
Abstract
Abstract
Objective:
The objective of this study was to evaluate the analgesic effects of maternal milk odor on newborns.
Materials and Methods:
We searched the literature in PubMed, MEDLINE, CINAHL, EMBASE, Web of Science, and the Cochrane Central Register of Controlled Trials (CENTRAL) and collected all the randomized controlled trials (RCTs) investigating the effects of maternal milk odor versus scentless or other odors on procedural pain in newborns. The quality of included studies was assessed by the Cochrane Collaboration Risk of Bias tool. A meta-analysis was undertaken with the Review Manager 5.3 software and Stata version 11.0. Subgroup comparisons were prespecified according to the types of control groups.
Results:
Eight RCTs included a total of 453 participants. The results of meta-analysis showed that compared with the scentless group, the maternal milk odor group had lower pain scores during blood sampling (standardized mean difference, −0.81; 95% confidence interval [95% CI], −1.18 to −0.44; p < 0.001) and shorter crying time afterward (mean difference, −8.10; 95% CI, −15.46 to 0.73; p = 0.03). The maternal milk odor group had lower heart rate variability and oxygen saturation variability during and after a procedure, compared with both the scentless group and the vanilla group. However, no significant difference was identified in the mean heart rate and mean oxygen saturation in terms of the maternal milk odor group compared with amniotic fluid odor or mother's scent. The maternal milk odor group versus the formula milk odor group had shorter crying duration and lower levels of salivary cortisol after sampling.
Conclusions:
Maternal milk odor appears to play an analgesic role in newborns. However, more high-quality studies are needed to confirm and quantitate the effect.
Introduction
M
Research shows that when breastfed newborns are exposed to the scent of human milk from an unfamiliar mother and to the odor of an unfamiliar formula milk simultaneously, they respond to the former one more actively. 8 Even bottle-fed newborns who have never had contact with maternal milk directly show a preference for the scent of maternal milk over an unfamiliar formula milk scent that resembles the one they have consumed since birth. 9 However, it is hard to define the properties in maternal milk odor that attract newborns.
One view suggests that these properties are due to prenatal learning or phylogenetic inheritance. 8 Anatomically, newborns already have a reasonably well-developed olfactory system in the womb. 10 Olfaction originates from the interaction of ciliated olfactory receptors on olfactory sensory neurons and odorant molecules; when stimulated by odorants, the olfactory neurons are activated and, through a series of processing activities, modification, and encoding, the olfactory signals are transmitted to the olfactory cortex and then decoded to distinguish different odors. 11 In the human fetus, the ciliated olfactory receptors show a mature appearance at the 24th gestational week 10 and the olfactory marker protein can be expressed in epithelia of the nasopharynx at the 28th gestational week 12 ; hence, they form a perception of amniotic fluid odor in the womb. 13 Moreover, both amniotic fluid and maternal milk originate in the mother's blood system,11,14,15 and one study shows that maternal milk is similar to amniotic fluid in the content of seven fatty acids present consistently, 10 which probably encourages newborns to display orienting movements toward maternal milk after birth and to adapt to the transition to life outside the womb through olfactory cues. 16
As shown in substantial evidence, newborns could distinguish maternal milk odor from nonmaternal milk odor, amniotic fluid odor, and body scent, due to the capacity for early olfactory detection, discrimination, and memory.17,18 To date, based on the mature olfactory system, accumulating research has applied odor stimulation to newborns as a nonpharmacological intervention, looking to the effects of different odors on physiology and behavior of newborns. Some studies19–21 show that premature infants have increased sucking activity and consume more milk when stimulated by breast milk odor rather than formula milk odor. The odor of rose could reduce apnea attacks and decrease the heart pulse rate in premature infants. 22 In addition, numerous randomized controlled trials (RCTs) discuss the analgesic effects of maternal milk odor on newborns during blood sampling, comparing it with other odors such as amniotic fluid odor and mother's scent. However, to our knowledge, there have been no systematic reviews in the literature to evaluate the odor of maternal milk to lessen procedural pain in newborns.
Therefore, the objective of this study is to summarize and evaluate the analgesic effects of maternal milk odor on newborns and to establish stronger evidence to guide clinical practices and further study in the future.
