first oral feed (OR = 7.72, 95% CI 1.37–43.6) were associated with successful DBF at discharge.
Conclusion:
Maternal age and method of first oral feed are critical predictors of breastfeeding success in preterm infants. Mothers should be encouraged to breastfeed at the infant's first oral attempt and strategic breastfeeding support should be provided before initiation of oral feeding.
Introduction
H
The World Health Organization (WHO) and Health Canada recommend that infants are exclusively fed from the breast until 6 months of age.6,7 Despite the well-known advantages of direct breastfeeding (DBF), the rate of mothers feeding their preterm infants from the breast at hospital discharge is low. In one study of 7,000 VLBW infants, only 6% received exclusive human milk at discharge, and only 42% received human milk in any form. 8 This is compared with the 76% of term infants who received exclusive breastfeeding at 1 month after discharge. 9
There are many barriers to feeding a preterm infant that may waylay a mother's existing plans to breastfeed. Infants born at less than 32 weeks' gestational age (GA) are developmentally unable to coordinate the sucking, swallowing, and breathing necessary for oral feeding, and must be fed via nasogastric tube. 10 Most mothers must depend on pumps to initiate and maintain milk supply for weeks or months before the infant can suckle at the breast. 8 Moreover, mother's own milk may be insufficient to meet the demands of a preterm infant, who requires more calories per kilogram than a term infant. 1 The establishment of DBF can be delayed because of physical separation while the infant is in the neonatal intensive care unit (NICU), and because infants can be too medically fragile for handling, prohibiting frequent skin-to-skin contact. 8 For the mother, obstetrical and preexisting illness (e.g., gestational diabetes mellitus, depressive, and anxiety disorders), combined with the stress of premature delivery, can further aggravate the situation and make breastfeeding the preterm neonate a demanding task.11–14
Historically, much of the research investigating the factors that affect breastfeeding in preterm infants have been concerned with the provision of mother's own milk in any form.11,15–17 However, DBF is distinct from and preferable to expressed mother's milk. Relative to DBF, expressing milk is time consuming and resource-intensive, and it introduces the risk of contamination and the degradation of beneficial immunologic and nutritional components due to freezing and storage. 18 Additionally, mothers who breastfeed directly have increased breastfeeding duration, 15 which enhances the likelihood that they will meet recommended health standards in feeding their infants.
To capitalize on the therapeutic effects of DBF, and to improve the low rates of breastfeeding in preterm infants, a greater understanding of the factors that contribute to DBF is needed. While a mother's intent to breastfeed has a major impact on breastfeeding success, 19 these breastfeeding goals tend to reflect less desire for human milk provision as the infant's hospitalization progresses, and are at the same time less likely to be met. 20 Not much is known about what factors may impede a woman from accomplishing her original goal of breastfeeding. This study aims to identify the maternal-, infant-, and feeding-related factors associated with preterm infants receiving DBF at hospital discharge, when their mothers intended to breastfeed. An understanding of these variables will facilitate the identification of mothers and babies who are at risk of not achieving their breastfeeding goals, and will promote the development of a strategic breastfeeding support program.
Materials and Methods
Design and setting
The current investigation is a retrospective chart review of preterm infants and their mothers admitted to the NICU. Ethics approval for this study was obtained from the Queen's University Health Sciences Research Ethics Board.
The study site was the level III NICU of the Kingston Health Sciences Centre (KHSC), a tertiary care center in Kingston, Ontario, Canada. This NICU has 22 beds and cares for ∼400 infants per year. KHSC is striving to become accredited as a Baby-Friendly Hospital Initiative (BFHI), a global effort advocated by the WHO to support breastfeeding initiation and exclusive breastfeeding until 6 months. To this end, the NICU has an adjacent room equipped with supplies for expressing milk. The KHSC does not have designated International Board Certified Lactation Consultants (IBCLCs), but it does have two members of the nursing staff who are certified as IBCLCs but who are able to provide the teaching and health-promotion aspects of IBCLCs.
