
Abstract
Abstract
Objectives:
This systematic review aimed to evaluate the association between breastfeeding and breathing patterns in children.
Materials and Methods:
We searched PubMed, EMBASE, Web of Science, CINAHL, and the Cochrane Central Register of Controlled Trials for publications from inception to October 1, 2017. The breastfeeding duration and period of exclusive breastfeeding were selected as primary outcomes. The odds ratio (OR) and 95% confidence interval (CI) were calculated. A meta-analysis was conducted to synthesize the evidence. The Newcastle-Ottawa Score was used for quality and comparability assessment.
Results:
Of the 54 articles identified, three observational studies met the inclusion criteria for this meta-analysis, representing 1,046 participants. The results of the meta-analysis revealed that the prevalence rate of mouth breathing (OR = 2.04; 95% CI, 1.26–3.31; p = 0.004) was significantly higher in subjects who were breastfed for less than 6 months, but no significant difference was observed within the periods of exclusive breastfeeding (6 months or less) (OR = 1.27; 95% CI, 0.73–2.21; p = 0.40).
Conclusion:
We found only limited evidence about the association between breastfeeding and breathing patterns. However, the current evidence supports the association between breastfeeding and childhood breathing patterns. Based on this review, we found that the frequency of normal nasal respiration increases with the duration of breastfeeding. The methodological quality of the studies included was moderate. Thus, future studies should aim to correct the confounding factors related to breathing patterns, to use standardized diagnostic criteria of mouth breathing, and to conduct a prospective research to reduce the recall bias.
Introduction
E
The mouth-breathing syndrome is defined as when a child has mixed breathing or exclusive oral breathing. Normal nasal breathing is an unequaled way of providing optimal air for the healthy growth and development of infants; it is also an integral part of the craniofacial growth process, which has a significant impact on the growth and development of the craniofacial skeleton.5–7 Furthermore, abnormal mouth breathing patterns are more predisposed to sleep disorders, learning difficulty, atopic dermatitis, and allergic rhinitis.8–11
The results of recent systematic literature reviews reported that breastfeeding could affect the occlusion of the teeth.12–16 Breastfeeding stimulates optimal craniofacial development by inducing intense muscle activity, including proper lip closure, mandibular functional movement, and precisely locating the tongue against the palate. The mechanism of breastfeeding in newborn infants is a complicated action that involves sucking, breathing, and swallowing simultaneously and works in conjunction with the central nervous system. 17 During breastfeeding, the lip and tongue movements obtain milk through squeeze action, while bottle-feeding children exercise more passive motion to gain milk, which causes less stimulation to the orofacial structure.17,18
Although previous studies have suggested that mouth breathing pattern may be related to the breastfeeding duration,19–21 there is no firm evidence supporting the claim that breastfeeding duration affects the breathing patterns in children. Therefore, the present systematic review and meta-analysis aimed to examine the current evidence on the possible effects of breastfeeding on the breathing patterns and to assess the methodological quality of the individual studies.
Materials and Methods
Protocol
This systematic review was conducted under the recommendation of the MOOSE (Meta-analysis of Observational Studies in Epidemiology) guidelines for design, implementation, and reporting. 22
Eligibility criteria (PICOS)
The systematic review was designed to answer the following focused questions: “Is there a relationship between breastfeeding duration and breathing patterns?” and “Is there a relationship between exclusively breastfeeding and breathing patterns?” The PICOS (population, the exposure or intervention, comparisons, outcome, study design) method was used to define the following eligibility criteria: P (population) comprised children who are breastfed or not breastfed by their mother without age restrictions, I (exposure or intervention) is related to the duration of breastfeeding, C (comparisons) were the measurement values of breastfeeding duration and periods of exclusive breastfeeding, O (outcomes considered) is the difference in breathing patterns of children, and S (study type) in not limited. Eligible articles were assessed according to the following inclusion criteria: (1) studies related to the association of breastfeeding and breathing patterns, (2) studies that have clearly defined criteria for assessing breathing patterns, and (3) studies evaluating any duration of breastfeeding or periods of exclusive breastfeeding. The exclusion criteria were as follows: (1) studies without duration of breastfeeding assessment; (2) literature or systematic reviews, narrative review, and case reports; (3) protocols, comments, editorials, letters, and interviews; and (4) studies not conducted in human subjects.
