
Abstract
Abstract
Background:
While breastfeeding rates have been increasing in the United States, they remain below targets set by multiple public health organizations. Lower rates are associated with certain demographic groups. We performed a retrospective chart review to examine rates of breastfeeding at the time of postpartum follow-up in a mixed-race urban cohort.
Objective:
This study was conducted to examine the proportion of women who were breastfeeding at 6–8 weeks postpartum and to determine if these proportions differed by race and insurance status.
Materials and Methods:
We identified women who delivered singleton term infants at an urban university hospital between July and December 2013. Self-reported breastfeeding status at 6–8 weeks postpartum was abstracted for all women who completed postpartum follow-up visits. Data were analyzed with logistic regression to compare rates of any or exclusive breastfeeding between women with Medicaid and private insurance.
Results:
Charts of 656 women were reviewed; 405 women completed postpartum follow-up within 8 weeks. The Medicaid population had significantly lower rates of breastfeeding even after accounting for interaction and confounding by demographic factors (any breastfeeding odd ratio [OR] 0.53, confidence interval [CI] 0.04–0.31; exclusive breastfeeding OR 0.48, CI 0.33–0.85). When stratified by race, white women on Medicaid had the lowest probability of breastfeeding of all groups (p < 0.01).
Conclusions:
Among patients delivering at an urban academic hospital, women on Medicaid were significantly less likely to breastfeed than those with private insurance. The greatest differential by insurance was seen among white women. Efforts to improve breastfeeding should focus on low-income women of all races.
Introduction
B
Baby-friendly programs which increase support and education regarding breastfeeding have likely contributed to the impressive increase in breastfeeding initiation.4–6 However, continuation of breastfeeding is essential, and even in supportive environments, about 60% of women report stopping breastfeeding earlier than they intended. 7 Multiple factors may contribute to discontinuation of breastfeeding, and most discontinuation is multifactorial. Women who do initiate breastfeeding are at the highest risk of discontinuation in the first month, with many stopping rapidly after hospital discharge. 8
Many maternal characteristics such as young age, African American race, lower socioeconomic status, and lower education have been shown to be associated with lower rates of breastfeeding continuation,9,10 although much of the literature regarding race and socioeconomic status (SES) is somewhat inconsistent. One study using data from the National Survey on Children Health has shown higher rates of breastfeeding discontinuation among women of a lower SES defined as <400% of federal poverty level. 11 However, a recent study from the National Survey of Family Growth showed the income was not a factor in breastfeeding behavior, 12 and a large study among California women found that SES had little impact compared to education level and race. 13 Similar conflicting results have been seen regarding race as well. In general, African American women are reported to have lower rates of breastfeeding when compared with white or Latina women.11,14,15 However, some studies have found that specific populations of African American women are more likely to breastfeed than other groups. 16 Breastfeeding rates and behavior by income or race differ between urban and rural settings,17–19 and one study of urban women found that African American women were more likely to intend to breastfeed than non-Hispanic white women. 20
The interaction of race and SES in health behaviors is complex and likely varies in different environments, such as urban, inner city, or rural areas. Understanding the prevalence of breastfeeding in a particular population and accurately identifying true risk factors for early discontinuation may require a focus on that given population. Development of effective interventions to change outcomes also requires that the risk factors be defined in a way that is clinically relevant and accessible to clinicians. Prior research regarding breastfeeding among urban women has often focused on race in a specifically low-income population.8,20,21 Other studies of rural women have examined SES but in racially homogenous populations. 22 Many studies examining SES and breastfeeding have stratified on reported income, but income information is not often directly available to providers. We wished to examine the relationship between socioeconomic status and early discontinuation of breastfeeding in our typical urban population, using markers and classifications that are readily available in the clinical care setting. We performed a retrospective cohort study to examine continuation of breast feeding in women receiving either Medicaid or commercial insurance at 6–8 weeks postpartum in a mixed-race, economically diverse urban population.