Sample
The participants were a sample of all preterm infants born before 34 weeks' gestation between January 2014 and March 2016. Infants were admitted to the KHSC NICU at birth, and were excluded if they were transferred to another care facility before their discharge home. These infants had been previously enrolled in a retrospective study on oral feeding progression with a sample size of 101. The second-born of every twin pair was excluded to ensure that their mothers did not count as double in the analysis. As part of the admission history at the KHSC NICU, mothers are asked about how they intend to feed their child, and this is recorded in the infant's chart. Infants from this sample whose mothers had not expressed intention to breastfeed directly were excluded, resulting in a final sample of 69. Figure 1 demonstrates the sample selection process of infant-mother dyads for this study.
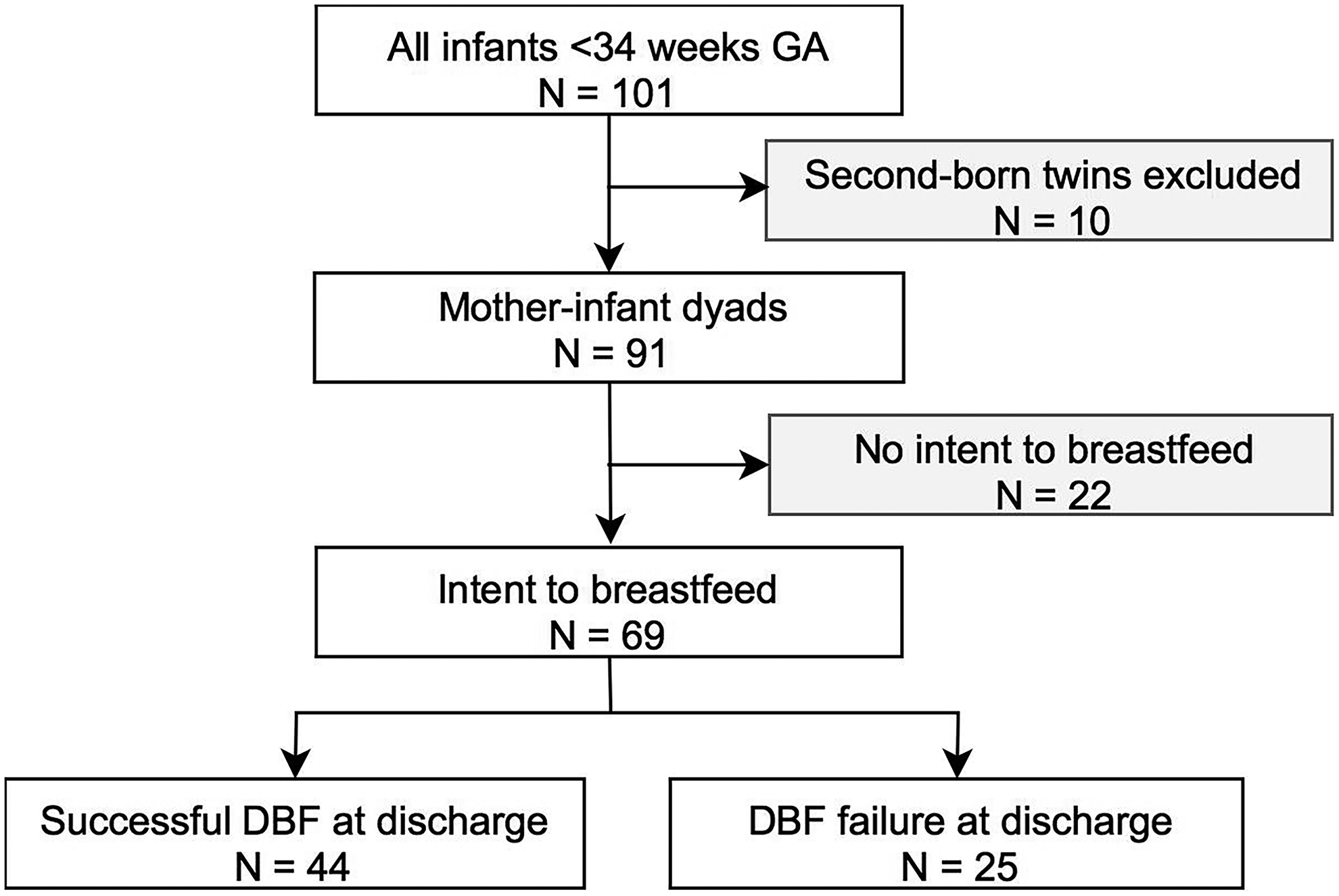
Flow diagram of sample selection process. Successful DBF was defined as when infants received equal to or more than 50% of feeds from the breast in the 24 hours before discharge. DBF, direct breastfeeding; GA, gestational age.