Materials and Methods
Search strategy
We searched relevant literature comprehensively from inception to September 2017 in the following databases: PubMed, MEDLINE, CINHAL, EMBASE, Web of Science, and the Cochrane Central Register of Controlled Trials (CENTRAL). A combination of medical subject headings (MeSH) and free words was used in searching, as follows: (“Infant*” OR “Infant*, Newborn” OR “Newborn Infant*” OR “Newborn*” OR “Neonate*”), (“Milk, Human” OR “Breast Milk*” OR “Milk, Breast” OR “Human Milk”), and (“Odorant*” OR “odor*” OR “odour*” OR “smell” OR “scent”). We also screened references cited in included studies for acquiring additional literature to avoid omission.
Selection criteria
We created the following inclusion criteria: (1) types of studies: an RCT of the effects of maternal milk odor on pain responses in newborns; (2) types of populations: stable premature infants who were born at <37 weeks and >28 weeks; or healthy, full-term infants who were born at <42 weeks and >37 weeks of gestational age who underwent a blood procedure; (3) types of interventions: a maternal milk odor group versus a control group exposed to no scent, amniotic fluid odor, mother's scent, vanilla odor, and formula milk odor during blood sampling; and (4) types of outcome measures: involved in at least one outcome of validated pain measures, heart rate, oxygen saturation, crying duration, and salivary cortisol.
Exclusion criteria
(1) We excluded multimodal interventions that combined with other sensory stimulation. (2) We excluded literature that was not in English.
Data extraction
Two investigators (S.Y.Z., F.S.) screened the literature and extracted data independently, in line with the inclusion and exclusion criteria. A data extraction form was created, including general information (author list, published years, and published country), characteristics of the participants (sample size and types of populations), intervention and control groups (the details of measures and intervening time), and outcome assessment. A cross-check was made after the data extraction; when disagreements appeared, a third investigator (J.L.) engaged in a discussion.
Assessment of risk of bias
Two investigators (S.Y.Z., F.S.) assessed the quality of included studies independently by using the Cochrane Collaboration Risk of Bias tool. Similarly, a third investigator (J.L.) was consulted if there was any disagreement. The assessment included random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias with low risk, unclear risk, and high risk to be defined.
Data analysis