Materials and Methods
This retrospective chart review assessed breastfeeding among women who delivered infants at Thomas Jefferson University Hospital between July 1 and December 15, 2013. Women who delivered live-born, term, singleton infants in the study period were identified from the labor and delivery records. Women who delivered an infant at <37 weeks gestation or had multiple gestation were not considered for analysis. Among those who met inclusion criteria, outpatient records were queried, and women who completed an office visit between 6 and 8 weeks postpartum were identified and included in the study.
Our primary outcome was the proportion of women who were doing any breastfeeding or exclusive breastfeeding at the time of their follow-up office visit. Outpatient electronic medical records were abstracted to determine breastfeeding status at the time of the visit. Standard office forms used for documenting postpartum visits include a question where infant feeding is characterized in a structured format as “breast” “bottle/formula” or “both.” From these classifications, our primary outcome was defined as a three category description of breastfeeding: no breastfeeding (bottle/formula only), any breastfeeding (breast only or breast and bottle/formula), or exclusive breastfeeding (breast only). Our primary exposure variable was the patient insurance status in the pregnancy. This was defined as a dichotomous categorical variable of Medicaid (either Medicaid Health Maintenance Organization or “straight” Medicaid) or commercial insurance (any of the non-Medicaid commercial insurance payers seen in the outpatient practice). Patients without any insurance are not seen for outpatient care at this practice.
Characteristics, which have been shown in prior literature to correlate with probability of breastfeeding, were considered as possible confounders of the relationship between insurance status and breastfeeding. We abstracted demographic characteristics from the prenatal and outpatient chart. Race and ethnicity were categorized as white, African American, Asian, and Hispanic. Age and body mass index at delivery and postpartum were considered as continuous variables. Education was considered both as a multilevel variable (some high school, graduated high school, some college, graduate of college, or postcollege degree) and as a dichotomous variable (some/graduated high school and some/graduated college). Gravidity and parity were classed a dichotomous variables (any prior pregnancy and any prior deliveries).
Differential distributions of the demographic characteristics were assessed with t-tests for continuous variables and chi square testing for categorical variables. Those characteristics which were differentially distributed in the exposure and outcome categories were considered as potential confounders. Separate models were developed for the outcomes of any breastfeeding and exclusive breastfeeding. Unadjusted odds ratios for breastfeeding were calculated with logistic regression. A full model by logistic regression was estimated, including insurance status, all potential confounders, and interaction terms. Interaction effects were assessed with likelihood ratio testing, and nonsignificant terms were removed from the model. We then estimated odds ratio and 95% confidence interval for breastfeeding between insurance categories, adjusted for all confounders, and interaction effects. We used change-in-effect modeling and partial–F testing to determine which potential confounders had true effect in the model, and the final model included all significant interactions and those confounders which changed the odd ratio by a significant amount.
Reported rates of breastfeeding in the general population range from 35% to 75% depending on various demographic factors. Based on prior literature, we estimated that rates of breastfeeding would range from 40% to 60% in our patient population. We estimated that to have 80% power to detect a difference in breastfeeding rates of 40% and 55% in our Medicaid and commercially insured population, with p-values set at 0.05 for significance, we would need to have a total of 374 subjects, with 187 in each arm. Our patient population is known to have a typical postpartum follow-up rate of about 56%. Therefore, we planned to review ∼650 delivery records to ensure complete postpartum and breastfeeding data for an adequate sample of 380 subjects. All analyses were conducted in Stata Version 12 (StataCorp LP, College Station, TX). The study was approved by the Thomas Jefferson University IRB.
Results
A total of 656 women delivered term, singleton infants at our hospital in the study timeframe. Of these, 405 (61%) completed a standard postpartum follow-up visit in the typical timeframe of 6–8 weeks. All patients had documentation of their feeding method in the medical record. There were minimal missing data for any of the demographic or medial characteristics and no systemic pattern to missing data. All continuous variables were confirmed to have normal distribution.