Measurement and data collection
This study defined DBF as when an infant suckled at the mother's breast for nutritive purposes. The primary outcome of this study was successful direct-breastfeeding at discharge, described as when infants received equal to or more than 50% of their feeds from the breast in the 24 hours before discharge. The 50% benchmark was chosen to allow infants who require supplementation with human milk fortifiers via bottle, to maintain adequate growth, as recommended by the neonatal dietitian.
The study examined several maternal-, infant-, and feeding-related factors for their relationship with direct-breastfeeding success, which were obtained from the mother's and infant's electronic medical records. The maternal characteristics included age (in completed years until the due date), body mass index (BMI), whether she was a first-time mother, whether she had multiple gestation, her mode of delivery (vaginal versus caesarean section), diabetes (gestational or preexisting), hypertensive disorders of pregnancy, and psychiatric illnesses (depression, anxiety, and bipolar disorder), smoking, opioid use, and other recreational drugs (including alcohol, marijuana, cocaine, and methamphetamine).
Infant characteristics included GA (reported in weeks and days), birth weight and whether they were affected by growth/feeding issues (as identified by the health team), intraventricular hemorrhage (grades I–IV), bronchopulmonary dysplasia, NEC (stages I–III), or cardiac anomalies. These illnesses were chosen because they may affect execution or coordination of the suck-swallow-breathe process that is required for safe and efficient oral feeding.10,21,22 The number of days of ventilation and continuous positive airway pressure support were also recorded from the infant's charts to examine how the need for significant respiratory support might affect breastfeeding success.
At the KHSC NICU, the time, method, volume or duration, and composition of each feed are recorded in the infant's chart, and these were accessed electronically as well. Feeding characteristics included number of days made nothing by mouth (NPO), mode of first oral feed (breastfeeding versus bottle), postmenstrual age (PMA), day of life, and weight at first oral feed, first full oral feed, and discharge. Full oral feeds were defined as the first day on which infants were able to take all prescribed volume of nutrients by mouth for two consecutive days.
Reasons for DBF cessation were gathered via perusal of the daily progress notes in the infants' charts, as the nursing staff documents discussions with parents regarding the infant's care, and changes made on medical rounds, and so on.
Data analysis
Statistical analysis was undertaken using IBM SPSS Statistics, version 23. Descriptive statistics data are presented as means and standard deviation for continuous variables and percentages for categorical variables. Bivariate analysis of success or failure to receive DBF at discharge and the variables were studied using either the chi-square test (χ2) for categorical variables or a two-tailed Student's t test for continuous variables. Significant (p < 0.05) variables from the bivariate analyses were entered into multivariate logistic regression, and are presented as adjusted odds ratios and 95% confidence intervals (CIs). p-values are two-sided and were considered significant at p < 0.05.
Results
Participant characteristics
Infants in this study had a mean GA of 31 ± 2.8 weeks. The average maternal age was 29 years. Infants spent an average of 3.5 days designated as NPO. The first oral feed occurred on average at day of life 26 (average PMA 34 weeks, 5 days), and consisted of a DBF in 75% of cases. Discharge occurred, on average, at day of life 48 (PMA 37 weeks, 5 days). A summary of participant characteristics can be found in Table 1.
Data expressed as mean ± standard deviation.
Data expressed as n (%).
p < 0.05.
BMI, body mass index; BPD, bronchopulmonary dysplasia; CPAP, continuous positive airway pressure; C-section, cesarean section; DBF, direct breastfeeding; DOL, day of life; ETT, endotracheal tube; GA, gestational age; IVH, intraventricular hemorrhage; NEC, necrotizing enterocolitis; NPO, nothing by mouth.