We performed data analysis, using Review Manager 5.3 software and Stata version 11.0. Owing to the heterogeneity of interventions among studies, we used a random-effects model directly to obtain a more conservative assessment of the outcomes. Statistical parameters included the mean difference (MD) or standardized mean difference (SMD) with 95% confidence interval (95% CI) due to the continuous variables. We calculated MD when the outcome was measured by the same instrument; we reported SMD when different scales were used for the same outcome (e.g., pain). I 2 was used to assess heterogeneity. In addition, we prespecified subgroup comparisons based on the types of control groups to determine whether significant differences would exist in the outcomes of maternal milk odor stimulation compared with every other odor.
Results
Results of the search
We obtained 261 records from the databases and added 1 record through other sources. After removing duplications, 107 articles were retained. Of these, 82, regarding reviews or irrelevant literature, were excluded through reading the title and abstract, leaving 25 full-text articles. Finally, we selected eight studies. The process of study screening is shown in Figure 1.
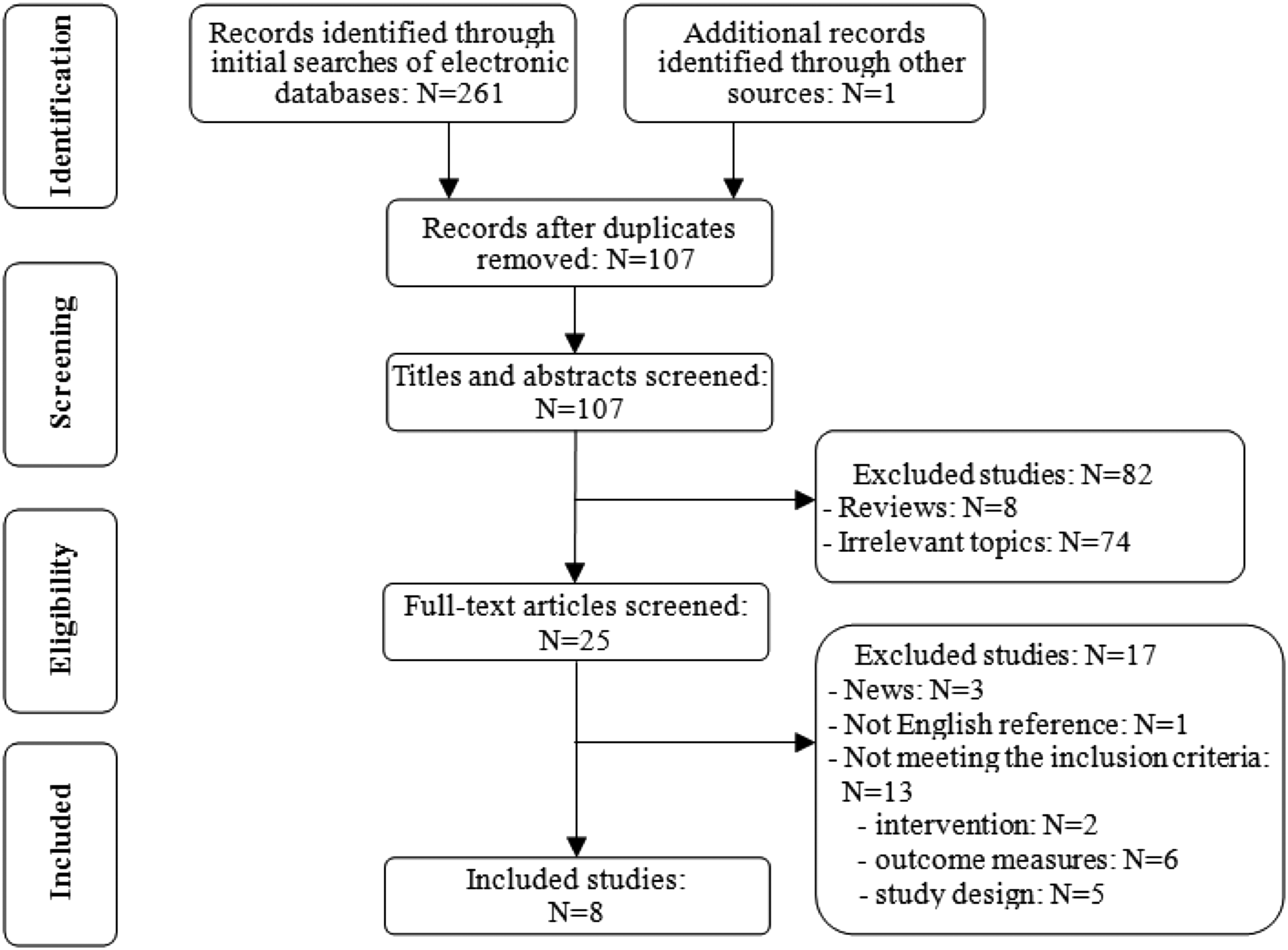
Flow diagram of studies identified, included, and excluded.
Detailed characteristics of included studies
The eight studies18,23–29 we included were all RCTs that were published in France, 23 Turkey,18,25 Iran,24,26,27 Japan, 28 and Switzerland. 29 We integrated the information of two studies24,26 because they were by the same authors with the same study conditions but different outcome domains. A total of 453 newborns were engaged, including 303 premature infants and 150 full-term infants. Three studies23,24,26 were conducted by venipuncture, the remaining studies by heel stick. The time for intervention ranged from several minutes before sampling to several minutes afterward. The amount of liquid that gave off odors ranged from one drop to 10 mL, and the odors were given via odor diffuser, 23 sterile sponge, 18 clean cotton,24,26 filter paper, 27 cotton pad, 29 or Ookie doll. 18 The detailed characteristics of the included studies are summarized in Table 1.
DAN, Douleur Aiguë du Nouveau-né; NIPS, neonatal infant pain scale; PIPP, premature infant pain profile.
Methodological quality of included studies
The methodological quality of the included studies is presented in Figure 2. Seven studies described the methods of randomization and allocation concealment in detail, which, respectively, used an opaque envelope, 25 the computer system,18,23 the Random list software,24,26 a selected box number, 27 and the random number table 29 ; the remaining two studies only mentioned that they were RCTs but did not give any information about the methods. Only one study 23 reported blinding participants and personnel, which is sometimes difficult to achieve in behavioral interventions. For blinding of the outcome assessment, three studies23,25,27 showed that the assessors were masked about the research purpose, whereas the remaining studies did not mention blinding. In addition, none of the 8 included studies had attrition bias, reporting bias, or other bias.