Forty-seven percent of patients were Medicaid-insured, and 53% were African American (Table 1). Women with Medicaid insurance were younger, more likely to be of African American race, more likely to be primiparous, and less likely to be married or have attended college.
Reported as mean (standard deviation) or n(%).
BMI, body mass index.
Overall, 239 women (59%) were performing any breastfeeding, and 166 (40%) were exclusively breastfeeding at the time of the postpartum visit. Medicaid-insured patients were significantly less likely to be performing either any breastfeeding or exclusive breastfeeding than commercially insured patients (Table 2). Age, parity, education, and marital status were noted to be potential confounders. Logistic regression models accounting for both interaction and all confounders showed significantly lower odds of either exclusive or any breastfeeding in the Medicaid population, even when adjusted for race, education, parity, and marital status. Change in effect modeling and partial-F testing showed that, of these factors, race was the patient characteristic that most significantly affected the relationship between breastfeeding and insurance status and that there was significant interaction effect between race and breastfeeding.
Adjusted for age, race, parity, education, and marital status.
CI, confidence interval; OR, odd ratio.
To explore the effect of interaction between race and insurance status, a stratified analysis was performed to estimate the proportions of breastfeeding women in each race and ethnicity group, in each insurance category. The probability of any or exclusive breastfeeding was highly variable between the insurance categories and race/ethnic groups. The interaction was statistically significant across