Of the 69 infants whose mothers had an intention to breastfeed, 80% received human milk at discharge from the hospital. Successful DBF was accomplished by 64% (n = 44) of mothers. The remaining 36% (n = 25) of infants who did not achieve ≥50% DBF were fed with formula only (56%, n = 14), formula and some breastfeeding (20%, n = 5), expressed milk and some breastfeeding (12%, n = 3), expressed milk only (8%, n = 2), or formula and expressed milk (4%, n = 1).
As compared with mothers who did not successfully provide DBF at hospital discharge, mothers who provided DBF at discharge were older (p < 0.0001), had less psychiatric illness by more than half (p = 0.03), and smoked (p < 0.0001) and used nonopioid recreational drugs (p = 0.04) more than five times less. Infants successfully directly breastfed at discharge had higher birth weights (p = 0.03), less BPD (p = 0.04), and received more DBF at the first oral feed (p < 0.001). These infants were also discharged 16 days of life earlier on average (p = 0.03). Though it was not significant, there was a trend for infants who received DBF at discharge to have fewer days on respiratory support, fewer NPO days, and fewer illnesses (save for cardiac anomalies).
Factors predicting DBF success at hospital discharge
Factors found to be significant in the bivariate comparison of mother-infant dyads who succeeded versus those who were unsuccessful at DBF at hospital discharge were selected for multivariate logistic regression. These were maternal age, psychiatric illness, smoking, recreational drug use, birth weight, BPD, and DBF at first oral feed. GA and maternal BMI were added into the equation due to the known association of GA and BMI with breastfeeding outcomes.9,23 The generated model was statistically significant (χ2 36.7, p < 0.0001) and predicted DBF success with 84.4% accuracy. The model identified two independent predictors of breastfeeding success, presented in Table 2. The first was maternal age, with each additional year of life increasing the likelihood of breastfeeding success by 1.24 (95% CI 1.02–1.51). Second, receiving DBF at the first oral feed increased an infant's likelihood of DBF success at discharge by 7.72 times (95% CI 1.37–43.6).
p < 0.05.
aOR, adjusted odds ratio; BMI, body mass index; BPD, bronchopulmonary dysplasia; BW, birth weight; CI, confidence interval; DBF, direct breastfeeding; GA, gestational age.
Reasons for DBF failure
Inadequate milk supply was cited in the infants' progress notes as a reason for failure in 36% (n = 9) of cases. In two (8%) cases, breastfeeding was reported to be “too stressful.” In three (12%) cases, medical reasons caused infants to be fed by bottle (apnea, reflux, and poor weight gain with DBF), and in one (4%), the mother's medical status hindered breastfeeding (admission to hospital). For the remaining 40%, no reason was given for the failure to breastfeed at discharge.
Discussion
In this retrospective chart review of 69 preterm infants, we show that infants whose mothers were older and who received DBF at the first oral feed were more likely to be breastfed at hospital discharge.
Our results corroborate a consistent theme in the literature, namely that early and frequent feeds at the breast are paramount to breastfeeding the preterm neonate. In particular, the provision of human milk at the initial enteral feedings, 24 and on the seventh day of life, 16 had strong positive impacts on infants receiving human milk at discharge. The findings of our study echo several others who showed that preterm infants who received their first oral feed at the breast were more likely to receive human milk at discharge.15,17 Infants having DBF at their first feed were breastfed for longer than their peers, 15 and infants who received one or more DBF per day were more likely to be receiving human milk at 4 months' corrected GA. 25 Our findings reaffirm previous research that suggests that if the NICU staff can enable mothers to provide the infant's first oral feed at the breast, breastfeeding outcomes may be improved.15,19 However, ours was the first study to connect DBF at the first oral feed, with the provision of DBF to their infants at discharge in mothers who originally intended to breastfeed.
Maternal age has been implicated in many studies of infants both preterm and term to positively impact breastfeeding.9,19,26 One reason for this is that advanced maternal age correlates with higher education and thus socioeconomic status, another well-known contributor to breastfeeding attainment. 24 Older and more educated mothers often have better health behaviors, problem-solving skills, and self-confidence and are more cognizant of the benefits of breastfeeding. 24 On the other hand, this study did not identify several variables that have been shown repeatedly to adversely affect breastfeeding outcomes, including younger GA,9,16 higher maternal BMI,23,26 and smoking. 27 And while gestational diabetes has been shown to negatively affect breastfeeding, 12 all mothers with gestational diabetes in this study were successful in providing DBF at discharge (though the difference between the groups was not significant).