Information sources and search strategy
Electronic search
We searched the following databases for publication articles from the earliest available date to October 1, 2017 that explore the association between breastfeeding and breathing patterns: MEDLINE, EMBASE, Web of Science, CINAHL, and Cochrane Central Register of Controlled Trials. The strategy used was a combination of Mesh terms and free text words, including “breastfeeding” [Mesh terms], “breastfeeding” [text word], “mouth breathing” [Mesh terms], “mouth breathing” [text word], and “breathing patterns” [text word]. There were no language restrictions. The detailed search strategy used in this study is shown in Appendix Table A1. The gray literature was searched using the opengrey (opengrey.eu), and unpublished or ongoing trials were identified using the electronically searching ProQuest Dissertations and thesis database, ClinicalTrials.gov, and National Research Register.
Hand search
The reference lists of the included studies and previously published articles related to the topic were screened for identification of any additional studies.
Study selection
Each identified article was independently screened by title and abstract by the two authors (D.W. and E.H.) to remove duplicate entries and studies that failed to meet the inclusion criteria. To avoid excluding potentially relevant articles, abstracts providing unclear results were included in the full-text analysis. Any disagreement was resolved by discussion. The full-text articles of the remaining studies were assessed according to the previously defined inclusion and exclusion criteria and then eligible articles were selected. The review authors were not blinded to the authors of the study, the institutions, or the publication. The references of the included articles were further checked manually. If the retrieved articles were unclear, we contacted the author by e-mail to clarify the incomplete information.
Data collection process
Two of the authors (D.W. and E.H.) independently extracted the data from each included article into the predesigned data collection forms on Microsoft Excel: (1) study identification: first author's name, year of publication, and country; (2) study design; (3) population (participants): sample size, mean age, and numbers of male and female participants; (4) diagnosis criteria of breathing patterns; (5) method of assessing the breastfeeding information; (6) exposure or intervention; and (7) primary outcome measures and time of assessment. Discrepancies were resolved by discussion.
Data items
The primary outcome measures were duration of breastfeeding and periods of exclusive breastfeeding. When the data were not provided, the calculations were performed based on the raw data reported in the article if present, or we contacted the author by e-mail to clarify the incomplete information.
Risk of bias in individual studies
Two of the authors (D.W. and E.H.) independently evaluated the risk of bias of the enrolled studies in our meta-analysis using the Newcastle-Ottawa Score. 23 The observational studies included were evaluated mainly through eight methodological items. Each study can be awarded only one star for each item, with the exception of comparability, for which up to two stars can be given; thus, the maximum possible score for each study is nine stars. The quality of the studies was assessed independently by two reviewers. If they disagreed, a consensus was reached by discussion.
Summary measures and synthesis of the results
To answer the research question, the data regarding the association of breastfeeding and breathing patterns, in the form of dichotomous variables, were aggregated from the previous studies. To perform the meta-analysis, data extraction was performed based on the number of patients and the number of cases in the exposure (intervention) and the control group. The surveys on the duration of breastfeeding conducted by the included studies were not unified; thus, the breathing patterns were analyzed based on the period of exclusive breastfeeding (6 months) recommended by the WHO guideline. For the breastfeeding duration and periods of exclusive breastfeeding outcomes, a weighted treatment effect (prevalence rate) was calculated, and the results were expressed as odds ratio (OR) and 95% confidence interval (CI). We used the fixed effect model in this study because the population and exposure of the individual studies integrated into the meta-analysis were considered homogeneous. In addition, we cannot estimate the between-study variance when the number of studies conducted through the meta-analysis is very small. Hence, we used the generic inverse variance estimation method to estimate the weights in the fixed effect model. The inverse variance method is the most common method of meta-analysis and uses the inverse of the effect estimate variance as the weight of individual studies. This is an effective method if the number of studies to be combined is small, but the number of participants in each study is large. The weighted mean effect size was calculated using the RevMan software v.5.1 (Cochrane Collaboration, Oxford, UK). We provided forest plots to describe the results of the meta-analysis. A heterogeneity analysis was conducted to examine if all the effect sizes in the sample were from the same population using the I2 test and the Q statistic. A p value of Q statistic <0.05 was the indicator of heterogeneity, and the data were considered heterogeneous for I2 value higher than 40%.