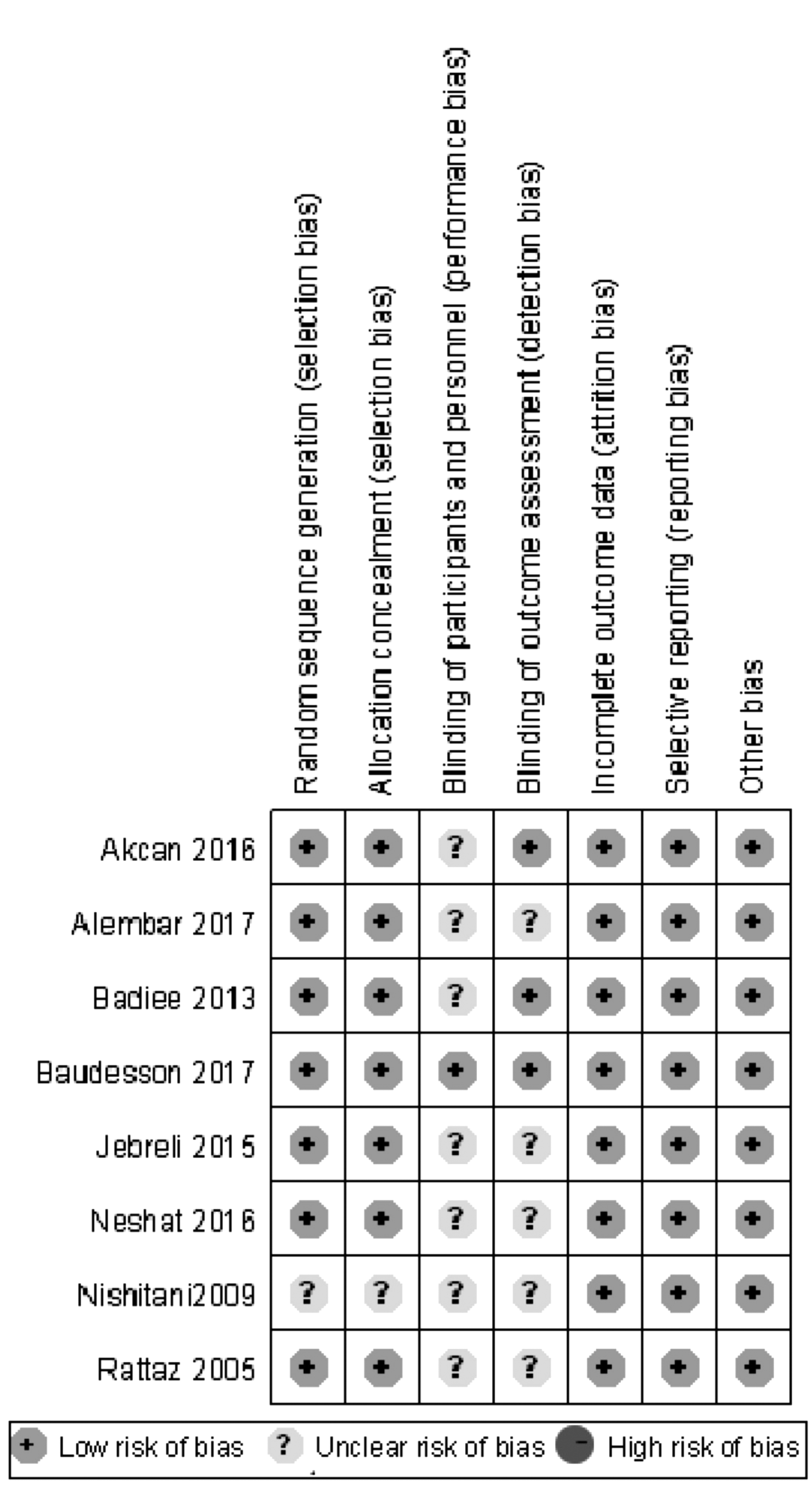
Risk of bias for the included studies.
Effects of the interventions
We summarized the effects of maternal milk odor on newborns not only during blood sampling but also after blood sampling. To define the effects of maternal milk odor compared with every other odor, we created subgroups for control groups, including a scentless group, an amniotic fluid group, a mother's scent group, a vanilla odor group, and a formula milk odor group.