Out of 69 women in this study with a predetermined wish to breastfeed, only 64% provided exclusive, DBF at discharge from the hospital. Maternal intention to breastfeed is a powerful predictor of breastfeeding outcomes 28 ; in another investigation of 88 preterm infants, while a breastfeeding goal increased the odds of breastfeeding at discharge by 13 times, only 50% of mothers who intended to breastfeed actually accomplished this goal. 19 These low rates of success are a testament to the existence of many barriers to feeding a preterm infant. Achieving adequate milk volume is cited as the most common reason why women discontinued breastfeeding. 29 Indeed, concerns related to insufficient milk were reported in a third of women in this study, and this number may be higher due to missing data regarding mothers' specific reasons for discontinuing DBF. Lactation is compromised in the majority of women delivering preterm due to immature hormonal profiles, stress and anxiety, and delayed breastfeeding initiation. 30 Expressing milk via electric or manual means is exhausting and associated with negative emotions that may further hinder milk production. 31
Considering this information, early, frequent feeds from the breast may be associated with breastfeeding success and longevity because they capitalize on the infant's ability to sustain milk production. Infants who were successfully breastfed at discharge received their first oral feed 1 week and a half earlier than those who were not breastfed, though this result was not significant. DBF stimulates oxytocin release through skin-to-skin contact 32 and in response to the infant suckling at the breast, 33 which relieves maternal stress. Since stress is a well-known antagonist of human milk production, 34 these practices encourage ongoing breastfeeding. DBF also provides a means to actively participate in an infant's care, imparting confidence and reinforcing the mother's disposition to breastfeed. 15 Furthermore, Suberi et al. suggest that preterm neonates are susceptible to “feeding imprinting” whereby the feeding method used during the transition to oral intake becomes the infant's preferred method. 35 Feeding imprinting was purported by Suberi et al. to explain why infants first fed at the breast received more mother's milk at discharge in their study, 35 and may be the reason for the increased rates of DBF at discharge among those receiving DBF at the first oral feed in the current investigation.
As evidenced by ours and previous research,15,19,35 the first oral feed is a critical window during which mothers who wish to breastfeed should be encouraged to put their baby to the breast. Skin-to-skin holding improves milk production 36 and breastfeeding initiation rates. 37 Thus, even before infants are physiologically and developmentally ready to breastfeed, NICU staff should enable skin-to-skin contact, as in kangaroo mother care, between mother and baby. Furthermore, mothers who are unable to provide DBF at the first oral feed, or who are at risk to do so, should be identified so that additional lactation support can be instituted. By anticipating the assistance a mother may need to manage the first feed at the breast, NICU staff may improve the delivery of DBF to these high-risk preterm infants who are most in need of its therapeutic effects.
Limitations
This study was limited in its sample size, which likely resulted in the broad CIs as seen with DBF at first oral feed and recreational drug use. The sample size may have been too small to identify significant risk factors that might have otherwise influenced the infants' receipt of DBF at discharge. Since this investigation was retrospective, the data available to the researchers were limited, resulting, for example, in having to infer the cause of breastfeeding cessation from the charts.
Conclusion
Feeding a preterm infant is a challenge even for mothers with a predetermined resolve to breastfeed. Because breastfeeding is an efficient and cost-effective therapeutic approach to lessen the morbidity associated with preterm birth, it is essential that we identify mothers who need support in achieving their breastfeeding goals. This study supports the infant's first oral feed as a critical window during which mothers must be encouraged to put their baby to breast. By preparing mothers for this first feed through education, reinforcing milk expression practices, and facilitating skin-to-skin contact NICU staff may improve the chances that infants will receive DBF as they leave the hospital.
Footnotes
Acknowledgments
The authors would like to thank Sarah Phillips, Kelly Bishop, Taylor Yuzdepski, and Meagan Jackson for their efforts in the initial data collection phase for this project.
Disclosure Statement
No competing financial interests exist.