Risk of bias across the studies
The funnel plot is a scatter plot showing the estimated effect sizes of the individual studies based on the sample size of the study. The interpretation of asymmetry can only be applied if at least 10 studies are included.
Additional analysis
In this study, we could not perform a subgroup analysis because of the small number of studies included.
Results
Study selection
Database searches identified 54 publications (Fig. 1). After eliminating duplicates, 45 articles were selected; 21 of these were excluded after the screening of titles and abstracts. A total of 21 articles were reviewed for eligibility by assessing the full text. The reasons for the study exclusion during the final review were as follows: not related with the topic (n = 9), evaluation on the impact of breastfeeding on malocclusion (n = 8), evaluation on the impact of breastfeeding on temporomandibular disorder (n = 1), evaluation on the impact of breastfeeding on otitis media (n = 1), and review and note (n = 2). We included the remaining three articles for quantitative and qualitative analyses.19–21
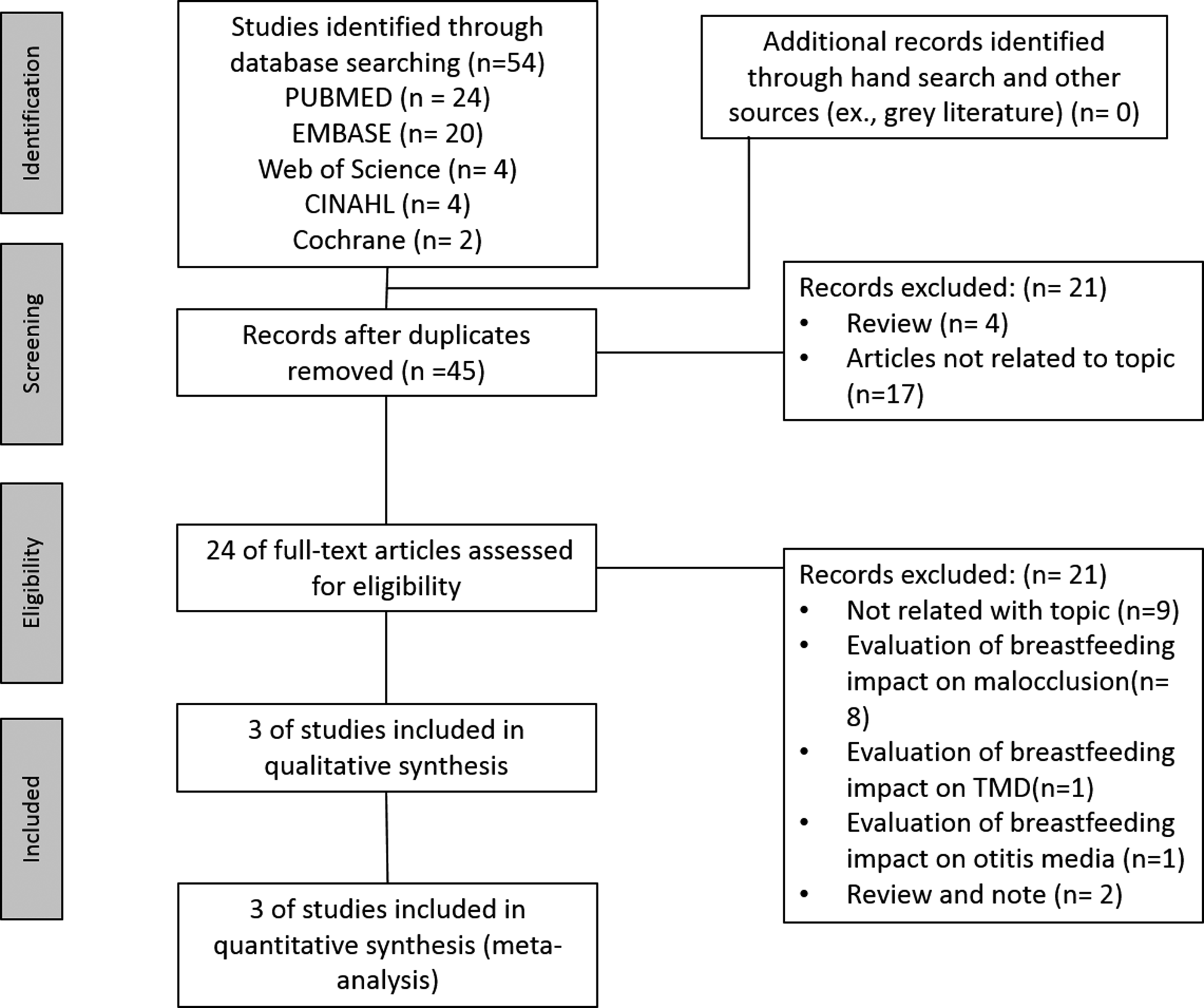
Flow diagram for identification of relevant studies.
Study characteristics
Study design and population
The main characteristics of all included studies are shown in Table 1. Included studies were published between 2005 and 2014. All trials were considered as observational studies, including 1,046 participants. Most of the participants in the included studies were between the ages of 3 and 9 years. All three studies included were conducted in Brazil.
Type of exposures
Most studies have been surveyed about breastfeeding duration; two among those studies surveyed examined the periods of exclusive breastfeeding.
Type of outcome measure