all categories, even when adjusted for other potential confounders (p < 0.01) (Figs. 1 and 2). Overall, the highest rates of exclusive breastfeeding were seen among commercially insured white women, and the highest rates of any breast feeding were seen in commercially insured Asian women. While African American women overall had the lowest rates of breastfeeding (52% any; 33% exclusive), these women had only a moderate difference in either breastfeeding category between the insurance groups. In contrast, white women overall were more likely to breastfeed (64% any; 55% exclusive), but white women on Medicaid had the lowest rates of breastfeeding of all race and ethnicity groups, and the largest differential by insurance was seen among white women. Only 24% and 22% of white women on Medicaid performed any or exclusive breastfeeding, respectively, while 76% and 64% of white women with commercial insurance were performing any or exclusive breastfeeding.
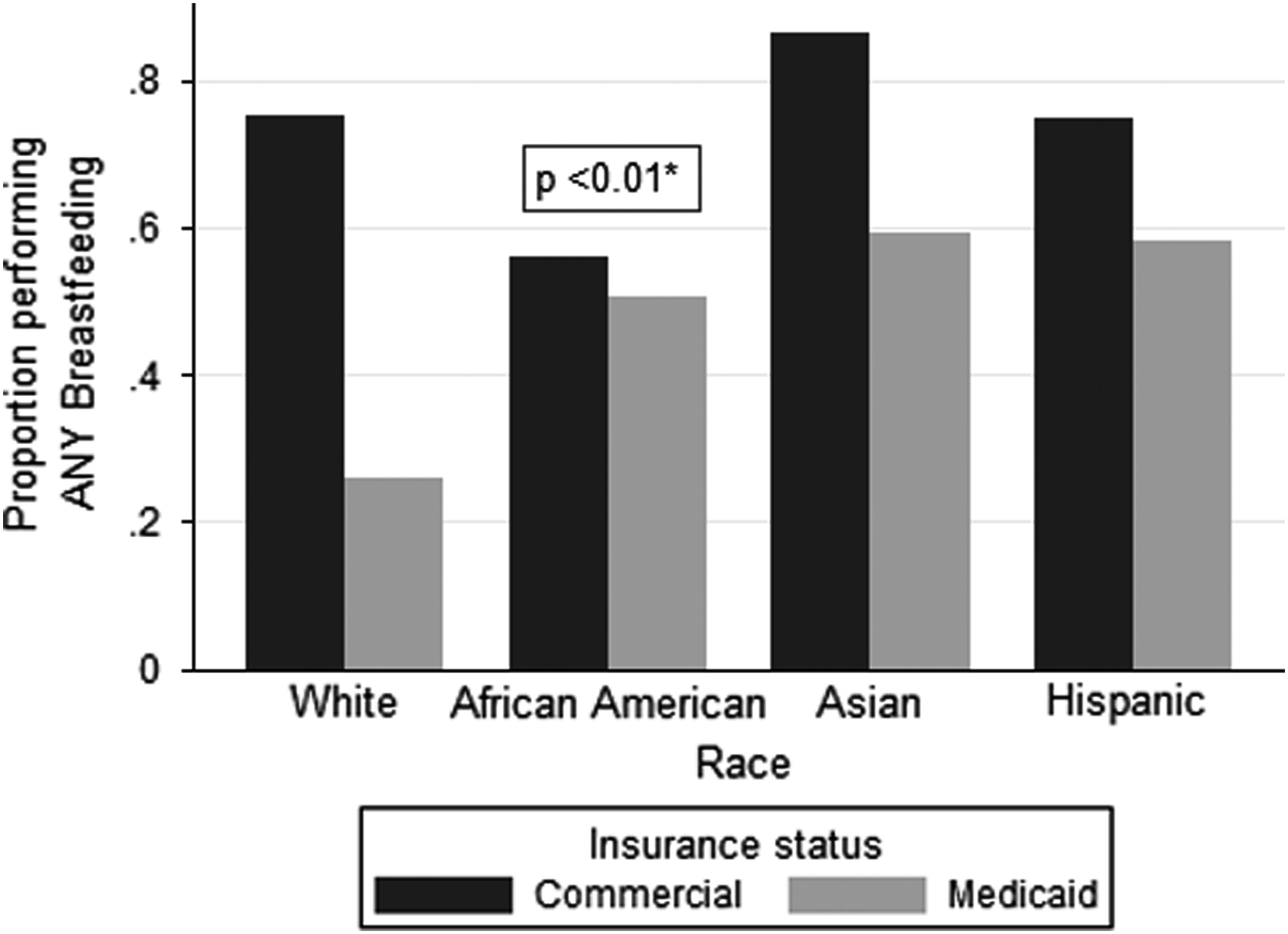
Race, insurance, and any breastfeeding. Proportion of women performing any breastfeeding differs by insurance status across race/ethnic categories. *Statistically significant difference in probability of breastfeeding between insurance categories, across multiple race/ethnic groups.
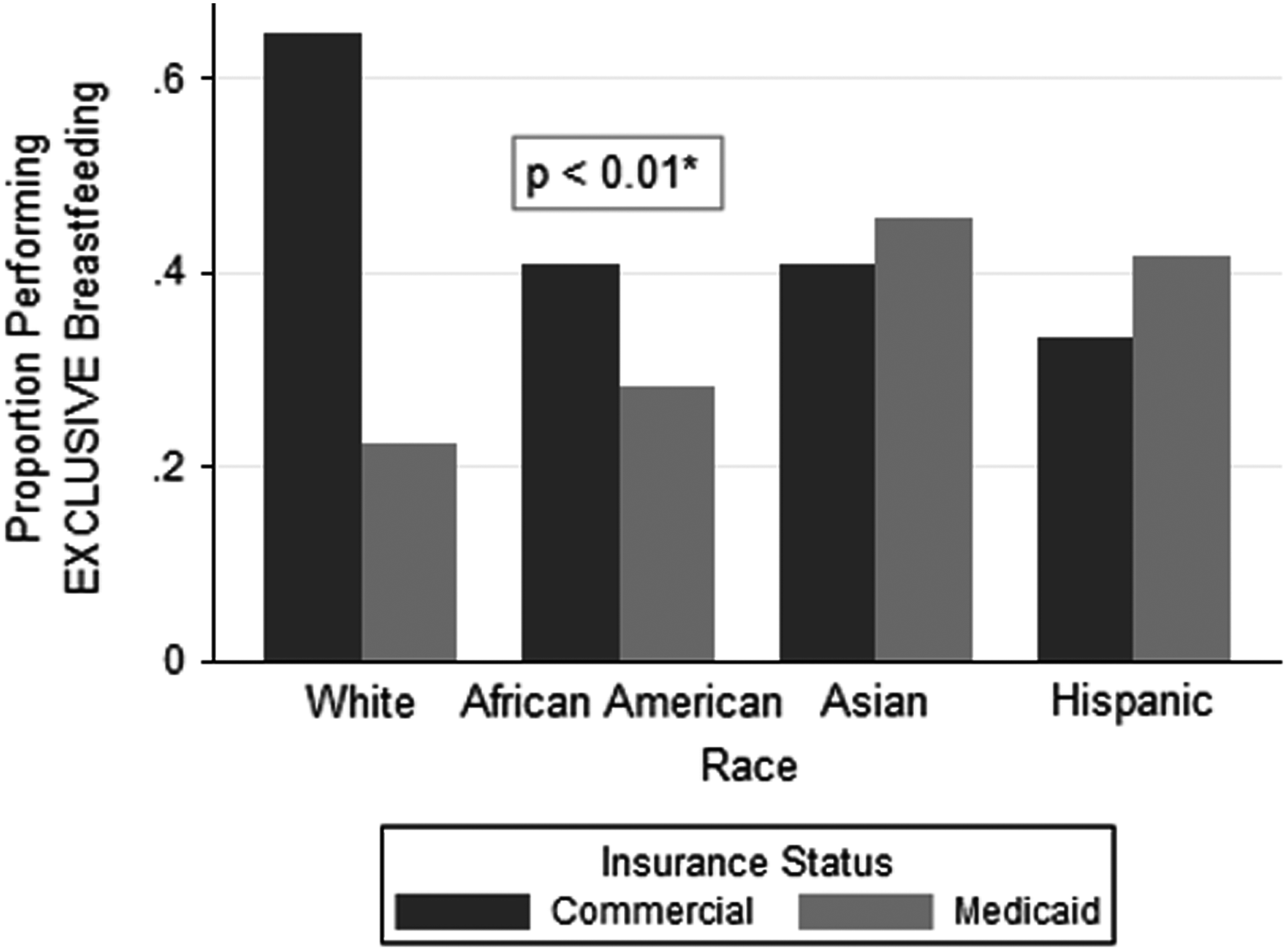
Race, Insurance, and exclusive breastfeeding. Proportion of women performing exclusive breastfeeding differs by insurance status across race/ethnic categories. *Statistically significant difference in probability of breastfeeding between insurance categories, across multiple race/ethnic groups.
Discussion