Outcome during blood sampling
Four studies18,23,25,26 reported on the pain score during blood sampling, in which pain was measured by the premature infant pain profile, neonatal infant pain score, and Douleur Aiguë du Nouveau-né scale. The pain scores were statistically significantly lower in the maternal milk odor group than in the scentless group (SMD, −0.81; 95% CI, −1.18 to −0.44; p < 0.001). The pain scores were also lower in the maternal milk odor group than in the amniotic fluid odor group (SMD, −0.14; 95% CI, −0.54 to −0.27; p = 0.52), mother's scent group (SMD, −0.47; 95% CI, −1.09 to −0.14; p = 0.13), and vanilla odor group (SMD, −0.29; 95% CI, −1.15 to 0.56; p = 0.050) but not statistically significantly different. The results appear in Table 2.
95% CI, 95% confidence interval; NA, not applicable; SMD, standardized mean difference; MD, mean difference.
With regard to the mean heart rate during blood sampling, the statistically combined results of the two studies18,25 showed that no significant effects were observed comparing the maternal milk odor with the scentless, amniotic fluid odor, mother's scent, or vanilla odor groups (Table 2). However, Neshat et al. 24 also reported on the heart rate variability during blood sampling and got a significant result in the maternal milk odor group compared with the vanilla odor group (MD, −3.53; 95% CI, −3.74 to −3.32; p < 0.0001) and the scentless group (MD, −3.71; 95% CI, −4.04 to −3.38; p < 0.0001). Newborns in the maternal milk odor group showed a significant difference in the oxygen saturation variability compared with the vanilla odor group (MD, −0.97; 95% CI, −1.92 to −0.02; p < 0.0001) but no significant difference in the other three groups. Neshat et al. 24 also showed that the variability in oxygen saturation in the maternal milk odor group was significantly lower than in the vanilla odor group (MD, −0.78; 95% CI, −1.01 to −0.55; p < 0.0001) and scentless group (MD, −0.56; 95% CI, −0.79 to −0.33; p < 0.0001).
As shown in Table 2, there was no statistically significant difference in crying duration among newborns during blood sampling when comparing the maternal milk odor group with every other group.
Outcome after blood sampling
Compared with the scentless group, the result of pain score after blood sampling in the maternal milk odor group is displayed in Table 3 (MD, −0.38; 95% CI, −0.77 to 0.00; p = 0.05). To get a more accurate result, we performed analysis again, using Stata version 11.0 and obtained the p-value of 0.051. Thus, our meta-analysis showed no significant effect of maternal milk odor on pain in newborns after blood sampling, compared with all the other odors.
95% CI, 95% confidence interval; NA, not applicable; SMD, standardized mean difference; MD, mean difference.
The maternal milk odor group showed a significant result in mean oxygen saturation (MD, −0.97; 95% CI, −1.92 to −0.02; p = 0.05) only when compared with the vanilla odor group. There was no significant difference in the mean heart rate and mean oxygen saturation after blood sampling between the maternal milk odor group and the other groups. However, one study 24 found a significant difference in the variability of heart rate and oxygen saturation by comparing the maternal milk odor group with the vanilla odor group and the scentless group. The result is shown in Table 3.
With regard to the duration of crying among newborns after blood sampling, a significant result existed only in the maternal milk odor group compared with the scentless group (MD, −8.10; 95% CI, −15.46 to 0.73; p = 0.03) and formula milk odor group (MD, −2.50; 95% CI, −4.26 to −0.47; p = 0.005). Comparing the maternal milk odor group with mother's scent, vanilla odor, and amniotic fluid odor groups produced no significant results.
Our meta-analysis also recorded the level of salivary cortisol in newborns after intervention (Table 3). The results showed that there was a statistically significant difference between the maternal milk odor group and the formula milk odor group (MD, −7.60; 95% CI, −11.83 to −3.37; p = 0.0004), but no statistical significance was observed in comparison with the scentless group.
Discussion
The findings of our meta-analysis were relatively comprehensive because of the diversity of control groups. Compared with a scentless environment, maternal milk odor reduced neonatal pain during blood sampling, decreased the duration of crying after blood sampling, and narrowed the variability of heart rate and oxygen saturation both during the intervention and after the intervention. The encouraging results seemed to verify further that maternal milk odor was one type of olfactory stimulation that could elicit emotional behavior in newborns.16,30,31 When newborn babies are exposed to their favorite milk odor, the olfactory information is delivered to the hypothalamus and the hippocampus, whose mechanisms mediate the emotional and motivational aspects of odors and induce physiological and behavioral effects of odors, 32 perhaps calming them.