The included studies evaluated about breastfeeding duration and/or periods of exclusive breastfeeding. Two trials investigated the breastfeeding duration and/or periods of exclusive breastfeeding, while one trial included only breastfeeding duration. The descriptions of the diagnostic criteria for breathing patterns and the measurement tools for assessing breastfeeding information were reported clearly by the authors of all studies. The three studies included a total of 1,046 participants, of which the mouth breather group consisted of 500 persons, while the nasal breather group comprised 546 persons. The methods for diagnosing the breathing pattern included otorhinolaryngological evaluation or clinical examination such as the Glatzel mirror test, water test, and lip closure assessment. The information related to breastfeeding duration was obtained mainly from questionnaires.
Synthesis of results
Effect of breastfeeding duration on breathing patterns
The three included studies provided three effect sizes that examined the effect of the duration of breastfeeding on the types of breathing patterns. Subjects breastfed for less than 6 months showed increased levels of mouth breathing patterns (OR = 2.04; 95% CI, 1.26–3.31; p = 0.004) compared with those breastfed more than 6 months under the fixed model (Fig. 2). The present meta-analysis found that children who were breastfed for up to 12 months presented 1.78 times more risk of mouth breathing pattern than those breastfed for more than 12 months. Subjects breastfed for less than 24 months showed increased levels of mouth breathing patterns (OR = 1.63; 95% CI, 1.20–2.21; p = 0.002) compared with those breastfed for more than 24 months under the fixed model. Under the fixed effects model, the Higgin's I2 test and the Q statistic for heterogeneity testing explained the heterogeneity in the effects of breastfeeding duration on the breathing patterns, with I2 = 45.0% and chi-square = 3.36 (p = 0.16), respectively.