In this study, overall rates of breastfeeding at just 6–8 weeks postpartum–both any and exclusive–were slightly lower than Healthy People 2020 targets for 6 months. The endpoint of our study, at 6–8 weeks postpartum, does not give data that can be exactly compared to targets that are set for three 6–12 months. However, rates of breastfeeding attrition are highest in the first 4 weeks postpartum, 8 and average duration of breastfeeding ranges from 3 to 5 months. 15 This suggests that rates seen at our time point are likely higher than what would be found at 6 months, implying that this population, overall, falls well below the targets.
Rates of both, any, and exclusive breastfeeding were significantly lower within the Medicaid population when compared with a commercially insured population, even when controlling for other factors that have been shown to correlate with breastfeeding. This finding is consistent with prior studies showing that women of lower SES are less likely to both initiate and continue breastfeeding, confirming that this pattern is found specifically in the urban setting. Our study expands on this by finding significant difference in breastfeeding in stratified analysis combining insurance status and race. Our cohort showed that African American women overall were the least likely to breastfeed when compared with Hispanic, non-Hispanic white, and Asian women, which is consistent with prior literature. However, our stratified analysis demonstrated significant interaction between race and insurance status, finding that white women on Medicaid are actually the least likely of all groups to breastfeed, either at all or exclusively. Our finding suggests that in an urban population, the strongest risk factor for not breastfeeding is insurance status rather than race, and that within the subset of women receiving Medicaid, non-Hispanic white women are the highest risk.