Our study showed no significant improvement in the physiological parameters of the newborns under the maternal milk odor stimulation, when compared with the amniotic fluid odor and the mother's scent stimulation. May be all three odors are familiar and attractive to them. Therefore, the results were certainly not difficult to explain. Maternal milk odor could stabilize newborns' heart rates and blood oxygen saturation better than a vanilla odor. However, one study, 13 using near-infrared spectroscopy (NIRS), showed an opposite result of our study, concluding that the changes in blood flow to the brain from the vanilla odor were greater than those from the colostrum odor. Indeed, some studies33–35 have emphasized the calming effects of vanilla odor on newborns, but more high-quality research is needed to validate the difference between maternal milk odor stimulation and vanilla odor stimulation. Furthermore, another NIRS study 36 demonstrated that the changes in oxygenated hemoglobin from maternal milk stimulation were significantly different from those from formula milk odor, which was consistent with our results. Compared with formula milk odor stimulation, maternal milk odor stimulation seemed to support shortening the crying time and significantly reducing the salivary cortisol level after neonatal blood collection.
The number of included studies was limited, but studies have been published mostly in recent years, reflecting the fact that researchers are paying more and more attention to the effect of maternal milk odor stimulation on newborns. To our knowledge, this is the first meta-analysis of the effect of maternal milk odor stimulation on newborns. Although the total number of trials included was small, only RCTs were selected and supposed to improve the quality of the meta-analysis in one way. All 8 articles had a low risk of attrition, reporting, and other biases, and of these, seven studies recounted the method of randomization and allocation concealment. In principle, studies that were not perfected in the details of blinding method should not be considered for inclusion in a meta-analysis to ensure its scientific validity. However, we found that the current literature in the considered domain had some shortcomings in blinding methods in general after being systematically reviewed. In terms of the blinding method, blinding of participants and personnel was difficult to realize, but that of outcome assessment could be manipulated because odor stimulation belongs to behavioral intervention. Nevertheless, researchers should perform with an eye to the design of the blinding method to increase the experimental standard of future studies and to come to more reliable and valuable conclusions.
We also found some other limitations in relevant studies in this domain. The studies we included used the odor of maternal milk that originated from the infants' own mothers. More studies could explore the effect of maternal milk odor on the procedural pain in newborns, comparing with breast milk odor from unrelated lactating women; this should be further investigated in the future. In contrast, Romantshik et al. 37 mentioned that early exposure to amniotic fluid or breast milk odor in the sensitive period of neonatal olfactory learning contributed to improvement of the breastfeeding outcome, guiding future studies to pay more attention to the long-term effects of maternal milk odor stimulation such as the duration of breastfeeding and the bonding relationship between the infant and the mother.
Some limitations also exist in our meta-analysis. We did not assess the outcome measures such as feeding behavior, time for transition to oral feeding, and the duration of hospitalization, which some researchers explored.20,35,38 The number of relevant studies was also reduced because we limited the language to English. In addition, it would be worth examining whether full-term newborns or premature infants (>28 weeks) react differently under different odor stimulation, and, in particular, whether some are more reactive to the odor of milk than to amniotic fluid, despite them having a mature olfactory system. 12 However, we could not perform the analysis above due to the number limit of the included studies and the diversity of control groups; this should also be further investigated when there are more studies in the future. The difference in the duration and intensity of odorants could also affect the results of our meta-analysis more or less, leading to the use of the random effects model for direct statistical analysis. Opposite views were put forward about whether the intensity of odorants affected the changes in cerebral blood flow in two NIRS studies.13,36 Therefore, future research on the specific effects of different intensities of odorants on newborns is also awaited.
The importance of maternal milk to newborns for their growth and development is beyond any doubt, and their ability to identify maternal breast milk odor could lay the foundation for their attachment and socialization39,40 and add to the richness of emotional cognition.11,41,42 The meaningful conclusions in our meta-analysis were small but seemed to affirm the analgesic role of maternal milk odor in newborns to a certain extent and could lead researchers to pay more attention to newborns' responses to olfactory stimulation especially of maternal milk odor. In future, more RCTs with high-quality design and a larger sample are needed to confirm and quantitate both the short-term and long-term effects of maternal milk odor stimulation on newborns.
Footnotes
Acknowledgments
We would like to thank Prof. Xiaomin Xiao and Prof. Jun Guo, The First Affiliate Hospital, Jinan University, for their kind suggestions for the revision of this manuscript.
Disclosure Statement
The authors declare no conflicts of interest.