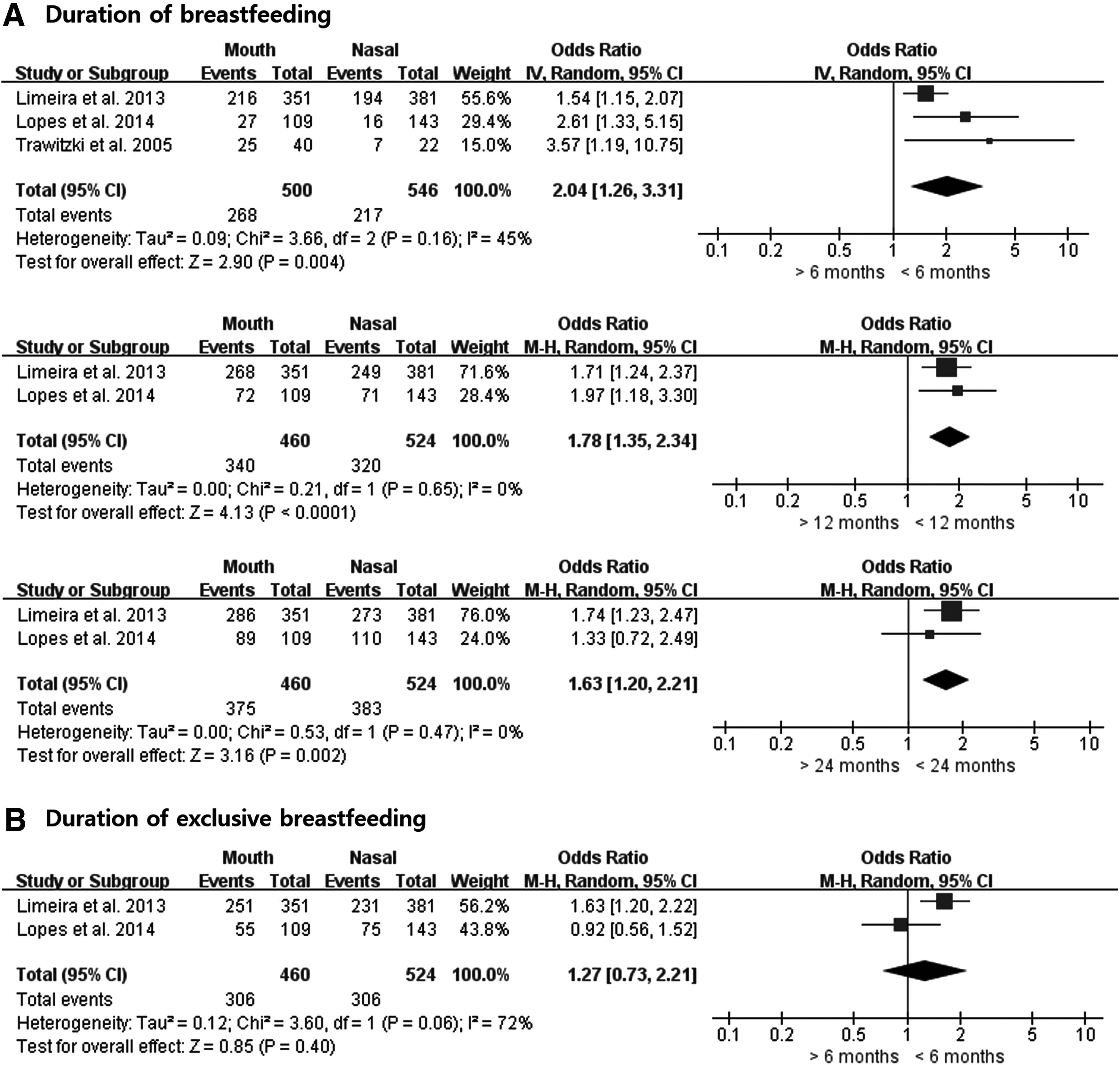
Effect of periods of exclusive breastfeeding on breathing patterns
The three included studies provided two effect sizes that examined the effect of the periods of exclusive breastfeeding on the types of breathing pattern; however, no significant difference was observed between the subjects breastfed for more than 6 months or less (OR = 1.27; 95% CI, 0.73–2.21; p = 0.40) and subjects who had breastfed for more than 6 months under the fixed model (Fig. 2). Under the fixed effects model, the Higgin's I2 test and the Q statistic for heterogeneity testing explained the heterogeneity in the effects of breastfeeding duration on the breathing patterns, with I2 = 72.0% and chi-square = 3.60 (p = 0.06), respectively.