Much effort is being placed into supporting and encouraging breastfeeding for all women. Several federally-funded programs provide support to hospitals to improve maternity care and breastfeeding support; these programs are focused on reducing racial and ethnic disparities in breastfeeding and specifically target low-income and minority populations.4,14 Clinical practice should encourage all women in breastfeeding, but effective interventions to improve outcomes need to accurately identify those who are most in need of education and support. Our study demonstrates that in simply considering racial and ethnic characteristics, interventions may miss more complex patterns and women who are at highest risk. The differential in breastfeeding between commercially insured and Medicaid insured white women is striking and clinically significant. If one is aware that 65% of white women are breastfeeding, but not that only 22% of white women on Medicaid are, it is easy to overlook this subpopulation and misclassify them as “low risk” simply based on race.
Women have a wide range of reasons for breastfeeding discontinuation, including perceived or actual low milk supply, perceived or actual infant breast rejection, pain, a lack of social support, need to return to work, and maternal preference. Influences on behavior vary between ethnic and racial groups and may differ by income classes.15,23 Effective interventions to improve breastfeeding need to be culturally sensitive and targeted to women's concerns. Given the heterogeneity in prior research, with conflicting data regarding which risk factors are most influential in different settings, it is essential to understand the specific population, in which one is working. In considering an urban population, within a healthcare system providing care to both Medicaid and commercially insured women, interventions should focus on women on Medicaid, and consider all racial groups in that category to be at high risk regarding breastfeeding. Support programs which build on the success of Baby-Friendly initiatives and expand them beyond the hospital setting, such as ongoing lactation counseling, home nursing, and peer support groups, could be considered by state and local Medicaid programs.
Our study does have weaknesses. By including only women who presented for their scheduled postpartum follow-up, we lack data on about 40% of our population, and we cannot be certain that this group represents the population at large. If women who do not complete postpartum follow-up differ from those who do, our results may be biased in an indeterminate manner. We also do not have information on why or precisely when women discontinued breastfeeding, which would have helped us stratify our findings more precisely. We also use Medicaid status as a proxy for socioeconomic status, which may not truly correlate with income; some women in low-wage jobs may have commercial insurance through their employer and have a household income not much above the Medicaid cutoff. However, this study was undertaken in a time period before the major Medicaid expansion, and anyone on a Medicaid plan would have had an income level not greater than 134% of the Federal Poverty Level, so we can confidently assume that this group is of low SES. If the commercial group also contains low-income women, and income rather than insurance was the true effect, this would have blunted rather than enhanced our observed effect. In addition, we consider the use of Medicaid status to be a clinically useful predictor. While clinicians do not routinely collect household income information from patients, we do always know their insurance status. The ready availability of this information makes it a feasible tool in assessing a patient's breastfeeding risk.
Our study also has several strengths. We have a racially and ethnically diverse cohort, making our results generalizable to many urban obstetric populations. Our population was also evenly divided between Medicaid and commercial insurance. In our clinical setting, these patients are cared for by the same providers in one facility, in contrast with some health systems where “clinic” and “private” populations may receive different care. Our data on breastfeeding were collected as part of routine clinical follow-up and reported patient behavior at the time of the visit. It is therefore less subject to recall or reporting bias, as might be a factor in many survey studies where women are separately contacted and asked about breastfeeding.
These data demonstrate that women on Medicaid insurance are significantly less likely to continue breastfeeding at 6–8 weeks postpartum. While African American women have the overall lowest rates of breastfeeding, non-Hispanic white women on Medicaid are the least likely to breastfeed. Future research should explore these relationships more explicitly. A better understanding of the reasons for these disparities and what influences breastfeeding in these groups will allow for more effective interventions to increase breastfeeding rates in this high-risk population.
Footnotes
Acknowledgments
The findings of this study were reported at the 2015 ACOG Annual Clinical and Scientific Meeting, May 2–6, 2015, in San Francisco, CA.
Disclosure Statement
No competing financial interests exist.