Risk of bias within individual studies
The quality assessment of observational trials using the Newcastle-Ottawa Score Tool is summarized in Table 2. All three included studies were described as observational studies. The representation of the exposed individuals and the selection of the nonexposed individuals were considered appropriate in all included studies. Although the ascertainment of the exposures was considered as inadequate in all cohort studies because they were conducted through questionnaire surveys, it is unlikely that the survey method used to evaluate the breastfeeding duration will increase the risk of bias. Demonstrations that malocclusion was not present at the start of study were not reported in all included studies. With regard to comparability, the exposure of interest (mouth breathing) was adjusted only for age factor, not for other confounding factors. The appropriate assessment of outcome was used in all observational studies, including clinical test, otorhinolaryngological examination, or Moyer's methods, for evaluating a lack of lip seal. A follow-up duration was long enough for outcomes (mouth breathing) to occur in all included studies.
Criteria: (1) Representativeness of the exposed cohort. (2) Selection of the nonexposed cohort. (3) Ascertainment of exposure. (4) Demonstration that outcome of interest was not present at start of study. (5) Comparability of cohorts on the basis of the design or analysis, (5a) for age factor and (5b) for additional factor. (6) Assessment of outcome. (7) Duration of follow-up period. (8) Adequacy of follow-up.
Discussion
This systematic review examines the current evidence on the possible effects of breastfeeding on the development of breathing patterns. Our findings suggested that the duration of breastfeeding is related to the breathing patterns. Possible explanations for such a relationship are as follows. The forward movement of the mandible and the tongue up and down movements promote the development of balanced muscles, while the bottle feeding promotes muscle action to contract the buccinator and orbicularis oris muscles and narrow the maxilla. Electromyography studies have confirmed that muscle activation is different between breastfeeding and bottle feeding, with less use of the mentalis and masseter muscles and more use of the buccinator and orbicularis oris muscles in bottle feeding.24–26 A recent meta-analysis found that the risk of posterior crossbite increases as the duration of breastfeeding decreases.14,27 This is the result of the excessive action of the buccinator muscles and the abnormal location of the tongue and lack of motor function. Human infants are able to experiment with different sucking pressure and different lip, tongue, and jaw movements to maximize the amount of milk they need to obtain or reduce an uncomfortably fast flow. These compensations will be adaptive for the infant and comfortable for the mother, but this compensation does not occur for bottle feeding. If breastfeeding is sure to affect the breathing pattern and occlusion, the importance of breastfeeding should be more emphasized to prevent side effects, such as long face syndrome, from abnormal oral breathing habits.
However, for the periods of exclusive breastfeeding, the results were different and homogenous conclusions could not be reached. In this study, only two studies have reported on exclusively breastfeeding,19,20 and the results were not in the same direction, so we could not find a possible association with breathing patterns.
Infants take breathing breaks whenever they need to to maintain normal blood oxygen levels, as long as the flow of milk is under their control. This ability to self-regulate is one of the reasons that physiology stability is greater during breastfeeding than during bottle feeding. However, the studies included in this review did not reveal the breathing patterns during breastfeeding, as it measured the effects of breathing patterns after breastfeeding in children aged 3 to 9 years. The sample sizes of studies included were large and representative, with the smallest sample being 62 and the largest sample being 732. For enhancing the reliability of research, two studies have attempted to measure the sample size. All the studies were performed only in Brazil. Thus, further research is needed in other races.
This study had the following limitations. First the method of diagnosis of mouth breathing differs across studies. One study performed a clinical examination, one study performed otorhinolaryngological examination, and another study used Moyer's methods for evaluating a lack of lip seal. The problem with most studies related to breathing is that it is not easy to integrate the results between studies as no single clinical protocol is available for the diagnosis mouth breathing. However, the methods used in the studies included in this study were reliable because they analyzed breathing patterns using at least one clinical test.
Second, all the studies included in this review retrospectively collected information related to breastfeeding using self-entry questionnaires or interviews, so breastfeeding data may have a recall bias for breastfeeding periods. In addition, two studies examined the duration of breastfeeding by distinguishing the subjects exclusively breastfeeding, but one study did not distinguish between exclusive breastfeeding and breastfeeding. Therefore, future prospective research designs should be used to reduce recall bias. In addition, exclusive breastfeeding, breastfeeding, and bottle feeding should be clearly distinguished. Third, since the studies included in this review were conducted in one country (Brazil), it is important to question whether the findings reflect local environmental factors or specific genetic predisposition. Therefore, there is a need for further research in other regions and populations to ascertain if this is a universal phenomenon. Finally, the included studies did not consider the confounding factors such as environmental factors that can affect breathing patterns and genetic factors related to respiratory diseases. The observational studies are aimed at examining the association between an exposure and an outcome, but can typically be affected by residual confounding, undetected bias, or reverse causality, which may generate associations that are not reliable indicators of causality. Therefore, to provide useful information about causality and to increase the certainty, future observational studies should aim to correct the confounding factors related to breathing patterns.
Conclusion
We found only limited evidence about the association between breastfeeding and breathing patterns. However, the current evidence supports the association between breastfeeding and breathing patterns. Based on this review, we found that the frequency of normal nasal respiration increases with the duration of breastfeeding, but we could not confirm the effects of exclusive breastfeeding up to 6 months or more. The methodological quality of all included studies was moderate. Therefore, future studies should aim to correct the confounding factors related to breathing patterns, to use standardized diagnostic criteria of mouth breathing, and to conduct prospective research to reduce recall bias.
Footnotes
Acknowledgments
The authors thank J.C. Justin Lee, DDS, PhD (Head of Children's Dental Center) for his help to get an insight into the breastfeeding. The work was supported by fund of Biomedical Research Institute, Chonbuk National University Hospital.
Disclosure Statement
No competing financial interests exist.
Appendix
| Database | Detailed search strategies | Records found |
|---|---|---|
| MEDLINE/PubMed | (“breast feeding”[MeSH Terms] OR “breast feeding”[All Fields]) AND (“mouth breathing”[Mesh Terms] OR “mouth breathing”[All Fields] OR “breathing pattern”[All Fields]) | 24 |
| EMBASE | (“breastfeeding”/exp OR “breastfeeding”) AND (“mouth breathing”/exp OR “mouth breathing” OR “breathing pattern”) | 20 |
| Cochrane central register of controlled trials | (“breast feeding” OR “bottle feeding”) AND (“mouth breathing” OR “breathing pattern”) | 2 |
| Web of Science | (“breast feeding”[MeSH] OR “breast feeding”) AND (“mouth breathing”[MesH] OR “mouth breathing” OR “breathing pattern”) | 4 |
| CINAHL | (“breast feeding”[MeSH] OR “breast feeding”) AND (“mouth breathing”[MesH] OR “mouth breathing” OR “breathing pattern”) | 4 |
Mesh terms, search terms, and combinations of the two were used for each database search.
There were no restrictions regarding language, setting, or geographic area of study. Ultimately, 54 records were found, 24 from MEDLINE/PubMed, 20 from EMBASE, 2 from the Cochrane Library, 4 from the Web of Science, and 4 from CINAHL. Studies were further selected according to the inclusion criteria listed in the Material and Methods (Fig. 1).
OR, odds ratio.